User login
New Drug Approvals Are the Wrong Metric for Cancer Policy
How should we define success in cancer policy — what should the endpoint be?
It’s debatable. Is it fewer cancer deaths? Perhaps improved access to therapies or a reduction in disparities?
One thing I know with certainty: The number of new cancer drugs approved by the US Food and Drug Administration (FDA) is not and should not be our primary endpoint in and of itself.
I’ll go a step further: It is not even a surrogate marker for success.
Unfortunately, a new drug approval does not necessarily mean improved patient outcomes. In fact, the majority of cancer drugs approved these days improve neither survival nor quality of life. Our previous work has shown better mortality outcomes in other high-income countries that have not approved or do not fund several cancer drugs that the FDA has approved.
Even if a drug has a meaningful benefit, at an average cost of more than $250,000 per year, if a new drug cannot reach patients because of access or cost issues, it’s meaningless.
However, regulators and media celebrate the number (and speed) of drug approvals every year as if it were a marker of success in and of itself. But approving more drugs should not be the goal; improving outcomes should. The FDA’s current approach is akin to a university celebrating its graduation rate by lowering the requirements to pass.
When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine ‘ending cancer as we know it’ is premature and even embarrassing.
This is exactly what the FDA has been doing with our regulatory standards for drug approval. They have gradually lowered the requirements for approval from two randomized trials to one randomized trial, then further to one randomized trial with a surrogate endpoint. In many instances, they have gone even further, demanding merely single-arm trials. They’ve also gone from requiring overall survival benefits to celebrating nondetrimental effects on overall survival. It’s no wonder that we approve more drugs today than we did in the past — the bar for approval is pretty low nowadays.
In 2019, our lab found an interesting phenomenon: The number of approvals based on surrogate endpoints has been increasing while the number of accelerated approvals has been decreasing. This made no sense at first, because you’d think surrogate-based approvals and accelerated approvals would be collinear. However, we realized that the recent approvals based on surrogate endpoints were regular approvals instead of accelerated approvals, which explained the phenomenon. Not only is the FDA approving more drugs on the basis of lower levels of evidence, but the agency is also offering regular instead of accelerated approval, thereby removing the safety net of a confirmatory trial.
Nearly everybody sees this as a cause for celebration. Pharma celebrates record profits, regulators celebrate record numbers of drug approvals, insurance companies celebrate because they can pass these costs on as insurance premiums and make even more money, and physicians and patients celebrate access to the shiniest, sexiest new cancer drug.
Everybody is happy in this system. The only problem is that patient outcomes don’t improve, resources are taken away from other priorities, and society suffers a net harm.
When you contrast this celebration with the reality on the ground, the difference is stark and sobering. In our clinics, patients lack access to even old chemotherapeutic drugs that are already generic and cheap but make a meaningful difference in patient outcomes. Citing a current lack of incentives, several generic cancer drug manufacturers have stopped making these drugs; the US supply now relies heavily on importing them from emerging economies such as India. When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine “ending cancer as we know it” is premature and even embarrassing.
5-Fluorouracil, methotrexate, and the platinums are backbones of cancer treatment. Cisplatin and carboplatin are not drugs we use with the hope of improving survival by a couple of months; these drugs are the difference between life and death for patients with testicular and ovarian cancers. In a survey of 948 global oncologists, these were considered among the most essential cancer drugs by oncologists in high-income and low- and middle-income countries alike. Although oncologists in low- and middle-income countries sometimes argue that even these cheap generic drugs may be unaffordable to their patients, they usually remain available; access is a function of both availability and affordability. However, the shortage situation in the US is unique in that availability — rather than affordability — is impacting access.
Our profit-over-patients policy has landed us in a terrible paradox.
Generic drugs are cheap, and any industrialized country can manufacture them. This is why so few companies actually do so; the profit margins are low and companies have little incentive to produce them, despite their benefit. Meanwhile, the FDA is approving and offering access to new shiny molecules that cost more than $15,000 per month yet offer less than a month of progression-free survival benefit and no overall survival benefit (see margetuximab in breast cancer). We have a literal fatal attraction to everything new and shiny.
This is a clear misalignment of priorities in US cancer drug policy. Our profit-over-patients policy has landed us in a terrible paradox: If a drug is cheap and meaningful, it won’t be available, but if it is marginal and expensive, we will do everything to ensure patients can get it. It’s no wonder that patients on Medicaid are disproportionately affected by these drug shortages. Unless all patients have easy access to cisplatin, carboplatin, and 5-fluorouracil, it is frankly embarrassing to celebrate the number of new cancer drugs approved each year.
We all have a responsibility in this — policymakers and lawmakers, regulators and payers, manufacturers and distributors, the American Society of Clinical Oncology and other oncology societies, and physicians and patients. This is where our advocacy work should focus. The primary endpoint of our cancer policy should not be how many new treatments we can approve or how many expensive drugs a rich person with the best insurance can get at a leading cancer center. The true measure of our civilization is how it treats its most vulnerable members.
Dr. Gyawali has disclosed the following relevant financial relationship: Received consulting fees from Vivio Health.
Dr. Gyawali is an associate professor in the Departments of Oncology and Public Health Sciences and a scientist in the Division of Cancer Care and Epidemiology at Queen’s University in Kingston, Ontario, Canada, and is also affiliated faculty at the Program on Regulation, Therapeutics, and Law in the Department of Medicine at Brigham and Women’s Hospital in Boston. His clinical and research interests revolve around cancer policy, global oncology, evidence-based oncology, financial toxicities of cancer treatment, clinical trial methods, and supportive care. He tweets at @oncology_bg.
A version of this article appeared on Medscape.com.
How should we define success in cancer policy — what should the endpoint be?
It’s debatable. Is it fewer cancer deaths? Perhaps improved access to therapies or a reduction in disparities?
One thing I know with certainty: The number of new cancer drugs approved by the US Food and Drug Administration (FDA) is not and should not be our primary endpoint in and of itself.
I’ll go a step further: It is not even a surrogate marker for success.
Unfortunately, a new drug approval does not necessarily mean improved patient outcomes. In fact, the majority of cancer drugs approved these days improve neither survival nor quality of life. Our previous work has shown better mortality outcomes in other high-income countries that have not approved or do not fund several cancer drugs that the FDA has approved.
