User login
Vitamin D Supplements May Be a Double-Edged Sword
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.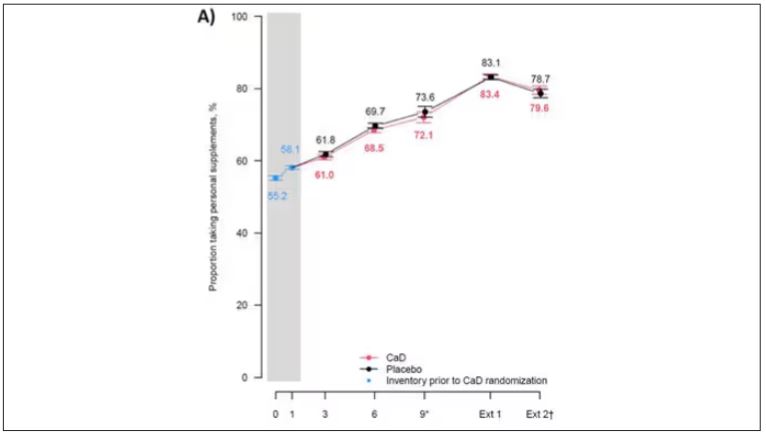
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.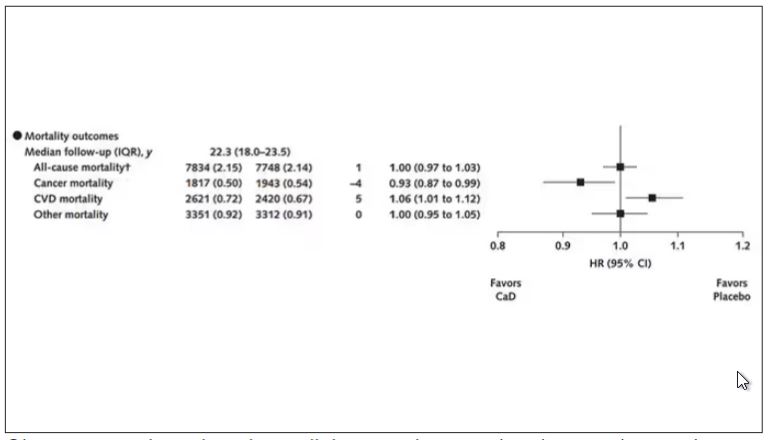
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.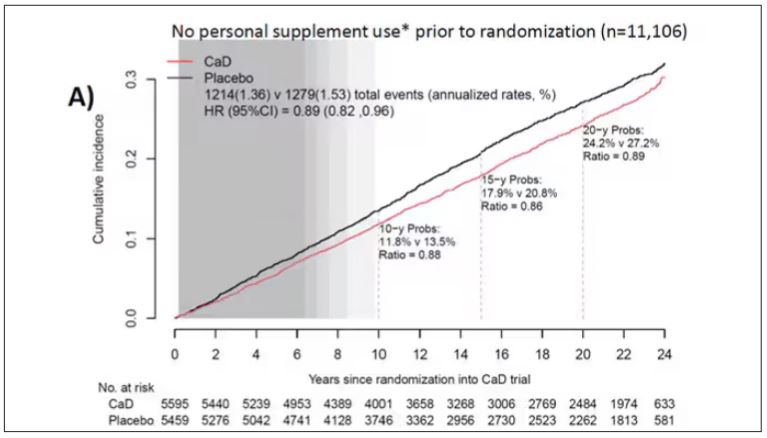
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.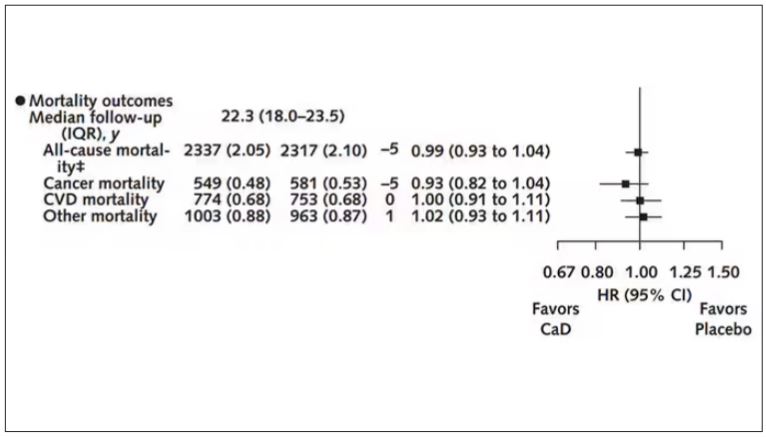
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
Imagine, if you will, the great Cathedral of Our Lady of Correlation. You walk through the majestic oak doors depicting the link between ice cream sales and shark attacks, past the rose window depicting the cardiovascular benefits of red wine, and down the aisles frescoed in dramatic images showing how Facebook usage is associated with less life satisfaction. And then you reach the altar, the holy of holies where, emblazoned in shimmering pyrite, you see the patron saint of this church: vitamin D.
Yes, if you’ve watched this space, then you know that I have little truck with the wildly popular supplement. In all of clinical research, I believe that there is no molecule with stronger data for correlation and weaker data for causation.
Low serum vitamin D levels have been linked to higher risks for heart disease, cancer, falls, COVID, dementia, C diff, and others. And yet, when we do randomized trials of vitamin D supplementation — the thing that can prove that the low level was causally linked to the outcome of interest — we get negative results.
Trials aren’t perfect, of course, and we’ll talk in a moment about a big one that had some issues. But we are at a point where we need to either be vitamin D apologists, saying, “Forget what those lying RCTs tell you and buy this supplement” — an $800 million-a-year industry, by the way — or conclude that vitamin D levels are a convenient marker of various lifestyle factors that are associated with better outcomes: markers of exercise, getting outside, eating a varied diet.
Or perhaps vitamin D supplements have real effects. It’s just that the beneficial effects are matched by the harmful ones. Stay tuned.
The Women’s Health Initiative remains among the largest randomized trials of vitamin D and calcium supplementation ever conducted — and a major contributor to the negative outcomes of vitamin D trials.
But if you dig into the inclusion and exclusion criteria for this trial, you’ll find that individuals were allowed to continue taking vitamins and supplements while they were in the trial, regardless of their randomization status. In fact, the majority took supplements at baseline, and more took supplements over time.
That means, of course, that people in the placebo group, who were getting sugar pills instead of vitamin D and calcium, may have been taking vitamin D and calcium on the side. That would certainly bias the results of the trial toward the null, which is what the primary analyses showed. To wit, the original analysis of the Women’s Health Initiative trial showed no effect of randomization to vitamin D supplementation on improving cancer or cardiovascular outcomes.
But the Women’s Health Initiative trial started 30 years ago. Today, with the benefit of decades of follow-up, we can re-investigate — and perhaps re-litigate — those findings, courtesy of this study, “Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women” appearing in Annals of Internal Medicine.
Dr Cynthia Thomson, of the Mel and Enid Zuckerman College of Public Health at the University of Arizona, and colleagues led this updated analysis focused on two findings that had been hinted at, but not statistically confirmed, in other vitamin D studies: a potential for the supplement to reduce the risk for cancer, and a potential for it to increase the risk for heart disease.
The randomized trial itself only lasted 7 years. What we are seeing in this analysis of 36,282 women is outcomes that happened at any time from randomization to the end of 2023 — around 20 years after the randomization to supplementation stopped. But, the researchers would argue, that’s probably okay. Cancer and heart disease take time to develop; we see lung cancer long after people stop smoking. So a history of consistent vitamin D supplementation may indeed be protective — or harmful.
Here are the top-line results. Those randomized to vitamin D and calcium supplementation had a 7% reduction in the rate of death from cancer, driven primarily by a reduction in colorectal cancer. This was statistically significant. Also statistically significant? Those randomized to supplementation had a 6% increase in the rate of death from cardiovascular disease. Put those findings together and what do you get? Stone-cold nothing, in terms of overall mortality.
Okay, you say, but what about all that supplementation that was happening outside of the context of the trial, biasing our results toward the null?
The researchers finally clue us in.
First of all, I’ll tell you that, yes, people who were supplementing outside of the trial had higher baseline vitamin D levels — a median of 54.5 nmol/L vs 32.8 nmol/L. This may be because they were supplementing with vitamin D, but it could also be because people who take supplements tend to do other healthy things — another correlation to add to the great cathedral.
To get a better view of the real effects of randomization, the authors restricted the analysis to just those who did not use outside supplements. If vitamin D supplements help, then these are the people they should help. This group had about a 11% reduction in the incidence of cancer — statistically significant — and a 7% reduction in cancer mortality that did not meet the bar for statistical significance.
There was no increase in cardiovascular disease among this group. But this small effect on cancer was nowhere near enough to significantly reduce the rate of all-cause mortality.
Among those using supplements, vitamin D supplementation didn’t really move the needle on any outcome.
I know what you’re thinking: How many of these women were vitamin D deficient when we got started? These results may simply be telling us that people who have normal vitamin D levels are fine to go without supplementation.
Nearly three fourths of women who were not taking supplements entered the trial with vitamin D levels below the 50 nmol/L cutoff that the authors suggest would qualify for deficiency. Around half of those who used supplements were deficient. And yet, frustratingly, I could not find data on the effect of randomization to supplementation stratified by baseline vitamin D level. I even reached out to Dr Thomson to ask about this. She replied, “We did not stratify on baseline values because the numbers are too small statistically to test this.” Sorry.
In the meantime, I can tell you that for your “average woman,” vitamin D supplementation likely has no effect on mortality. It might modestly reduce the risk for certain cancers while increasing the risk for heart disease (probably through coronary calcification). So, there might be some room for personalization here. Perhaps women with a strong family history of cancer or other risk factors would do better with supplements, and those with a high risk for heart disease would do worse. Seems like a strategy that could be tested in a clinical trial. But maybe we could ask the participants to give up their extracurricular supplement use before they enter the trial. F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his book, How Medicine Works and When It Doesn’t, is available now.
Long-Term Calcium and Vitamin D: Cancer Deaths Down, CVD Deaths Up in Older Women?
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.

“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.

“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”

Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.

“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.
“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.
“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”
Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.
“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
Some doctors may be scratching their heads over a new analysis reporting that combined calcium and vitamin D (CaD) supplements appear to be associated with a slight 6% increase in cardiovascular (CVD) mortality, a slight 7% decrease in cancer risk, and no effect on osteoporotic fracture in postmenopausal women.
The study, in Annals of Internal Medicine, found no effect of supplementation on all-cause mortality.
The findings emerged from an analysis of more than 20 years’ follow-up data on a randomized trial in postmenopausal women conducted as part of the Women’s Health Initiative (WHI).
Cynthia A. Thomson, PhD, RD, first author and cancer prevention scientist at the Arizona Cancer Center and a professor of health promotion sciences at the University of Arizona in Tucson said the findings recommend individualized assessment of the need for supplements for older women as they consider them in hopes of preventing fractures.
“Evaluate your patients individually and understand that there are some who may benefit from supplementation, for example, in terms of reducing colorectal cancer mortality,” Dr. Thomson said in an interview. The approach should be nuanced. “If you check the adequacy of vitamin D and calcium in their diets, supplementation may not be needed.” She added that supplementation is best considered in the context of a woman’s overall health profile, including risk factors for fracture, heart disease, and cancer, especially colorectal cancer (CRC).
Study Details
The investigators conducted postintervention follow-up of the WHI’s 7-year multicenter randomized intervention trial of CaD vs placebo.
Since existing evidence of long-term health outcomes was limited, the trial, begun in 1999 and closed in 2005, enrolled 36,282 postmenopausal women (mean age 62) with no history of breast or colorectal cancer. They were randomly assigned 1:1 to supplementation with 1000 mg of calcium carbonate (400 mg elemental calcium) plus 400 IU of vitamin D3 daily or placebo, taken twice daily in half doses.
Study outcomes were incidence of CRC, total and invasive breast cancer; disease-specific and all-cause mortality; total CVD; and hip fracture measured through December 2020, with analyses stratified by personal supplement usage.
Cancer. CaD was associated with reduced incident total cancer, CRC, and invasive breast cancer — notably among participants not taking CaD before randomization. Cancer incidence estimates varied widely, the authors noted, when stratified by supplement use before randomization. Noting that CaD seemed to have more cancer-related impact in those without prior supplementation, the authors suggested supplementation may affect cancer biology primarily by augmenting nutrient insufficiency.
An estimated 7% reduction in cancer mortality was observed after a median cumulative follow-up of 22.3 years: 1817 vs 1943 deaths (hazard ratio, 0.93; 95% CI, 0.87-0.99).