Even if a drug has a meaningful benefit, at an average cost of more than $250,000 per year, if a new drug cannot reach patients because of access or cost issues, it’s meaningless.
However, regulators and media celebrate the number (and speed) of drug approvals every year as if it were a marker of success in and of itself. But approving more drugs should not be the goal; improving outcomes should. The FDA’s current approach is akin to a university celebrating its graduation rate by lowering the requirements to pass.
When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine ‘ending cancer as we know it’ is premature and even embarrassing.
This is exactly what the FDA has been doing with our regulatory standards for drug approval. They have gradually lowered the requirements for approval from two randomized trials to one randomized trial, then further to one randomized trial with a surrogate endpoint. In many instances, they have gone even further, demanding merely single-arm trials. They’ve also gone from requiring overall survival benefits to celebrating nondetrimental effects on overall survival. It’s no wonder that we approve more drugs today than we did in the past — the bar for approval is pretty low nowadays.
In 2019, our lab found an interesting phenomenon: The number of approvals based on surrogate endpoints has been increasing while the number of accelerated approvals has been decreasing. This made no sense at first, because you’d think surrogate-based approvals and accelerated approvals would be collinear. However, we realized that the recent approvals based on surrogate endpoints were regular approvals instead of accelerated approvals, which explained the phenomenon. Not only is the FDA approving more drugs on the basis of lower levels of evidence, but the agency is also offering regular instead of accelerated approval, thereby removing the safety net of a confirmatory trial.
Nearly everybody sees this as a cause for celebration. Pharma celebrates record profits, regulators celebrate record numbers of drug approvals, insurance companies celebrate because they can pass these costs on as insurance premiums and make even more money, and physicians and patients celebrate access to the shiniest, sexiest new cancer drug.
Everybody is happy in this system. The only problem is that patient outcomes don’t improve, resources are taken away from other priorities, and society suffers a net harm.
When you contrast this celebration with the reality on the ground, the difference is stark and sobering. In our clinics, patients lack access to even old chemotherapeutic drugs that are already generic and cheap but make a meaningful difference in patient outcomes. Citing a current lack of incentives, several generic cancer drug manufacturers have stopped making these drugs; the US supply now relies heavily on importing them from emerging economies such as India. When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine “ending cancer as we know it” is premature and even embarrassing.
5-Fluorouracil, methotrexate, and the platinums are backbones of cancer treatment. Cisplatin and carboplatin are not drugs we use with the hope of improving survival by a couple of months; these drugs are the difference between life and death for patients with testicular and ovarian cancers. In a survey of 948 global oncologists, these were considered among the most essential cancer drugs by oncologists in high-income and low- and middle-income countries alike. Although oncologists in low- and middle-income countries sometimes argue that even these cheap generic drugs may be unaffordable to their patients, they usually remain available; access is a function of both availability and affordability. However, the shortage situation in the US is unique in that availability — rather than affordability — is impacting access.
Our profit-over-patients policy has landed us in a terrible paradox.
Generic drugs are cheap, and any industrialized country can manufacture them. This is why so few companies actually do so; the profit margins are low and companies have little incentive to produce them, despite their benefit. Meanwhile, the FDA is approving and offering access to new shiny molecules that cost more than $15,000 per month yet offer less than a month of progression-free survival benefit and no overall survival benefit (see margetuximab in breast cancer). We have a literal fatal attraction to everything new and shiny.
This is a clear misalignment of priorities in US cancer drug policy. Our profit-over-patients policy has landed us in a terrible paradox: If a drug is cheap and meaningful, it won’t be available, but if it is marginal and expensive, we will do everything to ensure patients can get it. It’s no wonder that patients on Medicaid are disproportionately affected by these drug shortages. Unless all patients have easy access to cisplatin, carboplatin, and 5-fluorouracil, it is frankly embarrassing to celebrate the number of new cancer drugs approved each year.
We all have a responsibility in this — policymakers and lawmakers, regulators and payers, manufacturers and distributors, the American Society of Clinical Oncology and other oncology societies, and physicians and patients. This is where our advocacy work should focus. The primary endpoint of our cancer policy should not be how many new treatments we can approve or how many expensive drugs a rich person with the best insurance can get at a leading cancer center. The true measure of our civilization is how it treats its most vulnerable members.
Dr. Gyawali has disclosed the following relevant financial relationship: Received consulting fees from Vivio Health.
Dr. Gyawali is an associate professor in the Departments of Oncology and Public Health Sciences and a scientist in the Division of Cancer Care and Epidemiology at Queen’s University in Kingston, Ontario, Canada, and is also affiliated faculty at the Program on Regulation, Therapeutics, and Law in the Department of Medicine at Brigham and Women’s Hospital in Boston. His clinical and research interests revolve around cancer policy, global oncology, evidence-based oncology, financial toxicities of cancer treatment, clinical trial methods, and supportive care. He tweets at @oncology_bg.
A version of this article appeared on Medscape.com.
How should we define success in cancer policy — what should the endpoint be?
It’s debatable. Is it fewer cancer deaths? Perhaps improved access to therapies or a reduction in disparities?
One thing I know with certainty: The number of new cancer drugs approved by the US Food and Drug Administration (FDA) is not and should not be our primary endpoint in and of itself.
I’ll go a step further: It is not even a surrogate marker for success.
Unfortunately, a new drug approval does not necessarily mean improved patient outcomes. In fact, the majority of cancer drugs approved these days improve neither survival nor quality of life. Our previous work has shown better mortality outcomes in other high-income countries that have not approved or do not fund several cancer drugs that the FDA has approved.
Even if a drug has a meaningful benefit, at an average cost of more than $250,000 per year, if a new drug cannot reach patients because of access or cost issues, it’s meaningless.
However, regulators and media celebrate the number (and speed) of drug approvals every year as if it were a marker of success in and of itself. But approving more drugs should not be the goal; improving outcomes should. The FDA’s current approach is akin to a university celebrating its graduation rate by lowering the requirements to pass.
When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine ‘ending cancer as we know it’ is premature and even embarrassing.
This is exactly what the FDA has been doing with our regulatory standards for drug approval. They have gradually lowered the requirements for approval from two randomized trials to one randomized trial, then further to one randomized trial with a surrogate endpoint. In many instances, they have gone even further, demanding merely single-arm trials. They’ve also gone from requiring overall survival benefits to celebrating nondetrimental effects on overall survival. It’s no wonder that we approve more drugs today than we did in the past — the bar for approval is pretty low nowadays.
In 2019, our lab found an interesting phenomenon: The number of approvals based on surrogate endpoints has been increasing while the number of accelerated approvals has been decreasing. This made no sense at first, because you’d think surrogate-based approvals and accelerated approvals would be collinear. However, we realized that the recent approvals based on surrogate endpoints were regular approvals instead of accelerated approvals, which explained the phenomenon. Not only is the FDA approving more drugs on the basis of lower levels of evidence, but the agency is also offering regular instead of accelerated approval, thereby removing the safety net of a confirmatory trial.
Nearly everybody sees this as a cause for celebration. Pharma celebrates record profits, regulators celebrate record numbers of drug approvals, insurance companies celebrate because they can pass these costs on as insurance premiums and make even more money, and physicians and patients celebrate access to the shiniest, sexiest new cancer drug.
Everybody is happy in this system. The only problem is that patient outcomes don’t improve, resources are taken away from other priorities, and society suffers a net harm.
When you contrast this celebration with the reality on the ground, the difference is stark and sobering. In our clinics, patients lack access to even old chemotherapeutic drugs that are already generic and cheap but make a meaningful difference in patient outcomes. Citing a current lack of incentives, several generic cancer drug manufacturers have stopped making these drugs; the US supply now relies heavily on importing them from emerging economies such as India. When US patients lack access to cisplatin and carboplatin, any talk of a Moonshot or precision medicine “ending cancer as we know it” is premature and even embarrassing.
5-Fluorouracil, methotrexate, and the platinums are backbones of cancer treatment. Cisplatin and carboplatin are not drugs we use with the hope of improving survival by a couple of months; these drugs are the difference between life and death for patients with testicular and ovarian cancers. In a survey of 948 global oncologists, these were considered among the most essential cancer drugs by oncologists in high-income and low- and middle-income countries alike. Although oncologists in low- and middle-income countries sometimes argue that even these cheap generic drugs may be unaffordable to their patients, they usually remain available; access is a function of both availability and affordability. However, the shortage situation in the US is unique in that availability — rather than affordability — is impacting access.
Our profit-over-patients policy has landed us in a terrible paradox.
Generic drugs are cheap, and any industrialized country can manufacture them. This is why so few companies actually do so; the profit margins are low and companies have little incentive to produce them, despite their benefit. Meanwhile, the FDA is approving and offering access to new shiny molecules that cost more than $15,000 per month yet offer less than a month of progression-free survival benefit and no overall survival benefit (see margetuximab in breast cancer). We have a literal fatal attraction to everything new and shiny.
This is a clear misalignment of priorities in US cancer drug policy. Our profit-over-patients policy has landed us in a terrible paradox: If a drug is cheap and meaningful, it won’t be available, but if it is marginal and expensive, we will do everything to ensure patients can get it. It’s no wonder that patients on Medicaid are disproportionately affected by these drug shortages. Unless all patients have easy access to cisplatin, carboplatin, and 5-fluorouracil, it is frankly embarrassing to celebrate the number of new cancer drugs approved each year.
We all have a responsibility in this — policymakers and lawmakers, regulators and payers, manufacturers and distributors, the American Society of Clinical Oncology and other oncology societies, and physicians and patients. This is where our advocacy work should focus. The primary endpoint of our cancer policy should not be how many new treatments we can approve or how many expensive drugs a rich person with the best insurance can get at a leading cancer center. The true measure of our civilization is how it treats its most vulnerable members.
Dr. Gyawali has disclosed the following relevant financial relationship: Received consulting fees from Vivio Health.
Dr. Gyawali is an associate professor in the Departments of Oncology and Public Health Sciences and a scientist in the Division of Cancer Care and Epidemiology at Queen’s University in Kingston, Ontario, Canada, and is also affiliated faculty at the Program on Regulation, Therapeutics, and Law in the Department of Medicine at Brigham and Women’s Hospital in Boston. His clinical and research interests revolve around cancer policy, global oncology, evidence-based oncology, financial toxicities of cancer treatment, clinical trial methods, and supportive care. He tweets at @oncology_bg.
A version of this article appeared on Medscape.com.
Extraordinary Patients Inspired Father of Cancer Immunotherapy
His pioneering research established interleukin-2 (IL-2) as the first U.S. Food and Drug Administration–approved cancer immunotherapy in 1992.
To recognize his trailblazing work and other achievements, the American Association for Cancer Research (AACR) will award Dr. Rosenberg with the 2024 AACR Award for Lifetime Achievement in Cancer Research at its annual meeting in April.

Dr. Rosenberg, a senior investigator for the Center for Cancer Research at the National Cancer Institute (NCI), and chief of the NCI Surgery Branch, shared the history behind his novel research and the patient stories that inspired his discoveries, during an interview.
Tell us a little about yourself and where you grew up.
Dr. Rosenberg: I grew up in the Bronx. My parents both immigrated to the United States from Poland as teenagers.
As a young boy, did you always want to become a doctor?
Dr. Rosenberg: I think some defining moments on why I decided to go into medicine occurred when I was 6 or 7 years old. The second world war was over, and many of the horrors of the Holocaust became apparent to me. I was brought up as an Orthodox Jew. My parents were quite religious, and I remember postcards coming in one after another about relatives that had died in the death camps. That had a profound influence on me.
How did that experience impact your aspirations?
Dr. Rosenberg: It was an example to me of how evil certain people and groups can be toward one another. I decided at that point, that I wanted to do something good for people, and medicine seemed the most likely way to do that. But also, I was developing a broad scientific interest. I ended up at the Bronx High School of Science and knew that I not only wanted to practice the medicine of today, but I wanted to play a role in helping develop the medicine.
What led to your interest in cancer treatment?