CVD. An estimated 6% increase in CVD mortality was seen in the CaD group: 2621 vs 2420 deaths (HR, 1.06; 95% CI, 1.01-1.12). Pretrial supplement users were found to be at higher CVD risk.
Hip fracture. No effect on hip fracture risk was measured, but the authors cautioned that hip fracture and CVD outcomes were available only for a subset of participants, and the effects of calcium alone vs vitamin D alone vs the combination could not be disentangled.
In a small subgroup analysis, some CaD users were seen to respond in terms of bone mineral density but since only 4 of the study’s 40 sites collected such information, the study was underpowered to examine the effect. ”Many other studies, however, show a response to supplementation in women who already have bone mineral deficits,” Dr. Thomson said.
The Calcification Question
One of the possible mechanisms of harm is that high-dose calcium supplements can increase the rate of blood coagulation and promote vascular calcification, said Emma Laing, PhD, RD, director of dietetics at the University of Georgia in Athens and a spokesperson for the Chicago-based Academy of Nutrition and Dietetics.
“Other factors that should be considered when determining a patient’s CVD risk are race, genetic predisposition, medical and social history, response to stress, and lifestyle behaviors, as well as the length of time supplements have been consumed,” added Dr. Laing, who was not involved in the WHI analysis.
“We asked ourselves if CaD supplements might contribute to calcification of the coronary arteries, since some believe this to be the case, although the literature is mixed,” said Dr. Thomson.
“So we did a shorter ancillary study in a small sample of several hundred [women] to see if there was any increase in calcification” and no difference was seen on imaging across the two arms. “However, women who were already on supplements before entering the study seemed to be at higher CVD risk,” she said.
Added study coauthor JoAnn E. Manson, MD, DrPH, chief of the division of preventive medicine at Brigham and Women’s Hospital and professor of women’s health at Harvard Medical School, both in Boston: “With no increase or decrease in coronary artery calcium at the end of the trial, we don’t believe starting or continuing calcium/vitamin D supplements should require screening for coronary artery disease.”
Some randomized trials and systematic reviews, however, have observed an increased risk of CVD in healthy patients on calcium supplements, with one Korean meta-analysis reporting a 15% increase in CVD risk in healthy postmenopausal women taking calcium supplements. Another meta-analysis found a link between calcium supplements and a greater risk of various cardiovascular outcomes, especially myocardial infarction.
Vitamin D Supplementation
As for vitamin D only supplementation, an updated meta-analysis including more than 83,000 individuals showed that it confers no cardiovascular protection and is therefore not indicated for this purpose.
Practice Considerations
Offering an outsider’s perspective, Sarah G. Candler, MD, MPH, an internist in Houston specializing in primary care for older high-risk adults, said: “Unfortunately, this latest study continues the trend of creating more questions than answers. If the adverse outcome of CVD death is a result of supplementation, it is unclear if this is due to the vitamin D, the calcium, or both. And it is unclear if this is dose dependent, time dependent, or due to concurrent risk factors unique to certain populations.
“It is recommended that patients at risk of osteoporosis based on age, sex, medications, and lifestyle be screened for osteoporosis and treated accordingly, including supplementation with CaD,” Dr. Candler said. “It remains unclear whether supplementation with CaD in the absence of osteoporosis and osteopenia is net beneficial or harmful, and at this time I would not recommend it to my patients.”
Added Dr. Manson: “The very small increase seen in cardiovascular mortality wouldn’t be a reason to discontinue supplementation among women who have been advised by their healthcare providers to take these supplements for bone health or other purposes.
“Among those at usual risk of fracture, we recommend trying to obtain adequate calcium and vitamin D from food sources first and to use supplements only for the purpose of filling gaps in intake,” Dr. Manson continued. Overall, the findings support the national recommended dietary allowances for daily calcium intake of 1200 mg and daily vitamin D intake of 600-800 IU among postmenopausal women for maintenance of bone health, she said.
While a 2022 study found that vitamin D supplementation alone did not prevent fractures in healthy adults, other research has shown that a calcium/vitamin D combination is more likely to protect the skeleton.
“Patients at risk for fractures will probably benefit from calcium and/or vitamin D supplementation if they do not meet dietary intake requirements, have malabsorption syndromes, are taking medications that affect nutrient absorption, or if they are older and not regularly exposed to sunlight,” said Dr. Laing. “A combination of biochemical, imaging, functional, and dietary intake data can help determine if a supplement is warranted.”
She stressed that additional research is needed in more diverse populations before changing practice guidelines. “However, doctors should continue to weigh the risks and benefits of prescribing supplements for each patient.”
The WHI program is funded by the National Heart, Lung, and Blood Institute. Dr. Thomson disclosed no competing interests. Dr. Manson reported a relationship with Mars Edge. Multiple authors reported grant support from government funding agencies. The outside commentators had no relevant competing interests to disclose.
FROM ANNALS OF INTERNAL MEDICINE
Nurse-Led Strategy Reduces Cholesterol, BP in HIV
TOPLINE:
A multicomponent strategy of nurse-led communication, home blood pressure monitoring, evidence-based treatment algorithms, and electronic health record tools improved systolic blood pressure (SBP) and non–high-density lipoprotein (non-HDL) cholesterol levels in people living with HIV.
METHODOLOGY:
- Investigators assessed if EXTRA-CVD, a nurse-led multicomponent intervention for preventing cardiovascular diseases (CVD), could effectively improve SBP and non-HDL cholesterol levels in people living with HIV whose viral replication has been controlled effectively using antiretroviral therapy.
- They recruited 297 individuals (median age, 59 years; 20.9% women) from three academic HIV clinics in the United States with an HIV-1 viral load < 200 copies/mL who were diagnosed with both hypertension and hypercholesterolemia.
- Participants were randomly assigned to either the EXTRA-CVD intervention group or a control group comprising individuals who received general prevention education.
- SBP (the primary outcome) was calculated as the mean of two SBP measurements obtained 1 minute apart, and non-HDL cholesterol (the secondary outcome) was calculated as total cholesterol minus HDL cholesterol.
TAKEAWAY:
- Participants in the intervention vs control group reported having significantly lower SBP as early as 4 months after the nurse-led strategy (mean difference, −6.4 mm Hg; P = .002), with the improvements sustaining until 12 months (mean difference, −4.2 mm Hg; P = .04).
- At 12 months, participants in the intervention group showed a 16.9-mg/dL (P < .001) reduction in non-HDL cholesterol levels compared with those in the control group.
- The nurse-led strategy led to a greater reduction in SBP in women with HIV vs men living with HIV (5.9 mm Hg greater SBP difference at 12 months), with the difference being clinically meaningful but not statistically significant.
- This nurse-led strategy did not increase the risk for adverse events in people living with HIV.
IN PRACTICE:
“Although the EXTRA-CVD intervention was limited to BP and cholesterol, nurse-led case management might be beneficial for a range of other primary care conditions in HIV clinics. If HIV clinics choose to implement EXTRA-CVD, they might consider adding staff trained in other chronic comorbidities and/or health promotion activities,” the authors noted.
SOURCE:
This study was led by Christopher T. Longenecker, MD, University of Washington School of Medicine, Seattle, and published online on March 5, 2024, in JAMA Network Open.
LIMITATIONS:
Because this trial was conducted at well-resourced, major academic HIV clinics, the results may not be applicable to other populations, such as smaller community-based clinics or HIV care outside the United States. The sensitivity analyses performed in this study may not have fully accounted for the bias introduced by the differential attrition in the intervention group.
DISCLOSURES:
This study was supported by grants from the National Institutes of Health (NIH). The authors declared receiving grants and personal fees from or having other ties with the NIH and other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
A multicomponent strategy of nurse-led communication, home blood pressure monitoring, evidence-based treatment algorithms, and electronic health record tools improved systolic blood pressure (SBP) and non–high-density lipoprotein (non-HDL) cholesterol levels in people living with HIV.
METHODOLOGY:
- Investigators assessed if EXTRA-CVD, a nurse-led multicomponent intervention for preventing cardiovascular diseases (CVD), could effectively improve SBP and non-HDL cholesterol levels in people living with HIV whose viral replication has been controlled effectively using antiretroviral therapy.
- They recruited 297 individuals (median age, 59 years; 20.9% women) from three academic HIV clinics in the United States with an HIV-1 viral load < 200 copies/mL who were diagnosed with both hypertension and hypercholesterolemia.
- Participants were randomly assigned to either the EXTRA-CVD intervention group or a control group comprising individuals who received general prevention education.
- SBP (the primary outcome) was calculated as the mean of two SBP measurements obtained 1 minute apart, and non-HDL cholesterol (the secondary outcome) was calculated as total cholesterol minus HDL cholesterol.
TAKEAWAY:
- Participants in the intervention vs control group reported having significantly lower SBP as early as 4 months after the nurse-led strategy (mean difference, −6.4 mm Hg; P = .002), with the improvements sustaining until 12 months (mean difference, −4.2 mm Hg; P = .04).
- At 12 months, participants in the intervention group showed a 16.9-mg/dL (P < .001) reduction in non-HDL cholesterol levels compared with those in the control group.
- The nurse-led strategy led to a greater reduction in SBP in women with HIV vs men living with HIV (5.9 mm Hg greater SBP difference at 12 months), with the difference being clinically meaningful but not statistically significant.
- This nurse-led strategy did not increase the risk for adverse events in people living with HIV.
IN PRACTICE:
“Although the EXTRA-CVD intervention was limited to BP and cholesterol, nurse-led case management might be beneficial for a range of other primary care conditions in HIV clinics. If HIV clinics choose to implement EXTRA-CVD, they might consider adding staff trained in other chronic comorbidities and/or health promotion activities,” the authors noted.
SOURCE:
This study was led by Christopher T. Longenecker, MD, University of Washington School of Medicine, Seattle, and published online on March 5, 2024, in JAMA Network Open.
LIMITATIONS:
Because this trial was conducted at well-resourced, major academic HIV clinics, the results may not be applicable to other populations, such as smaller community-based clinics or HIV care outside the United States. The sensitivity analyses performed in this study may not have fully accounted for the bias introduced by the differential attrition in the intervention group.
DISCLOSURES:
This study was supported by grants from the National Institutes of Health (NIH). The authors declared receiving grants and personal fees from or having other ties with the NIH and other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
A multicomponent strategy of nurse-led communication, home blood pressure monitoring, evidence-based treatment algorithms, and electronic health record tools improved systolic blood pressure (SBP) and non–high-density lipoprotein (non-HDL) cholesterol levels in people living with HIV.
METHODOLOGY:
- Investigators assessed if EXTRA-CVD, a nurse-led multicomponent intervention for preventing cardiovascular diseases (CVD), could effectively improve SBP and non-HDL cholesterol levels in people living with HIV whose viral replication has been controlled effectively using antiretroviral therapy.
- They recruited 297 individuals (median age, 59 years; 20.9% women) from three academic HIV clinics in the United States with an HIV-1 viral load < 200 copies/mL who were diagnosed with both hypertension and hypercholesterolemia.
- Participants were randomly assigned to either the EXTRA-CVD intervention group or a control group comprising individuals who received general prevention education.
- SBP (the primary outcome) was calculated as the mean of two SBP measurements obtained 1 minute apart, and non-HDL cholesterol (the secondary outcome) was calculated as total cholesterol minus HDL cholesterol.
TAKEAWAY:
- Participants in the intervention vs control group reported having significantly lower SBP as early as 4 months after the nurse-led strategy (mean difference, −6.4 mm Hg; P = .002), with the improvements sustaining until 12 months (mean difference, −4.2 mm Hg; P = .04).
- At 12 months, participants in the intervention group showed a 16.9-mg/dL (P < .001) reduction in non-HDL cholesterol levels compared with those in the control group.
- The nurse-led strategy led to a greater reduction in SBP in women with HIV vs men living with HIV (5.9 mm Hg greater SBP difference at 12 months), with the difference being clinically meaningful but not statistically significant.
- This nurse-led strategy did not increase the risk for adverse events in people living with HIV.
IN PRACTICE:
“Although the EXTRA-CVD intervention was limited to BP and cholesterol, nurse-led case management might be beneficial for a range of other primary care conditions in HIV clinics. If HIV clinics choose to implement EXTRA-CVD, they might consider adding staff trained in other chronic comorbidities and/or health promotion activities,” the authors noted.
SOURCE:
This study was led by Christopher T. Longenecker, MD, University of Washington School of Medicine, Seattle, and published online on March 5, 2024, in JAMA Network Open.
LIMITATIONS:
Because this trial was conducted at well-resourced, major academic HIV clinics, the results may not be applicable to other populations, such as smaller community-based clinics or HIV care outside the United States. The sensitivity analyses performed in this study may not have fully accounted for the bias introduced by the differential attrition in the intervention group.