Dr. Rosenberg: Well, as a medical student and resident, it became clear that the field of cancer needed major improvement. We had three major ways to treat cancer: surgery, radiation therapy, and chemotherapy. That could cure about half of the people [who] had cancer. But despite the best application of those three specialties, there were over 600,000 deaths from cancer each year in the United States alone. It was clear to me that new approaches were needed, and I became very interested in taking advantage of the body’s immune system as a source of information to try to make progress.
Were there patients who inspired your research?
Dr. Rosenberg: There were two patients that I saw early in my career that impressed me a great deal. One was a patient that I saw when working in the emergency ward as a resident. A patient came in with right upper quadrant pain that looked like a gallbladder attack. That’s what it was. But when I went through his chart, I saw that he had been at that hospital 12 years earlier with a metastatic gastric cancer. The surgeons had operated. They saw tumor had spread to the liver and could not be removed. They closed the belly, not expecting him to survive. Yet he kept showing up for follow-up visits.
Here he was 12 years later. When I helped operate to take out his gallbladder, there was no evidence of any cancer. The cancer had disappeared in the absence of any external treatment. One of the rarest events in medicine, the spontaneous regression of a cancer. Somehow his body had learned how to destroy the tumor.
Was the second patient’s case as impressive?
Dr. Rosenberg: This patient had received a kidney transplant from a gentleman who died in an auto accident. [The donor’s] kidney contained a cancer deposit, a kidney cancer, unbeknownst to the transplant surgeons. [When the kidney was transplanted], the recipient developed widespread metastatic kidney cancer.
[The recipient] was on immunosuppressive drugs, and so the drugs had to be stopped. [When the immunosuppressive drugs were stopped], the patient’s body rejected the kidney and his cancer disappeared.
That showed me that, in fact, if you could stimulate a strong enough immune reaction, in this case, an [allogeneic] reaction, against foreign tissues from a different individual, that you could make large vascularized, invasive cancers disappear based on immune reactivities. Those were clues that led me toward studying the immune system’s impact on cancer.
From there, how did your work evolve?
Dr. Rosenberg: As chief of the surgery branch at NIH, I began doing research. It was very difficult to manipulate immune cells in the laboratory. They wouldn’t stay alive. But I tried to study immune reactions in patients with cancer to see if there was such a thing as an immune reaction against the cancer. There was no such thing known at the time. There were no cancer antigens and no known immune reactions against the disease in the human.
Around this time, investigators were publishing studies about interleukin-2 (IL-2), or white blood cells known as leukocytes. How did interleukin-2 further your research?
Dr. Rosenberg: The advent of interleukin-2 enabled scientists to grow lymphocytes outside the body. [This] enabled us to grow t-lymphocytes, which are some of the major warriors of the immune system against foreign tissue. After [studying] 66 patients in which we studied interleukin-2 and cells that would develop from it, we finally saw a disappearance of melanoma in a patient that received interleukin-2. And we went on to treat hundreds of patients with that hormone, interleukin-2. In fact, interleukin-2 became the first immunotherapy ever approved by the Food and Drug Administration for the treatment of cancer in humans.
How did this finding impact your future discoveries?
Dr. Rosenberg: [It] led to studies of the mechanism of action of interleukin-2 and to do that, we identified a kind of cell called a tumor infiltrating lymphocyte. What better place, intuitively to look for cells doing battle against the cancer than within the cancer itself?
In 1988, we demonstrated for the first time that transfer of lymphocytes with antitumor activity could cause the regression of melanoma. This was a living drug obtained from melanoma deposits that could be grown outside the body and then readministered to the patient under suitable conditions. Interestingly, [in February the FDA approved that drug as treatment for patients with melanoma]. A company developed it to the point where in multi-institutional studies, they reproduced our results.
And we’ve now emphasized the value of using T cell therapy, t cell transfer, for the treatment of patients with the common solid cancers, the cancers that start anywhere from the colon up through the intestine, the stomach, the pancreas, and the esophagus. Solid tumors such as ovarian cancer, uterine cancer and so on, are also potentially susceptible to this T cell therapy.
We’ve published several papers showing in isolated patients that you could cause major regressions, if not complete regressions, of these solid cancers in the liver, in the breast, the cervix, the colon. That’s a major aspect of what we’re doing now.
I think immunotherapy has come to be recognized as a major fourth arm that can be used to attack cancers, adding to surgery, radiation, and chemotherapy.
What guidance would you have for other physician-investigators or young doctors who want to follow in your path?
Dr. Rosenberg: You have to have a broad base of knowledge. You have to be willing to immerse yourself in a problem so that your mind is working on it when you’re doing things where you can only think. [When] you’re taking a shower, [or] waiting at a red light, your mind is working on this problem because you’re immersed in trying to understand it.
You need to have a laser focus on the goals that you have and not get sidetracked by issues that may be interesting but not directly related to the goals that you’re attempting to achieve.
His pioneering research established interleukin-2 (IL-2) as the first U.S. Food and Drug Administration–approved cancer immunotherapy in 1992.
To recognize his trailblazing work and other achievements, the American Association for Cancer Research (AACR) will award Dr. Rosenberg with the 2024 AACR Award for Lifetime Achievement in Cancer Research at its annual meeting in April.
Dr. Rosenberg, a senior investigator for the Center for Cancer Research at the National Cancer Institute (NCI), and chief of the NCI Surgery Branch, shared the history behind his novel research and the patient stories that inspired his discoveries, during an interview.
Tell us a little about yourself and where you grew up.
Dr. Rosenberg: I grew up in the Bronx. My parents both immigrated to the United States from Poland as teenagers.
As a young boy, did you always want to become a doctor?
Dr. Rosenberg: I think some defining moments on why I decided to go into medicine occurred when I was 6 or 7 years old. The second world war was over, and many of the horrors of the Holocaust became apparent to me. I was brought up as an Orthodox Jew. My parents were quite religious, and I remember postcards coming in one after another about relatives that had died in the death camps. That had a profound influence on me.
How did that experience impact your aspirations?
Dr. Rosenberg: It was an example to me of how evil certain people and groups can be toward one another. I decided at that point, that I wanted to do something good for people, and medicine seemed the most likely way to do that. But also, I was developing a broad scientific interest. I ended up at the Bronx High School of Science and knew that I not only wanted to practice the medicine of today, but I wanted to play a role in helping develop the medicine.
What led to your interest in cancer treatment?
Dr. Rosenberg: Well, as a medical student and resident, it became clear that the field of cancer needed major improvement. We had three major ways to treat cancer: surgery, radiation therapy, and chemotherapy. That could cure about half of the people [who] had cancer. But despite the best application of those three specialties, there were over 600,000 deaths from cancer each year in the United States alone. It was clear to me that new approaches were needed, and I became very interested in taking advantage of the body’s immune system as a source of information to try to make progress.
Were there patients who inspired your research?
Dr. Rosenberg: There were two patients that I saw early in my career that impressed me a great deal. One was a patient that I saw when working in the emergency ward as a resident. A patient came in with right upper quadrant pain that looked like a gallbladder attack. That’s what it was. But when I went through his chart, I saw that he had been at that hospital 12 years earlier with a metastatic gastric cancer. The surgeons had operated. They saw tumor had spread to the liver and could not be removed. They closed the belly, not expecting him to survive. Yet he kept showing up for follow-up visits.
Here he was 12 years later. When I helped operate to take out his gallbladder, there was no evidence of any cancer. The cancer had disappeared in the absence of any external treatment. One of the rarest events in medicine, the spontaneous regression of a cancer. Somehow his body had learned how to destroy the tumor.
Was the second patient’s case as impressive?
Dr. Rosenberg: This patient had received a kidney transplant from a gentleman who died in an auto accident. [The donor’s] kidney contained a cancer deposit, a kidney cancer, unbeknownst to the transplant surgeons. [When the kidney was transplanted], the recipient developed widespread metastatic kidney cancer.
[The recipient] was on immunosuppressive drugs, and so the drugs had to be stopped. [When the immunosuppressive drugs were stopped], the patient’s body rejected the kidney and his cancer disappeared.
That showed me that, in fact, if you could stimulate a strong enough immune reaction, in this case, an [allogeneic] reaction, against foreign tissues from a different individual, that you could make large vascularized, invasive cancers disappear based on immune reactivities. Those were clues that led me toward studying the immune system’s impact on cancer.
From there, how did your work evolve?
Dr. Rosenberg: As chief of the surgery branch at NIH, I began doing research. It was very difficult to manipulate immune cells in the laboratory. They wouldn’t stay alive. But I tried to study immune reactions in patients with cancer to see if there was such a thing as an immune reaction against the cancer. There was no such thing known at the time. There were no cancer antigens and no known immune reactions against the disease in the human.
Around this time, investigators were publishing studies about interleukin-2 (IL-2), or white blood cells known as leukocytes. How did interleukin-2 further your research?
Dr. Rosenberg: The advent of interleukin-2 enabled scientists to grow lymphocytes outside the body. [This] enabled us to grow t-lymphocytes, which are some of the major warriors of the immune system against foreign tissue. After [studying] 66 patients in which we studied interleukin-2 and cells that would develop from it, we finally saw a disappearance of melanoma in a patient that received interleukin-2. And we went on to treat hundreds of patients with that hormone, interleukin-2. In fact, interleukin-2 became the first immunotherapy ever approved by the Food and Drug Administration for the treatment of cancer in humans.
How did this finding impact your future discoveries?
Dr. Rosenberg: [It] led to studies of the mechanism of action of interleukin-2 and to do that, we identified a kind of cell called a tumor infiltrating lymphocyte. What better place, intuitively to look for cells doing battle against the cancer than within the cancer itself?
In 1988, we demonstrated for the first time that transfer of lymphocytes with antitumor activity could cause the regression of melanoma. This was a living drug obtained from melanoma deposits that could be grown outside the body and then readministered to the patient under suitable conditions. Interestingly, [in February the FDA approved that drug as treatment for patients with melanoma]. A company developed it to the point where in multi-institutional studies, they reproduced our results.
And we’ve now emphasized the value of using T cell therapy, t cell transfer, for the treatment of patients with the common solid cancers, the cancers that start anywhere from the colon up through the intestine, the stomach, the pancreas, and the esophagus. Solid tumors such as ovarian cancer, uterine cancer and so on, are also potentially susceptible to this T cell therapy.
We’ve published several papers showing in isolated patients that you could cause major regressions, if not complete regressions, of these solid cancers in the liver, in the breast, the cervix, the colon. That’s a major aspect of what we’re doing now.
I think immunotherapy has come to be recognized as a major fourth arm that can be used to attack cancers, adding to surgery, radiation, and chemotherapy.
What guidance would you have for other physician-investigators or young doctors who want to follow in your path?
Dr. Rosenberg: You have to have a broad base of knowledge. You have to be willing to immerse yourself in a problem so that your mind is working on it when you’re doing things where you can only think. [When] you’re taking a shower, [or] waiting at a red light, your mind is working on this problem because you’re immersed in trying to understand it.
You need to have a laser focus on the goals that you have and not get sidetracked by issues that may be interesting but not directly related to the goals that you’re attempting to achieve.
His pioneering research established interleukin-2 (IL-2) as the first U.S. Food and Drug Administration–approved cancer immunotherapy in 1992.
To recognize his trailblazing work and other achievements, the American Association for Cancer Research (AACR) will award Dr. Rosenberg with the 2024 AACR Award for Lifetime Achievement in Cancer Research at its annual meeting in April.
Dr. Rosenberg, a senior investigator for the Center for Cancer Research at the National Cancer Institute (NCI), and chief of the NCI Surgery Branch, shared the history behind his novel research and the patient stories that inspired his discoveries, during an interview.
Tell us a little about yourself and where you grew up.
Dr. Rosenberg: I grew up in the Bronx. My parents both immigrated to the United States from Poland as teenagers.
As a young boy, did you always want to become a doctor?
Dr. Rosenberg: I think some defining moments on why I decided to go into medicine occurred when I was 6 or 7 years old. The second world war was over, and many of the horrors of the Holocaust became apparent to me. I was brought up as an Orthodox Jew. My parents were quite religious, and I remember postcards coming in one after another about relatives that had died in the death camps. That had a profound influence on me.
How did that experience impact your aspirations?