DISCLOSURES:
This study was supported by grants from the National Institutes of Health (NIH). The authors declared receiving grants and personal fees from or having other ties with the NIH and other sources.
A version of this article appeared on Medscape.com.
Higher Dietary Niacin Tied to Lower Mortality Risk in MASLD
TOPLINE:
Higher dietary niacin intake is associated with a lower risk for all-cause mortality among people with metabolic dysfunction-associated steatotic liver disease (MASLD), but there is no connection between niacin consumption and cardiovascular disease (CVD) mortality, a recent study suggested.
METHODOLOGY:
- Researchers analyzed data from the National Health and Nutrition Examination Survey (2003-2018) for 4315 adults with MASLD (mean age, 52.5 years; 55%, men; 67%, non-Hispanic White).
- Dietary niacin intake levels were based on two 24-hour dietary recall interviews to report the types and quantities of foods that participants consumed in the 24 hours prior to the interviews.
- Participants were categorized by tertile of dietary niacin intake: Tertile 1 (n = 1440), < 18.4 mg; tertile 2 (n = 1441), 18.5-26.6 mg; and tertile 3 (n = 1434), > 26.7 mg.
TAKEAWAY:
- During a median follow-up of 8.8 years, 566 deaths occurred, of which 197 were attributed to CVD.
- Compared with participants with a niacin intake of 18.4 mg or lower (the lowest tertile), the multivariable-adjusted hazard ratios (HRs) for participants with a niacin intake of 26.7 mg or higher (the highest tertile) were 0.70 for all-cause mortality and 0.65 for CVD mortality.
- For the subgroup with diabetes compared with the reference group (the first tertile), the HR of all-cause mortality in the third tertile was 0.82.
- When the subgroup without diabetes was compared with the reference group, the HR of all-cause mortality in the third tertile was 0.58, suggesting a significant interaction between niacin and diabetes with the risk of all-cause mortality.
- An inverse association between dietary niacin intake and all-cause mortality was seen in sensitivity analyses, when excluding a participant who died within 2 years of follow-up.
IN PRACTICE:
“Higher dietary niacin intake was associated with a lower risk of all-cause mortality,” but not CVD, among individuals with MASLD, and “the dose-response association…needs to be further investigated to determine optimal intake level,” the authors wrote.
SOURCE:
The study, led by Jie Pan, MD, Sun Yat-sen University, Guangzhou, China, was published online in JAMA Network Open.
LIMITATIONS:
Physical activity data were missing and could not be adjusted for. The National Death Index used by the researchers has only “modest” ability to accurately classify CVD mortality, and the dietary data were subject to recall bias.
DISCLOSURES:
One author was supported by a grant from the National Nature Science Foundation of China. No other conflicts of interest were reported.
A version of this article appeared on Medscape.com.
TOPLINE:
Higher dietary niacin intake is associated with a lower risk for all-cause mortality among people with metabolic dysfunction-associated steatotic liver disease (MASLD), but there is no connection between niacin consumption and cardiovascular disease (CVD) mortality, a recent study suggested.
METHODOLOGY:
- Researchers analyzed data from the National Health and Nutrition Examination Survey (2003-2018) for 4315 adults with MASLD (mean age, 52.5 years; 55%, men; 67%, non-Hispanic White).
- Dietary niacin intake levels were based on two 24-hour dietary recall interviews to report the types and quantities of foods that participants consumed in the 24 hours prior to the interviews.
- Participants were categorized by tertile of dietary niacin intake: Tertile 1 (n = 1440), < 18.4 mg; tertile 2 (n = 1441), 18.5-26.6 mg; and tertile 3 (n = 1434), > 26.7 mg.
TAKEAWAY:
- During a median follow-up of 8.8 years, 566 deaths occurred, of which 197 were attributed to CVD.
- Compared with participants with a niacin intake of 18.4 mg or lower (the lowest tertile), the multivariable-adjusted hazard ratios (HRs) for participants with a niacin intake of 26.7 mg or higher (the highest tertile) were 0.70 for all-cause mortality and 0.65 for CVD mortality.
- For the subgroup with diabetes compared with the reference group (the first tertile), the HR of all-cause mortality in the third tertile was 0.82.
- When the subgroup without diabetes was compared with the reference group, the HR of all-cause mortality in the third tertile was 0.58, suggesting a significant interaction between niacin and diabetes with the risk of all-cause mortality.
- An inverse association between dietary niacin intake and all-cause mortality was seen in sensitivity analyses, when excluding a participant who died within 2 years of follow-up.
IN PRACTICE:
“Higher dietary niacin intake was associated with a lower risk of all-cause mortality,” but not CVD, among individuals with MASLD, and “the dose-response association…needs to be further investigated to determine optimal intake level,” the authors wrote.
SOURCE:
The study, led by Jie Pan, MD, Sun Yat-sen University, Guangzhou, China, was published online in JAMA Network Open.
LIMITATIONS:
Physical activity data were missing and could not be adjusted for. The National Death Index used by the researchers has only “modest” ability to accurately classify CVD mortality, and the dietary data were subject to recall bias.
DISCLOSURES:
One author was supported by a grant from the National Nature Science Foundation of China. No other conflicts of interest were reported.
A version of this article appeared on Medscape.com.
TOPLINE:
Higher dietary niacin intake is associated with a lower risk for all-cause mortality among people with metabolic dysfunction-associated steatotic liver disease (MASLD), but there is no connection between niacin consumption and cardiovascular disease (CVD) mortality, a recent study suggested.
METHODOLOGY:
- Researchers analyzed data from the National Health and Nutrition Examination Survey (2003-2018) for 4315 adults with MASLD (mean age, 52.5 years; 55%, men; 67%, non-Hispanic White).
- Dietary niacin intake levels were based on two 24-hour dietary recall interviews to report the types and quantities of foods that participants consumed in the 24 hours prior to the interviews.
- Participants were categorized by tertile of dietary niacin intake: Tertile 1 (n = 1440), < 18.4 mg; tertile 2 (n = 1441), 18.5-26.6 mg; and tertile 3 (n = 1434), > 26.7 mg.
TAKEAWAY:
- During a median follow-up of 8.8 years, 566 deaths occurred, of which 197 were attributed to CVD.
- Compared with participants with a niacin intake of 18.4 mg or lower (the lowest tertile), the multivariable-adjusted hazard ratios (HRs) for participants with a niacin intake of 26.7 mg or higher (the highest tertile) were 0.70 for all-cause mortality and 0.65 for CVD mortality.
- For the subgroup with diabetes compared with the reference group (the first tertile), the HR of all-cause mortality in the third tertile was 0.82.
- When the subgroup without diabetes was compared with the reference group, the HR of all-cause mortality in the third tertile was 0.58, suggesting a significant interaction between niacin and diabetes with the risk of all-cause mortality.
- An inverse association between dietary niacin intake and all-cause mortality was seen in sensitivity analyses, when excluding a participant who died within 2 years of follow-up.
IN PRACTICE:
“Higher dietary niacin intake was associated with a lower risk of all-cause mortality,” but not CVD, among individuals with MASLD, and “the dose-response association…needs to be further investigated to determine optimal intake level,” the authors wrote.
SOURCE:
The study, led by Jie Pan, MD, Sun Yat-sen University, Guangzhou, China, was published online in JAMA Network Open.
LIMITATIONS:
Physical activity data were missing and could not be adjusted for. The National Death Index used by the researchers has only “modest” ability to accurately classify CVD mortality, and the dietary data were subject to recall bias.
DISCLOSURES:
One author was supported by a grant from the National Nature Science Foundation of China. No other conflicts of interest were reported.
A version of this article appeared on Medscape.com.
Hypertension Stable in US, Antihypertensive Med Use Rises
TOPLINE:
Hypertension prevalence remained stable in the United States at 30% after guidelines updated in 2017 lowered the threshold for the condition, while antihypertensive medication use rose about 3%, new research from the Centers for Disease Control and Prevention (CDC) shows.
METHODOLOGY:
- Researchers analyzed data from the Behavioral Risk Factor Surveillance System, a telephone survey of US adults aged 18 years and older.
- Self-reported diagnosed hypertension was defined as an affirmative response to the question, “Have you ever been told by a doctor, nurse, or other health professional that you have high blood pressure?”
- To determine treatment, respondents who answered the first question affirmatively were then asked, “Are you currently taking medicine for your high blood pressure?”
- Hypertension and treatment were assessed by age group (18-44, 45-64, and > 65 years), sex, race, ethnicity, level of education, and state of residence.
TAKEAWAY:
- The final analytic samples for 2017, 2019, and 2021 included 425,417, 392,100, and 410,318 participants, respectively.
- From 2017 to 2021, the overall age-standardized prevalence of hypertension did not change, remaining at almost exactly 30%.
- The age-standardized prevalence of antihypertensive medication use among individuals with hypertension increased by 3.1 percentage points, from 59.8% to 62.9%.
- Increases in medication use were seen in most sociodemographic groups; for example, in 2021, the prevalence was higher among women than among men (68.5% vs 59.4%), among adults aged ≥ 65 years than among those aged 18-44 years (92.5% vs 42.5%), and among Black patients than among White patients (71.3% vs 62%).
- Increases in medication use were also seen by state; use increased in 11 states, ranging from 52.2% in Utah to 72.8% in Mississippi in 2021, and did not decrease significantly in any state.
IN PRACTICE:
“These findings can be used to increase awareness of hypertension and promote lifestyle modifications and antihypertensive medication use to optimize blood pressure control and reduce disparities in prevalence and control,” the authors wrote.
SOURCE:
The study was led by Ahlia Sekkarie, PhD, of CDC’s Division for Heart Disease and Stroke Prevention, and published online in Morbidity and Mortality Weekly Report.
LIMITATIONS:
The study had several limitations. The findings were based on self-report. Median response rates of less than 50% could lead to under- or overestimates of prevalence. Parts of the population, such as those in long-term care facilities or without a telephone, were not included in the analysis. Some demographic categories had small sample sizes; therefore, prevalence changes might not be detectable.
DISCLOSURES:
No specific funding was reported. The authors reported no potential conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Hypertension prevalence remained stable in the United States at 30% after guidelines updated in 2017 lowered the threshold for the condition, while antihypertensive medication use rose about 3%, new research from the Centers for Disease Control and Prevention (CDC) shows.
METHODOLOGY:
- Researchers analyzed data from the Behavioral Risk Factor Surveillance System, a telephone survey of US adults aged 18 years and older.
- Self-reported diagnosed hypertension was defined as an affirmative response to the question, “Have you ever been told by a doctor, nurse, or other health professional that you have high blood pressure?”
- To determine treatment, respondents who answered the first question affirmatively were then asked, “Are you currently taking medicine for your high blood pressure?”
- Hypertension and treatment were assessed by age group (18-44, 45-64, and > 65 years), sex, race, ethnicity, level of education, and state of residence.
TAKEAWAY:
- The final analytic samples for 2017, 2019, and 2021 included 425,417, 392,100, and 410,318 participants, respectively.
- From 2017 to 2021, the overall age-standardized prevalence of hypertension did not change, remaining at almost exactly 30%.
- The age-standardized prevalence of antihypertensive medication use among individuals with hypertension increased by 3.1 percentage points, from 59.8% to 62.9%.
- Increases in medication use were seen in most sociodemographic groups; for example, in 2021, the prevalence was higher among women than among men (68.5% vs 59.4%), among adults aged ≥ 65 years than among those aged 18-44 years (92.5% vs 42.5%), and among Black patients than among White patients (71.3% vs 62%).
- Increases in medication use were also seen by state; use increased in 11 states, ranging from 52.2% in Utah to 72.8% in Mississippi in 2021, and did not decrease significantly in any state.
IN PRACTICE:
“These findings can be used to increase awareness of hypertension and promote lifestyle modifications and antihypertensive medication use to optimize blood pressure control and reduce disparities in prevalence and control,” the authors wrote.
SOURCE:
The study was led by Ahlia Sekkarie, PhD, of CDC’s Division for Heart Disease and Stroke Prevention, and published online in Morbidity and Mortality Weekly Report.
LIMITATIONS:
The study had several limitations. The findings were based on self-report. Median response rates of less than 50% could lead to under- or overestimates of prevalence. Parts of the population, such as those in long-term care facilities or without a telephone, were not included in the analysis. Some demographic categories had small sample sizes; therefore, prevalence changes might not be detectable.
DISCLOSURES:
No specific funding was reported. The authors reported no potential conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Hypertension prevalence remained stable in the United States at 30% after guidelines updated in 2017 lowered the threshold for the condition, while antihypertensive medication use rose about 3%, new research from the Centers for Disease Control and Prevention (CDC) shows.