Dr. Rosenberg: It was an example to me of how evil certain people and groups can be toward one another. I decided at that point, that I wanted to do something good for people, and medicine seemed the most likely way to do that. But also, I was developing a broad scientific interest. I ended up at the Bronx High School of Science and knew that I not only wanted to practice the medicine of today, but I wanted to play a role in helping develop the medicine.
What led to your interest in cancer treatment?
Dr. Rosenberg: Well, as a medical student and resident, it became clear that the field of cancer needed major improvement. We had three major ways to treat cancer: surgery, radiation therapy, and chemotherapy. That could cure about half of the people [who] had cancer. But despite the best application of those three specialties, there were over 600,000 deaths from cancer each year in the United States alone. It was clear to me that new approaches were needed, and I became very interested in taking advantage of the body’s immune system as a source of information to try to make progress.
Were there patients who inspired your research?
Dr. Rosenberg: There were two patients that I saw early in my career that impressed me a great deal. One was a patient that I saw when working in the emergency ward as a resident. A patient came in with right upper quadrant pain that looked like a gallbladder attack. That’s what it was. But when I went through his chart, I saw that he had been at that hospital 12 years earlier with a metastatic gastric cancer. The surgeons had operated. They saw tumor had spread to the liver and could not be removed. They closed the belly, not expecting him to survive. Yet he kept showing up for follow-up visits.
Here he was 12 years later. When I helped operate to take out his gallbladder, there was no evidence of any cancer. The cancer had disappeared in the absence of any external treatment. One of the rarest events in medicine, the spontaneous regression of a cancer. Somehow his body had learned how to destroy the tumor.
Was the second patient’s case as impressive?
Dr. Rosenberg: This patient had received a kidney transplant from a gentleman who died in an auto accident. [The donor’s] kidney contained a cancer deposit, a kidney cancer, unbeknownst to the transplant surgeons. [When the kidney was transplanted], the recipient developed widespread metastatic kidney cancer.
[The recipient] was on immunosuppressive drugs, and so the drugs had to be stopped. [When the immunosuppressive drugs were stopped], the patient’s body rejected the kidney and his cancer disappeared.
That showed me that, in fact, if you could stimulate a strong enough immune reaction, in this case, an [allogeneic] reaction, against foreign tissues from a different individual, that you could make large vascularized, invasive cancers disappear based on immune reactivities. Those were clues that led me toward studying the immune system’s impact on cancer.
From there, how did your work evolve?
Dr. Rosenberg: As chief of the surgery branch at NIH, I began doing research. It was very difficult to manipulate immune cells in the laboratory. They wouldn’t stay alive. But I tried to study immune reactions in patients with cancer to see if there was such a thing as an immune reaction against the cancer. There was no such thing known at the time. There were no cancer antigens and no known immune reactions against the disease in the human.
Around this time, investigators were publishing studies about interleukin-2 (IL-2), or white blood cells known as leukocytes. How did interleukin-2 further your research?
Dr. Rosenberg: The advent of interleukin-2 enabled scientists to grow lymphocytes outside the body. [This] enabled us to grow t-lymphocytes, which are some of the major warriors of the immune system against foreign tissue. After [studying] 66 patients in which we studied interleukin-2 and cells that would develop from it, we finally saw a disappearance of melanoma in a patient that received interleukin-2. And we went on to treat hundreds of patients with that hormone, interleukin-2. In fact, interleukin-2 became the first immunotherapy ever approved by the Food and Drug Administration for the treatment of cancer in humans.
How did this finding impact your future discoveries?
Dr. Rosenberg: [It] led to studies of the mechanism of action of interleukin-2 and to do that, we identified a kind of cell called a tumor infiltrating lymphocyte. What better place, intuitively to look for cells doing battle against the cancer than within the cancer itself?
In 1988, we demonstrated for the first time that transfer of lymphocytes with antitumor activity could cause the regression of melanoma. This was a living drug obtained from melanoma deposits that could be grown outside the body and then readministered to the patient under suitable conditions. Interestingly, [in February the FDA approved that drug as treatment for patients with melanoma]. A company developed it to the point where in multi-institutional studies, they reproduced our results.
And we’ve now emphasized the value of using T cell therapy, t cell transfer, for the treatment of patients with the common solid cancers, the cancers that start anywhere from the colon up through the intestine, the stomach, the pancreas, and the esophagus. Solid tumors such as ovarian cancer, uterine cancer and so on, are also potentially susceptible to this T cell therapy.
We’ve published several papers showing in isolated patients that you could cause major regressions, if not complete regressions, of these solid cancers in the liver, in the breast, the cervix, the colon. That’s a major aspect of what we’re doing now.
I think immunotherapy has come to be recognized as a major fourth arm that can be used to attack cancers, adding to surgery, radiation, and chemotherapy.
What guidance would you have for other physician-investigators or young doctors who want to follow in your path?
Dr. Rosenberg: You have to have a broad base of knowledge. You have to be willing to immerse yourself in a problem so that your mind is working on it when you’re doing things where you can only think. [When] you’re taking a shower, [or] waiting at a red light, your mind is working on this problem because you’re immersed in trying to understand it.
You need to have a laser focus on the goals that you have and not get sidetracked by issues that may be interesting but not directly related to the goals that you’re attempting to achieve.
Combining Targeted Drugs and Radiation in Breast Cancer: What’s Safe?
One reason is studies of new drugs typically exclude concurrent radiotherapy, said Kathy Miller, MD, a contributor to this news organization and professor of oncology and medicine at the Indiana University School of Medicine, Indianapolis, Indiana.
If trials evaluating new targeted therapies included concurrent radiotherapy, it would be challenging to identify whether toxicities came from the drug itself, the radiation, or the combination, Dr. Miller explained.
Given the limited evidence, “we tend to be cautious and conservative” and not combine therapies that “we don’t know are safe or appropriate for patients,” said Chirag Shah, MD, director of breast radiology at the Cleveland Clinic, Cleveland, Ohio.
Below is a guide to what we do and don’t know about combining radiotherapy and systemic treatments in breast cancer.
1. Immunotherapy plus radiotherapy likely safe but evidence is limited
Safety data on combining immune checkpoint inhibitors and radiotherapy in breast cancer are limited because concurrent radiotherapy has typically been excluded in pivotal trials.