METHODOLOGY:
- Researchers analyzed data from the Behavioral Risk Factor Surveillance System, a telephone survey of US adults aged 18 years and older.
- Self-reported diagnosed hypertension was defined as an affirmative response to the question, “Have you ever been told by a doctor, nurse, or other health professional that you have high blood pressure?”
- To determine treatment, respondents who answered the first question affirmatively were then asked, “Are you currently taking medicine for your high blood pressure?”
- Hypertension and treatment were assessed by age group (18-44, 45-64, and > 65 years), sex, race, ethnicity, level of education, and state of residence.
TAKEAWAY:
- The final analytic samples for 2017, 2019, and 2021 included 425,417, 392,100, and 410,318 participants, respectively.
- From 2017 to 2021, the overall age-standardized prevalence of hypertension did not change, remaining at almost exactly 30%.
- The age-standardized prevalence of antihypertensive medication use among individuals with hypertension increased by 3.1 percentage points, from 59.8% to 62.9%.
- Increases in medication use were seen in most sociodemographic groups; for example, in 2021, the prevalence was higher among women than among men (68.5% vs 59.4%), among adults aged ≥ 65 years than among those aged 18-44 years (92.5% vs 42.5%), and among Black patients than among White patients (71.3% vs 62%).
- Increases in medication use were also seen by state; use increased in 11 states, ranging from 52.2% in Utah to 72.8% in Mississippi in 2021, and did not decrease significantly in any state.
IN PRACTICE:
“These findings can be used to increase awareness of hypertension and promote lifestyle modifications and antihypertensive medication use to optimize blood pressure control and reduce disparities in prevalence and control,” the authors wrote.
SOURCE:
The study was led by Ahlia Sekkarie, PhD, of CDC’s Division for Heart Disease and Stroke Prevention, and published online in Morbidity and Mortality Weekly Report.
LIMITATIONS:
The study had several limitations. The findings were based on self-report. Median response rates of less than 50% could lead to under- or overestimates of prevalence. Parts of the population, such as those in long-term care facilities or without a telephone, were not included in the analysis. Some demographic categories had small sample sizes; therefore, prevalence changes might not be detectable.
DISCLOSURES:
No specific funding was reported. The authors reported no potential conflicts of interest.
A version of this article appeared on Medscape.com.
Smoking Cessation Before Age 40 Years Brings Great Benefits
Chronic smoking remains a major cause of premature mortality on a global scale. Despite intensified efforts to combat this scourge, a quarter of deaths among middle-aged adults in Europe and North America are attributed to it. However, over the past decades, antismoking campaigns have borne fruit, and many smokers have quit before the age of 40 years, enabling some case-control studies.
Among those abstainers who made the right choice, the excess mortality attributable to smoking over a lifetime would be reduced by 90% compared with controls who continued smoking. The estimated benefit is clear, but the analysis lacks nuance. Is smoking cessation beneficial even at older ages? If so, is the effect measurable in terms of magnitude and speed of the effect? An article published online in The New England Journal of Medicine Evidence provided some answers to these questions.
Four-Cohort Meta-Analysis
The study was a meta-analysis of individual data collected within four national cohort studies that were linked to each country’s death registry. Two of these studies were nationally representative. The National Health Interview Survey involved a sample of US citizens living in the community, aged 20-79 years, who were included annually in the cohort between 1997 and 2018. The second, the Canadian Community Health Survey, included subjects in the same age group, with samples analyzed between 2000 and 2014.
In Norway, three cohort studies conducted between 1974 and 2003, in which participants aged 25-79 years were included, were combined to form the Norwegian Health Screening Survey. These were the Counties Study (1974-1988), the 40 Years Study (1985-1999), and the Cohort of Norway (1994-2003), respectively. The fourth cohort was established through recruitment via the UK Biobank, with adults aged 40-73 years invited to participate in the survey. The data analysis ultimately covered a relatively heterogeneous total population of 1.48 million adults, all from high-income countries and followed for 15 years. It relied on the Cox proportional hazards model applied to each study, considering smoker vs nonsmoker status, as well as the time elapsed since smoking cessation (less than 3 years, between 3 and 9 years, or at least 10 years). Statistical adjustments made in the context of multivariate Cox analysis considered age, education, alcohol consumption, and obesity.
Excess Mortality Confirmed
At the end of follow-up, 122,697 deaths were recorded. The comparison of smokers and nonsmokers confirmed smoking-related excess mortality, with adjusted hazard ratios (HRs) estimated at 2.80 for women and 2.70 for men. Smoking shortened life expectancy in the 40- to 79-year-age group by 12 years for women and 13 years for men, in terms of overall mortality. In terms of smoking-attributable specific mortality, the corresponding figures reached 24 and 26 years, respectively. Respiratory diseases ranked highest in both sexes (HR, 7.6 for women and 6.3 for men), followed by cardiovascular diseases (HR, 3.1 for women and 2.9 for men) and cancers (HR, 2.8 for women and 3.1 for men).
The Earlier, the Better
Smoking cessation halves overall excess mortality. Above all, quitting before age 40 years brings overall mortality back to the level of nonsmokers as early as the third year after quitting. The excess mortality decreases even more as the cessation period is prolonged, even after age 40 years. Thus, cessation ≥ 10 years in smokers aged 40-49 years almost cancels out overall excess mortality (-99% in women, -96% in men). The trend is almost as favorable in the older age group (50-59 years), with corresponding figures of -95% and -92%, respectively.
Long-term survival increases in the early years after cessation, especially if it occurs at a younger age, but the benefit remains tangible even in older smokers. Thus, cessation of less than 3 years, effective in patients aged 50-59 years, reduces overall excess mortality by 63% in women and 54% in men. In patients aged 60-79 years, the figures are -40% and -33%, respectively.
Naturally, the earlier the cessation, the greater the number of years gained. It is 12 years for cessation before age 40 years, reduced to 6 years for cessation between 40 and 49 years, and 2.5 years when it is even later (50-59 years). These quantitative results are approximate, given the methodology (a meta-analysis) and some heterogeneity in the studies, as well as the multitude of potential confounding factors that have not all been considered. Nevertheless, the results probably contain a kernel of truth, and their optimistic implications should be highlighted to encourage smokers to abstain, even older ones. Better late than never, even if the benefit of cessation is maximal when it occurs as early as possible, knowing that a minimum of 3 years of cessation would be sufficient to gain years of life.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Chronic smoking remains a major cause of premature mortality on a global scale. Despite intensified efforts to combat this scourge, a quarter of deaths among middle-aged adults in Europe and North America are attributed to it. However, over the past decades, antismoking campaigns have borne fruit, and many smokers have quit before the age of 40 years, enabling some case-control studies.
Among those abstainers who made the right choice, the excess mortality attributable to smoking over a lifetime would be reduced by 90% compared with controls who continued smoking. The estimated benefit is clear, but the analysis lacks nuance. Is smoking cessation beneficial even at older ages? If so, is the effect measurable in terms of magnitude and speed of the effect? An article published online in The New England Journal of Medicine Evidence provided some answers to these questions.
Four-Cohort Meta-Analysis
The study was a meta-analysis of individual data collected within four national cohort studies that were linked to each country’s death registry. Two of these studies were nationally representative. The National Health Interview Survey involved a sample of US citizens living in the community, aged 20-79 years, who were included annually in the cohort between 1997 and 2018. The second, the Canadian Community Health Survey, included subjects in the same age group, with samples analyzed between 2000 and 2014.
In Norway, three cohort studies conducted between 1974 and 2003, in which participants aged 25-79 years were included, were combined to form the Norwegian Health Screening Survey. These were the Counties Study (1974-1988), the 40 Years Study (1985-1999), and the Cohort of Norway (1994-2003), respectively. The fourth cohort was established through recruitment via the UK Biobank, with adults aged 40-73 years invited to participate in the survey. The data analysis ultimately covered a relatively heterogeneous total population of 1.48 million adults, all from high-income countries and followed for 15 years. It relied on the Cox proportional hazards model applied to each study, considering smoker vs nonsmoker status, as well as the time elapsed since smoking cessation (less than 3 years, between 3 and 9 years, or at least 10 years). Statistical adjustments made in the context of multivariate Cox analysis considered age, education, alcohol consumption, and obesity.
Excess Mortality Confirmed
At the end of follow-up, 122,697 deaths were recorded. The comparison of smokers and nonsmokers confirmed smoking-related excess mortality, with adjusted hazard ratios (HRs) estimated at 2.80 for women and 2.70 for men. Smoking shortened life expectancy in the 40- to 79-year-age group by 12 years for women and 13 years for men, in terms of overall mortality. In terms of smoking-attributable specific mortality, the corresponding figures reached 24 and 26 years, respectively. Respiratory diseases ranked highest in both sexes (HR, 7.6 for women and 6.3 for men), followed by cardiovascular diseases (HR, 3.1 for women and 2.9 for men) and cancers (HR, 2.8 for women and 3.1 for men).
The Earlier, the Better
Smoking cessation halves overall excess mortality. Above all, quitting before age 40 years brings overall mortality back to the level of nonsmokers as early as the third year after quitting. The excess mortality decreases even more as the cessation period is prolonged, even after age 40 years. Thus, cessation ≥ 10 years in smokers aged 40-49 years almost cancels out overall excess mortality (-99% in women, -96% in men). The trend is almost as favorable in the older age group (50-59 years), with corresponding figures of -95% and -92%, respectively.
Long-term survival increases in the early years after cessation, especially if it occurs at a younger age, but the benefit remains tangible even in older smokers. Thus, cessation of less than 3 years, effective in patients aged 50-59 years, reduces overall excess mortality by 63% in women and 54% in men. In patients aged 60-79 years, the figures are -40% and -33%, respectively.
Naturally, the earlier the cessation, the greater the number of years gained. It is 12 years for cessation before age 40 years, reduced to 6 years for cessation between 40 and 49 years, and 2.5 years when it is even later (50-59 years). These quantitative results are approximate, given the methodology (a meta-analysis) and some heterogeneity in the studies, as well as the multitude of potential confounding factors that have not all been considered. Nevertheless, the results probably contain a kernel of truth, and their optimistic implications should be highlighted to encourage smokers to abstain, even older ones. Better late than never, even if the benefit of cessation is maximal when it occurs as early as possible, knowing that a minimum of 3 years of cessation would be sufficient to gain years of life.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Chronic smoking remains a major cause of premature mortality on a global scale. Despite intensified efforts to combat this scourge, a quarter of deaths among middle-aged adults in Europe and North America are attributed to it. However, over the past decades, antismoking campaigns have borne fruit, and many smokers have quit before the age of 40 years, enabling some case-control studies.
Among those abstainers who made the right choice, the excess mortality attributable to smoking over a lifetime would be reduced by 90% compared with controls who continued smoking. The estimated benefit is clear, but the analysis lacks nuance. Is smoking cessation beneficial even at older ages? If so, is the effect measurable in terms of magnitude and speed of the effect? An article published online in The New England Journal of Medicine Evidence provided some answers to these questions.
Four-Cohort Meta-Analysis
The study was a meta-analysis of individual data collected within four national cohort studies that were linked to each country’s death registry. Two of these studies were nationally representative. The National Health Interview Survey involved a sample of US citizens living in the community, aged 20-79 years, who were included annually in the cohort between 1997 and 2018. The second, the Canadian Community Health Survey, included subjects in the same age group, with samples analyzed between 2000 and 2014.
In Norway, three cohort studies conducted between 1974 and 2003, in which participants aged 25-79 years were included, were combined to form the Norwegian Health Screening Survey. These were the Counties Study (1974-1988), the 40 Years Study (1985-1999), and the Cohort of Norway (1994-2003), respectively. The fourth cohort was established through recruitment via the UK Biobank, with adults aged 40-73 years invited to participate in the survey. The data analysis ultimately covered a relatively heterogeneous total population of 1.48 million adults, all from high-income countries and followed for 15 years. It relied on the Cox proportional hazards model applied to each study, considering smoker vs nonsmoker status, as well as the time elapsed since smoking cessation (less than 3 years, between 3 and 9 years, or at least 10 years). Statistical adjustments made in the context of multivariate Cox analysis considered age, education, alcohol consumption, and obesity.
Excess Mortality Confirmed
At the end of follow-up, 122,697 deaths were recorded. The comparison of smokers and nonsmokers confirmed smoking-related excess mortality, with adjusted hazard ratios (HRs) estimated at 2.80 for women and 2.70 for men. Smoking shortened life expectancy in the 40- to 79-year-age group by 12 years for women and 13 years for men, in terms of overall mortality. In terms of smoking-attributable specific mortality, the corresponding figures reached 24 and 26 years, respectively. Respiratory diseases ranked highest in both sexes (HR, 7.6 for women and 6.3 for men), followed by cardiovascular diseases (HR, 3.1 for women and 2.9 for men) and cancers (HR, 2.8 for women and 3.1 for men).