The 2020 KEYNOTE-522 trial did provide a rare look at concurrent radiotherapy and immunotherapy in early triple-negative breast cancer. The analysis found “no safety concerns” with concurrent radiotherapy and pembrolizumab, lead investigator Peter Schmid, MD, of Queen Mary University of London, England, told this news organization.
Research on other solid tumor types also suggests that radiotherapy “can be considered safe” alongside immunotherapy, the authors of a recent ESTRO consensus said.
Despite evidence indicating radiotherapy alongside immunotherapy can be safe in patients with breast cancer, “certain aspects, such as patient selection, total dose, and dose per fraction, remain open for debate to achieve the best therapeutic outcomes,” the ESTRO experts cautioned.
2. CDK4/6 inhibitors may be offered with radiotherapy in some settings, not others
CDK4/6 inhibitors are now standard of care for first- or second-line treatment in patients with advanced or metastatic hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)–negative breast cancer.
“Unfortunately, we found no information regarding concurrent radiotherapy in the adjuvant setting” in pivotal trials for palbociclib, abemaciclib, and ribociclib, the ESTRO authors said. In the pivotal trials for palbociclib and abemaciclib, patients had to discontinue immunotherapy before initiating radiotherapy, and in the trial for ribociclib, palliative radiotherapy was allowed for relieving bone pain only.
However, in 2023, a team of experts from 12 countries attempted to piece together the available evidence, publishing a meta-analysis of 11 retrospective studies on the safety of CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic disease.
Although most of these studies had small patient populations, the analysis revealed that CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic breast cancer led to a similar side-effect profile to that observed in trials of the inhibitors given sequentially with adjuvant radiotherapy.
“These findings suggest that the simultaneous administration of CDK4/6 inhibitors and radiotherapy is generally well tolerated,” the ESTRO authors concluded but added that CDK4/6 inhibitors and concomitant radiotherapy should be investigated more in the adjuvant locoregional, whole brain, and intracranial stereotactic radiotherapy settings.
The expert panel did note, however, that CDK4/6 inhibitors and concomitant radiotherapy “could be offered” during palliative and ablative extracranial radiotherapy.
3. Only offer poly (ADP-ribose) polymerase (PARP) inhibitors plus radiotherapy in clinical trial setting
PARP inhibitors olaparib (Lynparza) and talazoprib (Talzenna) are standard of care in patients with metastatic breast cancer who have BRCA1/2 gene mutations. Olaparib is also indicated for high-risk early breast cancer following neoadjuvant or adjuvant chemotherapy.
But data on combining PARP inhibitors with radiotherapy in breast cancer also remain limited.
One ongoing phase 2 trial, comparing olaparib plus radiotherapy to radiotherapy alone in 300 people with inflammatory breast cancer, is aiming to tease out the safety of the combination and whether it improves local control in patients with aggressive disease.
“The desire is to explore the exciting possibility that low doses of PARP inhibition may radiosensitize tumor cells more than normal tissues,” Reshma Jagsi, MD, chair of the Department of Radiation Oncology at Emory University School of Medicine in Atlanta, Georgia, who is leading the study.
Because of potential good or bad interactions between new systemic therapies and radiotherapy, “intentional trial design” is important, Dr. Jagsi said, so we “know the best way to combine treatments in practice to optimize outcomes.”
But given the evidence to date, the ESTRO experts advised waiting until “further research provides more comprehensive safety and efficacy data” in the primary, adjuvant, and metastatic settings. The experts also advised not offering PARP inhibitors and concomitant radiotherapy to treat advanced breast cancer outside of clinical trials.
4. Phosphoinositide 3-kinase inhibitors (PI3K) inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and newer targeted agents should not be offered concurrently with radiotherapy
Clinical trial data on the safety of combining PI3K and mTOR inhibitors with radiation are thin, especially in advanced breast cancer. Typically, radiotherapy within 4 weeks before randomization, or 2 weeks for palliative radiation, was excluded in pivotal trials.
For this reason, the ESTRO team recommended that concurrent radiation with either PI3K inhibitors or mTOR inhibitors “should not be offered.”
ESTRO also cautioned against providing radiation concurrently with newer anti-HER2 tyrosine-kinase drugs, such as neratinib or tucatinib, or newer antibody-drug conjugates such as trastuzumab deruxtecan, until more data emerge on the safety of these combinations.
5. Combining older HER2-targeted drugs and radiotherapy generally safe
The ESTRO authors agreed that older anti-HER2 drugs trastuzumab (Herceptin), pertuzumab (Perjeta), and lapatinib (Tykerb) can be safely used concurrently with locoregional radiotherapy as well.
One of the biggest concerns in the field is how to combine radiation with systemic therapies in the setting of brain metastases, and the data on these older anti-HER2 drugs are relatively clear that it’s safe, Dr. Miller said.
For instance, in a 2019 study of 84 patients with 487 brain metastases, stereotactic radiosurgery given alongside lapatinib led to significantly higher rates of complete responses than stereotactic radiosurgery alone (35% vs 11%) with no increased risk for radiation necrosis.
The ESTRO team agreed, noting that the latest evidence supports the use of trastuzumab, pertuzumab, or lapatinib alongside radiotherapy for whole brain and ablative intracranial stereotactic radiotherapy.
As for older antibody-drug conjugates, trastuzumab emtansine (T-DM1) plus radiotherapy “might be considered” during adjuvant locoregional radiotherapy for breast cancer but should not be offered for whole brain and ablative intracranial stereotactic radiotherapy, the ESTRO team said.
Dr. Jagsi declared the following conflicts in a recent 2024 publication: Stock options for advisory board role in Equity Quotient; grants or contracts from Genentech; and expert witness for Kleinbard, LLC, and Hawks Quindel Law. In the Keynote-522 trial publication Dr. Schmid declared relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Celgene, Eisai, Hoffmann-La Roche, Genetech, Merck, Novartis, and Pfizer. Dr. Shah reported consulting for Impedimed, Videra Surgical, and PreludeDX.
A version of this article appeared on Medscape.com.