The Earlier, the Better
Smoking cessation halves overall excess mortality. Above all, quitting before age 40 years brings overall mortality back to the level of nonsmokers as early as the third year after quitting. The excess mortality decreases even more as the cessation period is prolonged, even after age 40 years. Thus, cessation ≥ 10 years in smokers aged 40-49 years almost cancels out overall excess mortality (-99% in women, -96% in men). The trend is almost as favorable in the older age group (50-59 years), with corresponding figures of -95% and -92%, respectively.
Long-term survival increases in the early years after cessation, especially if it occurs at a younger age, but the benefit remains tangible even in older smokers. Thus, cessation of less than 3 years, effective in patients aged 50-59 years, reduces overall excess mortality by 63% in women and 54% in men. In patients aged 60-79 years, the figures are -40% and -33%, respectively.
Naturally, the earlier the cessation, the greater the number of years gained. It is 12 years for cessation before age 40 years, reduced to 6 years for cessation between 40 and 49 years, and 2.5 years when it is even later (50-59 years). These quantitative results are approximate, given the methodology (a meta-analysis) and some heterogeneity in the studies, as well as the multitude of potential confounding factors that have not all been considered. Nevertheless, the results probably contain a kernel of truth, and their optimistic implications should be highlighted to encourage smokers to abstain, even older ones. Better late than never, even if the benefit of cessation is maximal when it occurs as early as possible, knowing that a minimum of 3 years of cessation would be sufficient to gain years of life.
This story was translated from JIM, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
How Does Snoring Affect Cardiovascular Health?
Snoring is a common disorder that affects 20%-40% of the general population. The mechanism of snoring is the vibration of anatomical structures in the pharyngeal airways. The flutter of the soft palate explains the harsh aspect of the snoring sound, which occurs during natural sleep or drug-induced sleep. The presentation of snoring may vary throughout the night or between nights, with a subjective, and therefore inconsistent, assessment of its loudness.
Objective evaluation of snoring is important for clinical decision-making and predicting the effect of therapeutic interventions. It also provides information regarding the site and degree of upper airway obstruction. Snoring is one of the main features of sleep-disordered breathing, including hypopnea events, which reflect partial upper airway obstruction.
Obstructive sleep apnea (OSA) is characterized by episodes of complete (apnea) or partial (hypopnea) collapse of the upper airways with associated oxygen desaturation or awakening from sleep. Most patients with OSA snore loudly almost every night. However, in the Sleep Heart Health Study, one-third of participants with OSA reported no snoring, while one-third of snoring participants did not meet the criteria for OSA. Therefore, subjective assessments of snoring (self-reported) may not be sufficiently reliable to assess its potential impact on cardiovascular (CV) health outcomes.
CV Effects
OSA has been hypothesized as a modifiable risk factor for CV diseases (CVD), including hypertension, coronary artery disease (CAD), atrial fibrillation, heart failure, and stroke, primarily because of the results of traditional observational studies. Snoring is reported as a symptom of the early stage of OSA and has also been associated with a higher risk for CVD. However, establishing causality based on observational studies is difficult because of residual confounding from unknown or unmeasured factors and reverse causality (i.e., the scenario in which CVD increases the risk for OSA or snoring). A Mendelian randomization study, using the natural random allocation of genetic variants as instruments capable of producing results analogous to those of randomized controlled trials, suggested that OSA and snoring increase the risk for hypertension and CAD, with associations partly driven by body mass index (BMI). Conversely, no evidence was found that CVD causally influenced OSA or snoring.
Snoring has been associated with multiple subclinical markers of CV pathology, including high blood pressure, and loud snoring can interfere with restorative sleep and contribute to the risk for hypertension and other adverse outcomes in snorers. However, evidence on the associations between snoring and CV health outcomes remains limited and is primarily based on subjective assessments of snoring or small clinical samples with objective assessments of snoring for only 1 night.
Snoring and Hypertension
A study of 12,287 middle-aged patients (age, 50 years) who were predominantly males (88%) and generally overweight (BMI, 28 kg/m2) determined the prevalence of snoring and its association with the prevalence of hypertension using objective evaluation of snoring over multiple nights and multiple daytime blood pressure measurements. The findings included the following observations:
An increase in snoring duration was associated with a 3-mmHg increase in systolic (SBP) and a 4 mmHg increase in diastolic blood pressure (DBP) in patients with frequent and regular snoring, compared with those with infrequent snoring, regardless of age, BMI, sex, and estimated apnea/hypopnea index.
The association between severe OSA alone and blood pressure had an effect size similar to that of the association between snoring alone and blood pressure. In a model where OSA severity was classified and snoring duration was stratified into quartiles, severe OSA without snoring was associated with 3.6 mmHg higher SBP and 3.5 mmHg higher DBP, compared with the absence of snoring or OSA. Participants without OSA but with intense snoring (4th quartile) had 3.8 mmHg higher SBP and 4.5 mmHg higher DBP compared with participants without nighttime apnea or snoring.
Snoring was significantly associated with uncontrolled hypertension. There was a 20% increase in the probability of uncontrolled hypertension in subjects aged > 50 years with obesity and a 98% increase in subjects aged ≤ 50 years with normal BMI.
Duration of snoring was associated with an 87% increase in the likelihood of uncontrolled hypertension.
Implications for Practice
This study indicates that 15% of a predominantly overweight male population snore for > 20% of the night and about 10% of these subjects without nighttime apnea snore for > 12% of the night.
Regular nighttime snoring is associated with elevated blood pressure and uncontrolled hypertension, regardless of the presence or severity of OSA.
Physicians must be aware of the potential consequences of snoring on the risk for hypertension, and these results highlight the need to consider snoring in clinical care and in the management of sleep problems, especially in the context of managing arterial hypertension.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Snoring is a common disorder that affects 20%-40% of the general population. The mechanism of snoring is the vibration of anatomical structures in the pharyngeal airways. The flutter of the soft palate explains the harsh aspect of the snoring sound, which occurs during natural sleep or drug-induced sleep. The presentation of snoring may vary throughout the night or between nights, with a subjective, and therefore inconsistent, assessment of its loudness.
Objective evaluation of snoring is important for clinical decision-making and predicting the effect of therapeutic interventions. It also provides information regarding the site and degree of upper airway obstruction. Snoring is one of the main features of sleep-disordered breathing, including hypopnea events, which reflect partial upper airway obstruction.
Obstructive sleep apnea (OSA) is characterized by episodes of complete (apnea) or partial (hypopnea) collapse of the upper airways with associated oxygen desaturation or awakening from sleep. Most patients with OSA snore loudly almost every night. However, in the Sleep Heart Health Study, one-third of participants with OSA reported no snoring, while one-third of snoring participants did not meet the criteria for OSA. Therefore, subjective assessments of snoring (self-reported) may not be sufficiently reliable to assess its potential impact on cardiovascular (CV) health outcomes.
CV Effects
OSA has been hypothesized as a modifiable risk factor for CV diseases (CVD), including hypertension, coronary artery disease (CAD), atrial fibrillation, heart failure, and stroke, primarily because of the results of traditional observational studies. Snoring is reported as a symptom of the early stage of OSA and has also been associated with a higher risk for CVD. However, establishing causality based on observational studies is difficult because of residual confounding from unknown or unmeasured factors and reverse causality (i.e., the scenario in which CVD increases the risk for OSA or snoring). A Mendelian randomization study, using the natural random allocation of genetic variants as instruments capable of producing results analogous to those of randomized controlled trials, suggested that OSA and snoring increase the risk for hypertension and CAD, with associations partly driven by body mass index (BMI). Conversely, no evidence was found that CVD causally influenced OSA or snoring.
Snoring has been associated with multiple subclinical markers of CV pathology, including high blood pressure, and loud snoring can interfere with restorative sleep and contribute to the risk for hypertension and other adverse outcomes in snorers. However, evidence on the associations between snoring and CV health outcomes remains limited and is primarily based on subjective assessments of snoring or small clinical samples with objective assessments of snoring for only 1 night.
Snoring and Hypertension
A study of 12,287 middle-aged patients (age, 50 years) who were predominantly males (88%) and generally overweight (BMI, 28 kg/m2) determined the prevalence of snoring and its association with the prevalence of hypertension using objective evaluation of snoring over multiple nights and multiple daytime blood pressure measurements. The findings included the following observations:
An increase in snoring duration was associated with a 3-mmHg increase in systolic (SBP) and a 4 mmHg increase in diastolic blood pressure (DBP) in patients with frequent and regular snoring, compared with those with infrequent snoring, regardless of age, BMI, sex, and estimated apnea/hypopnea index.
The association between severe OSA alone and blood pressure had an effect size similar to that of the association between snoring alone and blood pressure. In a model where OSA severity was classified and snoring duration was stratified into quartiles, severe OSA without snoring was associated with 3.6 mmHg higher SBP and 3.5 mmHg higher DBP, compared with the absence of snoring or OSA. Participants without OSA but with intense snoring (4th quartile) had 3.8 mmHg higher SBP and 4.5 mmHg higher DBP compared with participants without nighttime apnea or snoring.
Snoring was significantly associated with uncontrolled hypertension. There was a 20% increase in the probability of uncontrolled hypertension in subjects aged > 50 years with obesity and a 98% increase in subjects aged ≤ 50 years with normal BMI.
Duration of snoring was associated with an 87% increase in the likelihood of uncontrolled hypertension.
Implications for Practice
This study indicates that 15% of a predominantly overweight male population snore for > 20% of the night and about 10% of these subjects without nighttime apnea snore for > 12% of the night.
Regular nighttime snoring is associated with elevated blood pressure and uncontrolled hypertension, regardless of the presence or severity of OSA.
Physicians must be aware of the potential consequences of snoring on the risk for hypertension, and these results highlight the need to consider snoring in clinical care and in the management of sleep problems, especially in the context of managing arterial hypertension.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Snoring is a common disorder that affects 20%-40% of the general population. The mechanism of snoring is the vibration of anatomical structures in the pharyngeal airways. The flutter of the soft palate explains the harsh aspect of the snoring sound, which occurs during natural sleep or drug-induced sleep. The presentation of snoring may vary throughout the night or between nights, with a subjective, and therefore inconsistent, assessment of its loudness.
Objective evaluation of snoring is important for clinical decision-making and predicting the effect of therapeutic interventions. It also provides information regarding the site and degree of upper airway obstruction. Snoring is one of the main features of sleep-disordered breathing, including hypopnea events, which reflect partial upper airway obstruction.
Obstructive sleep apnea (OSA) is characterized by episodes of complete (apnea) or partial (hypopnea) collapse of the upper airways with associated oxygen desaturation or awakening from sleep. Most patients with OSA snore loudly almost every night. However, in the Sleep Heart Health Study, one-third of participants with OSA reported no snoring, while one-third of snoring participants did not meet the criteria for OSA. Therefore, subjective assessments of snoring (self-reported) may not be sufficiently reliable to assess its potential impact on cardiovascular (CV) health outcomes.
CV Effects
OSA has been hypothesized as a modifiable risk factor for CV diseases (CVD), including hypertension, coronary artery disease (CAD), atrial fibrillation, heart failure, and stroke, primarily because of the results of traditional observational studies. Snoring is reported as a symptom of the early stage of OSA and has also been associated with a higher risk for CVD. However, establishing causality based on observational studies is difficult because of residual confounding from unknown or unmeasured factors and reverse causality (i.e., the scenario in which CVD increases the risk for OSA or snoring). A Mendelian randomization study, using the natural random allocation of genetic variants as instruments capable of producing results analogous to those of randomized controlled trials, suggested that OSA and snoring increase the risk for hypertension and CAD, with associations partly driven by body mass index (BMI). Conversely, no evidence was found that CVD causally influenced OSA or snoring.
Snoring has been associated with multiple subclinical markers of CV pathology, including high blood pressure, and loud snoring can interfere with restorative sleep and contribute to the risk for hypertension and other adverse outcomes in snorers. However, evidence on the associations between snoring and CV health outcomes remains limited and is primarily based on subjective assessments of snoring or small clinical samples with objective assessments of snoring for only 1 night.
Snoring and Hypertension
A study of 12,287 middle-aged patients (age, 50 years) who were predominantly males (88%) and generally overweight (BMI, 28 kg/m2) determined the prevalence of snoring and its association with the prevalence of hypertension using objective evaluation of snoring over multiple nights and multiple daytime blood pressure measurements. The findings included the following observations:
An increase in snoring duration was associated with a 3-mmHg increase in systolic (SBP) and a 4 mmHg increase in diastolic blood pressure (DBP) in patients with frequent and regular snoring, compared with those with infrequent snoring, regardless of age, BMI, sex, and estimated apnea/hypopnea index.
The association between severe OSA alone and blood pressure had an effect size similar to that of the association between snoring alone and blood pressure. In a model where OSA severity was classified and snoring duration was stratified into quartiles, severe OSA without snoring was associated with 3.6 mmHg higher SBP and 3.5 mmHg higher DBP, compared with the absence of snoring or OSA. Participants without OSA but with intense snoring (4th quartile) had 3.8 mmHg higher SBP and 4.5 mmHg higher DBP compared with participants without nighttime apnea or snoring.
Snoring was significantly associated with uncontrolled hypertension. There was a 20% increase in the probability of uncontrolled hypertension in subjects aged > 50 years with obesity and a 98% increase in subjects aged ≤ 50 years with normal BMI.
Duration of snoring was associated with an 87% increase in the likelihood of uncontrolled hypertension.
Implications for Practice
This study indicates that 15% of a predominantly overweight male population snore for > 20% of the night and about 10% of these subjects without nighttime apnea snore for > 12% of the night.
Regular nighttime snoring is associated with elevated blood pressure and uncontrolled hypertension, regardless of the presence or severity of OSA.
Physicians must be aware of the potential consequences of snoring on the risk for hypertension, and these results highlight the need to consider snoring in clinical care and in the management of sleep problems, especially in the context of managing arterial hypertension.
This story was translated from Univadis Italy, which is part of the Medscape professional network, using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Plastic in Carotid Plaques Increased Risk of CV Event, Death
According to a new study, patients found to have microplastics and nanoplastics in their carotid artery plaque had a higher risk for death or major cardiovascular events compared with patients who had plaques where particles were not found.
, study coauthor Antonio Ceriello, MD, IRCCS MultiMedica, Milan, told this news organization.
“I believe we have demonstrated that plastics are a new risk factor for cardiovascular disease,” he added. And while plastics may have made our lives easier in many respects, it appears that the price we are paying for that is a shortening of our lives. That is not a good balance.”
The trial involved 304 patients undergoing carotid endarterectomy for asymptomatic carotid artery disease, whose excised plaque specimens were analyzed for the presence of microplastics and nanoplastics, ultimately found in almost 60% of patients.
After a mean follow-up of 34 months, patients in whom microplastics and nanoplastics were detected within the atheroma had a 4.5 times higher risk for the composite endpoint of all cause death, myocardial infarction, or stroke than those in whom these substances were not detected (hazard ratio, 4.53; 95% CI, 2.00-10.27; P < .001).
The study, led by Raffaele Marfella, MD, University of Campania Luigi Vanvitelli, Naples, Italy, was published in The New England Journal of Medicine on March 7, 2024.
The researchers say the study does not prove causality, and many other unmeasured confounding factors could have contributed to the findings.
However, Dr. Ceriello noted that many important risk factors such as diabetes, hypertension, and dyslipidemia, were controlled for.
“In this study, all the patients involved were at high risk of cardiovascular events and they were well treated with statins and antithrombotics, so the relationship between the presence of plastic particles in plaque and cardiovascular events is seen on top of good preventive therapy,” he said.
“While we cannot say for sure that we have shown a causal relationship, we found a large effect and there is a great deal of literature than supports this. We know that plastic particles can penetrate cells and act at the mitochondrial level to increase free radical production and produce chronic inflammation which is the basis for atherosclerosis,” Dr. Ceriello added.
He believes there is only one approach to addressing this issue, and that is to reduce the amount of plastic in the environment.
“Plastic is everywhere — in water pipes, in the ocean. We are hoping that this study will increase the push for government to act on this. This is even more important for the long-term health of our children, who will be exposed to high levels of plastics for the whole of their lives,” he said.
‘Strongly Suggestive of a Causal Relationship’
Commenting for this news organization, Philip J. Landrigan, MD, author of an editorial accompanying publication of the study in the NEJM, described the link as “strongly suggestive.”
“Because this was just a single observational study, it doesn’t prove cause and effect, but I think this is strongly suggestive of a causal relationship,” he said. “While there may be some other confounding factors at play, it is hard for me to imagine that these could account for a hazard ratio of 4.5 — that is a large and alarming increase in just 3 years.”
Dr. Landrigan, who is director of the Program for Global Public Health and the Common Good, Boston College, points out that although it is not known what other exposures may have contributed to the adverse outcomes in patients in this study, the finding of microplastics and nanoplastics in plaque tissue is itself a breakthrough discovery that raises a series of urgent questions. These include: “Should exposure to microplastics and nanoplastics be considered a cardiovascular risk factor? What organs in addition to the heart may be at risk? How can we reduce exposure?”
Dr. Landrigan said he was not surprised that plastic particles had been found in carotid plaques. “Previous studies have found microplastics in other tissues including the lungs, colon and placenta. Now they have turned up in the vessel wall,” he said. “But what is really striking about this study is that it suggests the presence of these plastic particles is causing serious harm.”
He says this should be a wake-up call. “It is telling us that we need to worry about the amount of plastic in our environment. And it is not something that’s going to be a problem down the line — it is affecting us now.”
Dr. Landrigan explained that plastic particles are taken into the body predominantly by ingestion, which could include drinking from plastic bottles or eating food wrapped in plastic. He said it is particularly damaging to use plastic containers to heat food in the microwave, as heating plastic up drives particles into the food. “That will really increase exposure.”
He noted that plastics are often already in the food itself, especially seafood.
“Plastics are dumped in the ocean, they break down and get picked up by the fish. Especially if you eat fish at the top of the food chain like tuna, or if you eat oysters or mussels that are filter feeders, you are more likely to ingest microplastics.”
Dr. Landrigan said he would not advise against eating fish in general, however. “Maybe tuna or other predatory fish may be an issue, but fish in general are good for us, and fish like salmon which have a mainly vegetarian diet are probably safer in this regard.”
The other route is inhalation, with these small plastic particles being widely present in the air, from sources such as vehicle tires becoming abraded from running along the highway.
While it is impossible to avoid taking in plastic completely, Dr. Landrigan says individuals can make efforts to reduce their exposure.
“People can make intelligent choices in their homes about what they purchase for themselves and their families, and they can act in their local environments and workplace to try and reduce plastics.”
He noted that 40% of all plastic currently being made is single use plastic, and that percentage is growing, with global production of plastic on track to double by 2040 and triple by 2060, and most of this rapid growth being single use plastic.
“We are all members of the broader society, and we need to become educated about the plastic situation and lobby our elected officials to come up with a good strong legally binding treaty that will place a cap on plastic production,” Dr. Landrigan said.
A version of this article appeared on Medscape.com.
According to a new study, patients found to have microplastics and nanoplastics in their carotid artery plaque had a higher risk for death or major cardiovascular events compared with patients who had plaques where particles were not found.
, study coauthor Antonio Ceriello, MD, IRCCS MultiMedica, Milan, told this news organization.
“I believe we have demonstrated that plastics are a new risk factor for cardiovascular disease,” he added. And while plastics may have made our lives easier in many respects, it appears that the price we are paying for that is a shortening of our lives. That is not a good balance.”
The trial involved 304 patients undergoing carotid endarterectomy for asymptomatic carotid artery disease, whose excised plaque specimens were analyzed for the presence of microplastics and nanoplastics, ultimately found in almost 60% of patients.
After a mean follow-up of 34 months, patients in whom microplastics and nanoplastics were detected within the atheroma had a 4.5 times higher risk for the composite endpoint of all cause death, myocardial infarction, or stroke than those in whom these substances were not detected (hazard ratio, 4.53; 95% CI, 2.00-10.27; P < .001).
The study, led by Raffaele Marfella, MD, University of Campania Luigi Vanvitelli, Naples, Italy, was published in The New England Journal of Medicine on March 7, 2024.
The researchers say the study does not prove causality, and many other unmeasured confounding factors could have contributed to the findings.
However, Dr. Ceriello noted that many important risk factors such as diabetes, hypertension, and dyslipidemia, were controlled for.
“In this study, all the patients involved were at high risk of cardiovascular events and they were well treated with statins and antithrombotics, so the relationship between the presence of plastic particles in plaque and cardiovascular events is seen on top of good preventive therapy,” he said.
“While we cannot say for sure that we have shown a causal relationship, we found a large effect and there is a great deal of literature than supports this. We know that plastic particles can penetrate cells and act at the mitochondrial level to increase free radical production and produce chronic inflammation which is the basis for atherosclerosis,” Dr. Ceriello added.
He believes there is only one approach to addressing this issue, and that is to reduce the amount of plastic in the environment.
“Plastic is everywhere — in water pipes, in the ocean. We are hoping that this study will increase the push for government to act on this. This is even more important for the long-term health of our children, who will be exposed to high levels of plastics for the whole of their lives,” he said.
‘Strongly Suggestive of a Causal Relationship’
Commenting for this news organization, Philip J. Landrigan, MD, author of an editorial accompanying publication of the study in the NEJM, described the link as “strongly suggestive.”
“Because this was just a single observational study, it doesn’t prove cause and effect, but I think this is strongly suggestive of a causal relationship,” he said. “While there may be some other confounding factors at play, it is hard for me to imagine that these could account for a hazard ratio of 4.5 — that is a large and alarming increase in just 3 years.”
Dr. Landrigan, who is director of the Program for Global Public Health and the Common Good, Boston College, points out that although it is not known what other exposures may have contributed to the adverse outcomes in patients in this study, the finding of microplastics and nanoplastics in plaque tissue is itself a breakthrough discovery that raises a series of urgent questions. These include: “Should exposure to microplastics and nanoplastics be considered a cardiovascular risk factor? What organs in addition to the heart may be at risk? How can we reduce exposure?”
Dr. Landrigan said he was not surprised that plastic particles had been found in carotid plaques. “Previous studies have found microplastics in other tissues including the lungs, colon and placenta. Now they have turned up in the vessel wall,” he said. “But what is really striking about this study is that it suggests the presence of these plastic particles is causing serious harm.”
He says this should be a wake-up call. “It is telling us that we need to worry about the amount of plastic in our environment. And it is not something that’s going to be a problem down the line — it is affecting us now.”
Dr. Landrigan explained that plastic particles are taken into the body predominantly by ingestion, which could include drinking from plastic bottles or eating food wrapped in plastic. He said it is particularly damaging to use plastic containers to heat food in the microwave, as heating plastic up drives particles into the food. “That will really increase exposure.”
He noted that plastics are often already in the food itself, especially seafood.
“Plastics are dumped in the ocean, they break down and get picked up by the fish. Especially if you eat fish at the top of the food chain like tuna, or if you eat oysters or mussels that are filter feeders, you are more likely to ingest microplastics.”
Dr. Landrigan said he would not advise against eating fish in general, however. “Maybe tuna or other predatory fish may be an issue, but fish in general are good for us, and fish like salmon which have a mainly vegetarian diet are probably safer in this regard.”
The other route is inhalation, with these small plastic particles being widely present in the air, from sources such as vehicle tires becoming abraded from running along the highway.
While it is impossible to avoid taking in plastic completely, Dr. Landrigan says individuals can make efforts to reduce their exposure.
“People can make intelligent choices in their homes about what they purchase for themselves and their families, and they can act in their local environments and workplace to try and reduce plastics.”
He noted that 40% of all plastic currently being made is single use plastic, and that percentage is growing, with global production of plastic on track to double by 2040 and triple by 2060, and most of this rapid growth being single use plastic.
“We are all members of the broader society, and we need to become educated about the plastic situation and lobby our elected officials to come up with a good strong legally binding treaty that will place a cap on plastic production,” Dr. Landrigan said.
A version of this article appeared on Medscape.com.
According to a new study, patients found to have microplastics and nanoplastics in their carotid artery plaque had a higher risk for death or major cardiovascular events compared with patients who had plaques where particles were not found.
, study coauthor Antonio Ceriello, MD, IRCCS MultiMedica, Milan, told this news organization.
“I believe we have demonstrated that plastics are a new risk factor for cardiovascular disease,” he added. And while plastics may have made our lives easier in many respects, it appears that the price we are paying for that is a shortening of our lives. That is not a good balance.”
The trial involved 304 patients undergoing carotid endarterectomy for asymptomatic carotid artery disease, whose excised plaque specimens were analyzed for the presence of microplastics and nanoplastics, ultimately found in almost 60% of patients.
After a mean follow-up of 34 months, patients in whom microplastics and nanoplastics were detected within the atheroma had a 4.5 times higher risk for the composite endpoint of all cause death, myocardial infarction, or stroke than those in whom these substances were not detected (hazard ratio, 4.53; 95% CI, 2.00-10.27; P < .001).
The study, led by Raffaele Marfella, MD, University of Campania Luigi Vanvitelli, Naples, Italy, was published in The New England Journal of Medicine on March 7, 2024.
The researchers say the study does not prove causality, and many other unmeasured confounding factors could have contributed to the findings.
However, Dr. Ceriello noted that many important risk factors such as diabetes, hypertension, and dyslipidemia, were controlled for.
“In this study, all the patients involved were at high risk of cardiovascular events and they were well treated with statins and antithrombotics, so the relationship between the presence of plastic particles in plaque and cardiovascular events is seen on top of good preventive therapy,” he said.
“While we cannot say for sure that we have shown a causal relationship, we found a large effect and there is a great deal of literature than supports this. We know that plastic particles can penetrate cells and act at the mitochondrial level to increase free radical production and produce chronic inflammation which is the basis for atherosclerosis,” Dr. Ceriello added.
He believes there is only one approach to addressing this issue, and that is to reduce the amount of plastic in the environment.
“Plastic is everywhere — in water pipes, in the ocean. We are hoping that this study will increase the push for government to act on this. This is even more important for the long-term health of our children, who will be exposed to high levels of plastics for the whole of their lives,” he said.
‘Strongly Suggestive of a Causal Relationship’
Commenting for this news organization, Philip J. Landrigan, MD, author of an editorial accompanying publication of the study in the NEJM, described the link as “strongly suggestive.”
“Because this was just a single observational study, it doesn’t prove cause and effect, but I think this is strongly suggestive of a causal relationship,” he said. “While there may be some other confounding factors at play, it is hard for me to imagine that these could account for a hazard ratio of 4.5 — that is a large and alarming increase in just 3 years.”
Dr. Landrigan, who is director of the Program for Global Public Health and the Common Good, Boston College, points out that although it is not known what other exposures may have contributed to the adverse outcomes in patients in this study, the finding of microplastics and nanoplastics in plaque tissue is itself a breakthrough discovery that raises a series of urgent questions. These include: “Should exposure to microplastics and nanoplastics be considered a cardiovascular risk factor? What organs in addition to the heart may be at risk? How can we reduce exposure?”
Dr. Landrigan said he was not surprised that plastic particles had been found in carotid plaques. “Previous studies have found microplastics in other tissues including the lungs, colon and placenta. Now they have turned up in the vessel wall,” he said. “But what is really striking about this study is that it suggests the presence of these plastic particles is causing serious harm.”
He says this should be a wake-up call. “It is telling us that we need to worry about the amount of plastic in our environment. And it is not something that’s going to be a problem down the line — it is affecting us now.”
Dr. Landrigan explained that plastic particles are taken into the body predominantly by ingestion, which could include drinking from plastic bottles or eating food wrapped in plastic. He said it is particularly damaging to use plastic containers to heat food in the microwave, as heating plastic up drives particles into the food. “That will really increase exposure.”
He noted that plastics are often already in the food itself, especially seafood.
“Plastics are dumped in the ocean, they break down and get picked up by the fish. Especially if you eat fish at the top of the food chain like tuna, or if you eat oysters or mussels that are filter feeders, you are more likely to ingest microplastics.”
Dr. Landrigan said he would not advise against eating fish in general, however. “Maybe tuna or other predatory fish may be an issue, but fish in general are good for us, and fish like salmon which have a mainly vegetarian diet are probably safer in this regard.”
The other route is inhalation, with these small plastic particles being widely present in the air, from sources such as vehicle tires becoming abraded from running along the highway.
While it is impossible to avoid taking in plastic completely, Dr. Landrigan says individuals can make efforts to reduce their exposure.
“People can make intelligent choices in their homes about what they purchase for themselves and their families, and they can act in their local environments and workplace to try and reduce plastics.”
He noted that 40% of all plastic currently being made is single use plastic, and that percentage is growing, with global production of plastic on track to double by 2040 and triple by 2060, and most of this rapid growth being single use plastic.
“We are all members of the broader society, and we need to become educated about the plastic situation and lobby our elected officials to come up with a good strong legally binding treaty that will place a cap on plastic production,” Dr. Landrigan said.
A version of this article appeared on Medscape.com.
Artificially Sweetened Drinks Linked to Increased AF Risk
TOPLINE:
(AF) in a new observational study.
METHODOLOGY:
- The population-based cohort study looked at the associations of sugar-sweetened beverages, artificial sweetened beverages, and pure fruit juice consumption with the risk for incident AF and evaluated whether genetic susceptibility modifies these associations.
- The authors analyzed data from the UK Biobank on 201,856 participants who were free of baseline AF, had genetic data available, and completed a 24-hour diet questionnaire. The diagnosis of AF was obtained by linkage from primary care, hospital inpatient, and death register records.
- The results were adjusted for a wide range of potential confounders including age, sex, ethnicity, education level, socioeconomic status, smoking, alcohol consumption, physical activity level, sleep duration, body mass index, blood pressure, kidney function, sleep apnea, coronary heart disease, diabetes, and the use of lipid-lowering or antihypertensive medication.
TAKEAWAY:
- During a median follow-up of 9.9 years, 9362 incident AF cases were documented.
- Compared with nonconsumers, individuals who consumed more than 2 L per week of artificially sweetened beverages had a 20% increased risk of developing AF (hazard ratio [HR], 1.20; 95% CI, 1.10-1.31).
- Those who drank more than 2 L per week of sugar-sweetened beverages had a 10% increased risk for AF (HR, 1.10; 95% CI, 1.01-1.20).
- Consumption of 1 L or less per week of pure fruit juice was associated with an 8% lower risk of developing AF (HR, 0.92; 95% CI, 0.87-0.97).
- The associations persisted after adjustment for genetic susceptibility for AF.
IN PRACTICE:
The study authors concluded that this study does not demonstrate that consumption of sugar-sweetened or artificially sweetened beverages alters AF risk but rather that the consumption of these drinks may predict AF risk beyond traditional risk factors. They added that intervention studies and basic research are warranted to confirm whether the observed associations are causal. Commenting on the study, Duane Mellor, MD, registered dietitian at Aston University, Birmingham, England, said it is unclear if the observations in this study are a chance finding as there is a lack of a clear biological link. Naveed Sattar, MD, professor of metabolic medicine at the University of Glasgow, Glasgow, Scotland, added that although the authors tried to adjust for many factors, there is a strong chance that other behavioral aspects linked to beverage choice could be more relevant as a cause of AF rather than the drinks themselves. Tom Sanders, MD, professor emeritus of nutrition and dietetics, King’s College London, London, England, pointed out that as this is the first study that has reported such an effect with artificially sweetened drinks, the finding needs replication before any conclusions can be drawn. “It remains good dietary advice to recommend the consumption of low-calorie artificially sweetened drink in place of sugar-sweetened drinks and alcohol,” he added.
SOURCE:
The study, led by Ying Sun, MD, Shanghai Jiao Tong University School of Medicine, Shanghai, China, was published online in Circulation: Arrhythmia and Electrophysiology.
LIMITATIONS:
The consumption of beverages was self-reported and based on only five separate single-day food intake recalls which were taken over the first 3 years of the study, which was extrapolated to estimate weekly intake. The researchers could not tell whether the sugar-sweetened and artificially sweetened drinks were caffeinated and could not rule out residual confounding by other unmeasured or unknown factors.
DISCLOSURES:
This study was supported by the National Natural Science Foundation of China, Shanghai Municipal Health Commission, Shanghai Municipal Human Resources and Social Security Bureau, Clinical Research Plan of Shanghai Hospital Development Center, Postdoctoral Scientific Research Foundation of Shanghai Ninth People’s Hospital, and Shanghai Jiao Tong University School of Medicine.
A version of this article appeared on Medscape.com.
TOPLINE:
(AF) in a new observational study.
METHODOLOGY:
- The population-based cohort study looked at the associations of sugar-sweetened beverages, artificial sweetened beverages, and pure fruit juice consumption with the risk for incident AF and evaluated whether genetic susceptibility modifies these associations.
- The authors analyzed data from the UK Biobank on 201,856 participants who were free of baseline AF, had genetic data available, and completed a 24-hour diet questionnaire. The diagnosis of AF was obtained by linkage from primary care, hospital inpatient, and death register records.
- The results were adjusted for a wide range of potential confounders including age, sex, ethnicity, education level, socioeconomic status, smoking, alcohol consumption, physical activity level, sleep duration, body mass index, blood pressure, kidney function, sleep apnea, coronary heart disease, diabetes, and the use of lipid-lowering or antihypertensive medication.
TAKEAWAY:
- During a median follow-up of 9.9 years, 9362 incident AF cases were documented.
- Compared with nonconsumers, individuals who consumed more than 2 L per week of artificially sweetened beverages had a 20% increased risk of developing AF (hazard ratio [HR], 1.20; 95% CI, 1.10-1.31).
- Those who drank more than 2 L per week of sugar-sweetened beverages had a 10% increased risk for AF (HR, 1.10; 95% CI, 1.01-1.20).
- Consumption of 1 L or less per week of pure fruit juice was associated with an 8% lower risk of developing AF (HR, 0.92; 95% CI, 0.87-0.97).
- The associations persisted after adjustment for genetic susceptibility for AF.
IN PRACTICE:
The study authors concluded that this study does not demonstrate that consumption of sugar-sweetened or artificially sweetened beverages alters AF risk but rather that the consumption of these drinks may predict AF risk beyond traditional risk factors. They added that intervention studies and basic research are warranted to confirm whether the observed associations are causal. Commenting on the study, Duane Mellor, MD, registered dietitian at Aston University, Birmingham, England, said it is unclear if the observations in this study are a chance finding as there is a lack of a clear biological link. Naveed Sattar, MD, professor of metabolic medicine at the University of Glasgow, Glasgow, Scotland, added that although the authors tried to adjust for many factors, there is a strong chance that other behavioral aspects linked to beverage choice could be more relevant as a cause of AF rather than the drinks themselves. Tom Sanders, MD, professor emeritus of nutrition and dietetics, King’s College London, London, England, pointed out that as this is the first study that has reported such an effect with artificially sweetened drinks, the finding needs replication before any conclusions can be drawn. “It remains good dietary advice to recommend the consumption of low-calorie artificially sweetened drink in place of sugar-sweetened drinks and alcohol,” he added.
SOURCE:
The study, led by Ying Sun, MD, Shanghai Jiao Tong University School of Medicine, Shanghai, China, was published online in Circulation: Arrhythmia and Electrophysiology.
LIMITATIONS:
The consumption of beverages was self-reported and based on only five separate single-day food intake recalls which were taken over the first 3 years of the study, which was extrapolated to estimate weekly intake. The researchers could not tell whether the sugar-sweetened and artificially sweetened drinks were caffeinated and could not rule out residual confounding by other unmeasured or unknown factors.
DISCLOSURES:
This study was supported by the National Natural Science Foundation of China, Shanghai Municipal Health Commission, Shanghai Municipal Human Resources and Social Security Bureau, Clinical Research Plan of Shanghai Hospital Development Center, Postdoctoral Scientific Research Foundation of Shanghai Ninth People’s Hospital, and Shanghai Jiao Tong University School of Medicine.
A version of this article appeared on Medscape.com.
TOPLINE:
(AF) in a new observational study.
METHODOLOGY:
- The population-based cohort study looked at the associations of sugar-sweetened beverages, artificial sweetened beverages, and pure fruit juice consumption with the risk for incident AF and evaluated whether genetic susceptibility modifies these associations.
- The authors analyzed data from the UK Biobank on 201,856 participants who were free of baseline AF, had genetic data available, and completed a 24-hour diet questionnaire. The diagnosis of AF was obtained by linkage from primary care, hospital inpatient, and death register records.
- The results were adjusted for a wide range of potential confounders including age, sex, ethnicity, education level, socioeconomic status, smoking, alcohol consumption, physical activity level, sleep duration, body mass index, blood pressure, kidney function, sleep apnea, coronary heart disease, diabetes, and the use of lipid-lowering or antihypertensive medication.
TAKEAWAY:
- During a median follow-up of 9.9 years, 9362 incident AF cases were documented.
- Compared with nonconsumers, individuals who consumed more than 2 L per week of artificially sweetened beverages had a 20% increased risk of developing AF (hazard ratio [HR], 1.20; 95% CI, 1.10-1.31).
- Those who drank more than 2 L per week of sugar-sweetened beverages had a 10% increased risk for AF (HR, 1.10; 95% CI, 1.01-1.20).
- Consumption of 1 L or less per week of pure fruit juice was associated with an 8% lower risk of developing AF (HR, 0.92; 95% CI, 0.87-0.97).
- The associations persisted after adjustment for genetic susceptibility for AF.
IN PRACTICE:
The study authors concluded that this study does not demonstrate that consumption of sugar-sweetened or artificially sweetened beverages alters AF risk but rather that the consumption of these drinks may predict AF risk beyond traditional risk factors. They added that intervention studies and basic research are warranted to confirm whether the observed associations are causal. Commenting on the study, Duane Mellor, MD, registered dietitian at Aston University, Birmingham, England, said it is unclear if the observations in this study are a chance finding as there is a lack of a clear biological link. Naveed Sattar, MD, professor of metabolic medicine at the University of Glasgow, Glasgow, Scotland, added that although the authors tried to adjust for many factors, there is a strong chance that other behavioral aspects linked to beverage choice could be more relevant as a cause of AF rather than the drinks themselves. Tom Sanders, MD, professor emeritus of nutrition and dietetics, King’s College London, London, England, pointed out that as this is the first study that has reported such an effect with artificially sweetened drinks, the finding needs replication before any conclusions can be drawn. “It remains good dietary advice to recommend the consumption of low-calorie artificially sweetened drink in place of sugar-sweetened drinks and alcohol,” he added.
SOURCE:
The study, led by Ying Sun, MD, Shanghai Jiao Tong University School of Medicine, Shanghai, China, was published online in Circulation: Arrhythmia and Electrophysiology.
LIMITATIONS:
The consumption of beverages was self-reported and based on only five separate single-day food intake recalls which were taken over the first 3 years of the study, which was extrapolated to estimate weekly intake. The researchers could not tell whether the sugar-sweetened and artificially sweetened drinks were caffeinated and could not rule out residual confounding by other unmeasured or unknown factors.
DISCLOSURES:
This study was supported by the National Natural Science Foundation of China, Shanghai Municipal Health Commission, Shanghai Municipal Human Resources and Social Security Bureau, Clinical Research Plan of Shanghai Hospital Development Center, Postdoctoral Scientific Research Foundation of Shanghai Ninth People’s Hospital, and Shanghai Jiao Tong University School of Medicine.
A version of this article appeared on Medscape.com.
Effect of Metformin Across Renal Function States in Diabetes
TOPLINE:
Metformin cuts the risk for diabetic nephropathy (DN) and major kidney and cardiovascular events in patients with newly diagnosed type 2 diabetes (T2D) across various renal function states.
METHODOLOGY:
Metformin is a first-line treatment in US and South Korean T2D management guidelines, except for patients with advanced chronic kidney disease (CKD) (stage, ≥ 4; estimated glomerular filtration rate [eGFR], < 30).
The study used data from the databases of three tertiary hospitals in South Korea to assess the effect of metformin on long-term renal and cardiovascular outcomes across various renal function states in patients with newly diagnosed T2D.
Four groups of treatment-control comparative cohorts were identified at each hospital: Patients who had not yet developed DN at T2D diagnosis (mean age in treatment and control cohorts, 61-65 years) and those with reduced renal function (CKD stages 3A, 3B, and 4).
Patients who continuously received metformin after T2D diagnosis and beyond the observation period were 1:1 propensity score matched with controls who were prescribed oral hypoglycemic agents other than metformin.
Primary outcomes were net major adverse cardiovascular events including strokes (MACEs) or in-hospital death and a composite of major adverse kidney events (MAKEs) or in-hospital death.
TAKEAWAY:
Among patients without DN at T2D diagnosis, the continuous use of metformin vs other oral hypoglycemic agents was associated with a lower risk for:
Overt DN (incidence rate ratio [IRR], 0.82; 95% CI, 0.71-0.95),
MACEs (IRR, 0.76; 95% CI, 0.64-0.92), and
MAKEs (IRR, 0.45; 95% CI, 0.33-0.62).
Compared with non-metformin or discontinued metformin use, the continuous use of metformin was associated with a lower risk for MACE across CKD stages 3A (IRR, 0.70; 95% CI, 0.57-0.87), 3B (IRR, 0.83; 95% CI, 0.74-0.93), and 4 (IRR, 0.71; 95% CI, 0.60-0.85).
Similarly, the risk for MAKE was lower among continuous metformin users than in nonusers or discontinuous metformin users across CKD stage 3A (IRR, 0.39; 95% CI, 0.35-0.43), 3B (IRR, 0.44; 95% CI, 0.40-0.48), and 4 (IRR, 0.45; 95% CI, 0.39-0.51).
IN PRACTICE:
“The significance of the current study is highlighted by its integration of real-world clinical data, which encompasses patients diagnosed with CDK4 [eGRF, 15-29 mL/min/1.73 m2], a group currently considered contraindicated,” the authors wrote.
SOURCE:
The study, led by Yongjin Yi, MD, PhD, Department of Internal Medicine, Dankook University College of Medicine, Cheonan-si, Republic of Korea, was published in Scientific Reports.
LIMITATIONS:
There may be a possibility of selection bias because of the retrospective and observational nature of this study. Despite achieving a 1:1 propensity score matching to address the confounding factors, some variables, such as serum albumin and A1c levels, remained unbalanced after matching. The paper did not include observation length or patient numbers, but in response to an email query from Medscape, Yi notes that in one hospital, the mean duration of observation for the control and treatment groups was about 6.5 years, and the total number in the treatment groups across data from three hospitals was 11,675, with the same number of matched controls.
DISCLOSURES:
This study was supported by a Young Investigator Research Grant from the Korean Society of Nephrology, a grant from the Seoul National University Bundang Hospital Research Fund, and the Bio&Medical Technology Development Program of the National Research Foundation funded by the Korean government. The authors disclosed no competing interests.
A version of this article appeared on Medscape.com.
TOPLINE:
Metformin cuts the risk for diabetic nephropathy (DN) and major kidney and cardiovascular events in patients with newly diagnosed type 2 diabetes (T2D) across various renal function states.
METHODOLOGY:
Metformin is a first-line treatment in US and South Korean T2D management guidelines, except for patients with advanced chronic kidney disease (CKD) (stage, ≥ 4; estimated glomerular filtration rate [eGFR], < 30).
The study used data from the databases of three tertiary hospitals in South Korea to assess the effect of metformin on long-term renal and cardiovascular outcomes across various renal function states in patients with newly diagnosed T2D.
Four groups of treatment-control comparative cohorts were identified at each hospital: Patients who had not yet developed DN at T2D diagnosis (mean age in treatment and control cohorts, 61-65 years) and those with reduced renal function (CKD stages 3A, 3B, and 4).
Patients who continuously received metformin after T2D diagnosis and beyond the observation period were 1:1 propensity score matched with controls who were prescribed oral hypoglycemic agents other than metformin.
Primary outcomes were net major adverse cardiovascular events including strokes (MACEs) or in-hospital death and a composite of major adverse kidney events (MAKEs) or in-hospital death.
TAKEAWAY:
Among patients without DN at T2D diagnosis, the continuous use of metformin vs other oral hypoglycemic agents was associated with a lower risk for:
Overt DN (incidence rate ratio [IRR], 0.82; 95% CI, 0.71-0.95),
MACEs (IRR, 0.76; 95% CI, 0.64-0.92), and
MAKEs (IRR, 0.45; 95% CI, 0.33-0.62).
Compared with non-metformin or discontinued metformin use, the continuous use of metformin was associated with a lower risk for MACE across CKD stages 3A (IRR, 0.70; 95% CI, 0.57-0.87), 3B (IRR, 0.83; 95% CI, 0.74-0.93), and 4 (IRR, 0.71; 95% CI, 0.60-0.85).
Similarly, the risk for MAKE was lower among continuous metformin users than in nonusers or discontinuous metformin users across CKD stage 3A (IRR, 0.39; 95% CI, 0.35-0.43), 3B (IRR, 0.44; 95% CI, 0.40-0.48), and 4 (IRR, 0.45; 95% CI, 0.39-0.51).
IN PRACTICE:
“The significance of the current study is highlighted by its integration of real-world clinical data, which encompasses patients diagnosed with CDK4 [eGRF, 15-29 mL/min/1.73 m2], a group currently considered contraindicated,” the authors wrote.
SOURCE:
The study, led by Yongjin Yi, MD, PhD, Department of Internal Medicine, Dankook University College of Medicine, Cheonan-si, Republic of Korea, was published in Scientific Reports.
LIMITATIONS:
There may be a possibility of selection bias because of the retrospective and observational nature of this study. Despite achieving a 1:1 propensity score matching to address the confounding factors, some variables, such as serum albumin and A1c levels, remained unbalanced after matching. The paper did not include observation length or patient numbers, but in response to an email query from Medscape, Yi notes that in one hospital, the mean duration of observation for the control and treatment groups was about 6.5 years, and the total number in the treatment groups across data from three hospitals was 11,675, with the same number of matched controls.
DISCLOSURES:
This study was supported by a Young Investigator Research Grant from the Korean Society of Nephrology, a grant from the Seoul National University Bundang Hospital Research Fund, and the Bio&Medical Technology Development Program of the National Research Foundation funded by the Korean government. The authors disclosed no competing interests.
A version of this article appeared on Medscape.com.
TOPLINE:
Metformin cuts the risk for diabetic nephropathy (DN) and major kidney and cardiovascular events in patients with newly diagnosed type 2 diabetes (T2D) across various renal function states.
METHODOLOGY:
Metformin is a first-line treatment in US and South Korean T2D management guidelines, except for patients with advanced chronic kidney disease (CKD) (stage, ≥ 4; estimated glomerular filtration rate [eGFR], < 30).
The study used data from the databases of three tertiary hospitals in South Korea to assess the effect of metformin on long-term renal and cardiovascular outcomes across various renal function states in patients with newly diagnosed T2D.
Four groups of treatment-control comparative cohorts were identified at each hospital: Patients who had not yet developed DN at T2D diagnosis (mean age in treatment and control cohorts, 61-65 years) and those with reduced renal function (CKD stages 3A, 3B, and 4).
Patients who continuously received metformin after T2D diagnosis and beyond the observation period were 1:1 propensity score matched with controls who were prescribed oral hypoglycemic agents other than metformin.
Primary outcomes were net major adverse cardiovascular events including strokes (MACEs) or in-hospital death and a composite of major adverse kidney events (MAKEs) or in-hospital death.
TAKEAWAY:
Among patients without DN at T2D diagnosis, the continuous use of metformin vs other oral hypoglycemic agents was associated with a lower risk for:
Overt DN (incidence rate ratio [IRR], 0.82; 95% CI, 0.71-0.95),
MACEs (IRR, 0.76; 95% CI, 0.64-0.92), and
MAKEs (IRR, 0.45; 95% CI, 0.33-0.62).
Compared with non-metformin or discontinued metformin use, the continuous use of metformin was associated with a lower risk for MACE across CKD stages 3A (IRR, 0.70; 95% CI, 0.57-0.87), 3B (IRR, 0.83; 95% CI, 0.74-0.93), and 4 (IRR, 0.71; 95% CI, 0.60-0.85).
Similarly, the risk for MAKE was lower among continuous metformin users than in nonusers or discontinuous metformin users across CKD stage 3A (IRR, 0.39; 95% CI, 0.35-0.43), 3B (IRR, 0.44; 95% CI, 0.40-0.48), and 4 (IRR, 0.45; 95% CI, 0.39-0.51).
IN PRACTICE:
“The significance of the current study is highlighted by its integration of real-world clinical data, which encompasses patients diagnosed with CDK4 [eGRF, 15-29 mL/min/1.73 m2], a group currently considered contraindicated,” the authors wrote.
SOURCE:
The study, led by Yongjin Yi, MD, PhD, Department of Internal Medicine, Dankook University College of Medicine, Cheonan-si, Republic of Korea, was published in Scientific Reports.
LIMITATIONS:
There may be a possibility of selection bias because of the retrospective and observational nature of this study. Despite achieving a 1:1 propensity score matching to address the confounding factors, some variables, such as serum albumin and A1c levels, remained unbalanced after matching. The paper did not include observation length or patient numbers, but in response to an email query from Medscape, Yi notes that in one hospital, the mean duration of observation for the control and treatment groups was about 6.5 years, and the total number in the treatment groups across data from three hospitals was 11,675, with the same number of matched controls.
DISCLOSURES:
This study was supported by a Young Investigator Research Grant from the Korean Society of Nephrology, a grant from the Seoul National University Bundang Hospital Research Fund, and the Bio&Medical Technology Development Program of the National Research Foundation funded by the Korean government. The authors disclosed no competing interests.
A version of this article appeared on Medscape.com.