One reason is studies of new drugs typically exclude concurrent radiotherapy, said Kathy Miller, MD, a contributor to this news organization and professor of oncology and medicine at the Indiana University School of Medicine, Indianapolis, Indiana.
If trials evaluating new targeted therapies included concurrent radiotherapy, it would be challenging to identify whether toxicities came from the drug itself, the radiation, or the combination, Dr. Miller explained.
Given the limited evidence, “we tend to be cautious and conservative” and not combine therapies that “we don’t know are safe or appropriate for patients,” said Chirag Shah, MD, director of breast radiology at the Cleveland Clinic, Cleveland, Ohio.
Below is a guide to what we do and don’t know about combining radiotherapy and systemic treatments in breast cancer.
1. Immunotherapy plus radiotherapy likely safe but evidence is limited
Safety data on combining immune checkpoint inhibitors and radiotherapy in breast cancer are limited because concurrent radiotherapy has typically been excluded in pivotal trials.
The 2020 KEYNOTE-522 trial did provide a rare look at concurrent radiotherapy and immunotherapy in early triple-negative breast cancer. The analysis found “no safety concerns” with concurrent radiotherapy and pembrolizumab, lead investigator Peter Schmid, MD, of Queen Mary University of London, England, told this news organization.
Research on other solid tumor types also suggests that radiotherapy “can be considered safe” alongside immunotherapy, the authors of a recent ESTRO consensus said.
Despite evidence indicating radiotherapy alongside immunotherapy can be safe in patients with breast cancer, “certain aspects, such as patient selection, total dose, and dose per fraction, remain open for debate to achieve the best therapeutic outcomes,” the ESTRO experts cautioned.
2. CDK4/6 inhibitors may be offered with radiotherapy in some settings, not others
CDK4/6 inhibitors are now standard of care for first- or second-line treatment in patients with advanced or metastatic hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)–negative breast cancer.
“Unfortunately, we found no information regarding concurrent radiotherapy in the adjuvant setting” in pivotal trials for palbociclib, abemaciclib, and ribociclib, the ESTRO authors said. In the pivotal trials for palbociclib and abemaciclib, patients had to discontinue immunotherapy before initiating radiotherapy, and in the trial for ribociclib, palliative radiotherapy was allowed for relieving bone pain only.
However, in 2023, a team of experts from 12 countries attempted to piece together the available evidence, publishing a meta-analysis of 11 retrospective studies on the safety of CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic disease.
Although most of these studies had small patient populations, the analysis revealed that CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic breast cancer led to a similar side-effect profile to that observed in trials of the inhibitors given sequentially with adjuvant radiotherapy.
“These findings suggest that the simultaneous administration of CDK4/6 inhibitors and radiotherapy is generally well tolerated,” the ESTRO authors concluded but added that CDK4/6 inhibitors and concomitant radiotherapy should be investigated more in the adjuvant locoregional, whole brain, and intracranial stereotactic radiotherapy settings.
The expert panel did note, however, that CDK4/6 inhibitors and concomitant radiotherapy “could be offered” during palliative and ablative extracranial radiotherapy.
3. Only offer poly (ADP-ribose) polymerase (PARP) inhibitors plus radiotherapy in clinical trial setting
PARP inhibitors olaparib (Lynparza) and talazoprib (Talzenna) are standard of care in patients with metastatic breast cancer who have BRCA1/2 gene mutations. Olaparib is also indicated for high-risk early breast cancer following neoadjuvant or adjuvant chemotherapy.
But data on combining PARP inhibitors with radiotherapy in breast cancer also remain limited.
One ongoing phase 2 trial, comparing olaparib plus radiotherapy to radiotherapy alone in 300 people with inflammatory breast cancer, is aiming to tease out the safety of the combination and whether it improves local control in patients with aggressive disease.
“The desire is to explore the exciting possibility that low doses of PARP inhibition may radiosensitize tumor cells more than normal tissues,” Reshma Jagsi, MD, chair of the Department of Radiation Oncology at Emory University School of Medicine in Atlanta, Georgia, who is leading the study.
Because of potential good or bad interactions between new systemic therapies and radiotherapy, “intentional trial design” is important, Dr. Jagsi said, so we “know the best way to combine treatments in practice to optimize outcomes.”
But given the evidence to date, the ESTRO experts advised waiting until “further research provides more comprehensive safety and efficacy data” in the primary, adjuvant, and metastatic settings. The experts also advised not offering PARP inhibitors and concomitant radiotherapy to treat advanced breast cancer outside of clinical trials.
4. Phosphoinositide 3-kinase inhibitors (PI3K) inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and newer targeted agents should not be offered concurrently with radiotherapy
Clinical trial data on the safety of combining PI3K and mTOR inhibitors with radiation are thin, especially in advanced breast cancer. Typically, radiotherapy within 4 weeks before randomization, or 2 weeks for palliative radiation, was excluded in pivotal trials.
For this reason, the ESTRO team recommended that concurrent radiation with either PI3K inhibitors or mTOR inhibitors “should not be offered.”
ESTRO also cautioned against providing radiation concurrently with newer anti-HER2 tyrosine-kinase drugs, such as neratinib or tucatinib, or newer antibody-drug conjugates such as trastuzumab deruxtecan, until more data emerge on the safety of these combinations.
5. Combining older HER2-targeted drugs and radiotherapy generally safe
The ESTRO authors agreed that older anti-HER2 drugs trastuzumab (Herceptin), pertuzumab (Perjeta), and lapatinib (Tykerb) can be safely used concurrently with locoregional radiotherapy as well.
One of the biggest concerns in the field is how to combine radiation with systemic therapies in the setting of brain metastases, and the data on these older anti-HER2 drugs are relatively clear that it’s safe, Dr. Miller said.
For instance, in a 2019 study of 84 patients with 487 brain metastases, stereotactic radiosurgery given alongside lapatinib led to significantly higher rates of complete responses than stereotactic radiosurgery alone (35% vs 11%) with no increased risk for radiation necrosis.
The ESTRO team agreed, noting that the latest evidence supports the use of trastuzumab, pertuzumab, or lapatinib alongside radiotherapy for whole brain and ablative intracranial stereotactic radiotherapy.
As for older antibody-drug conjugates, trastuzumab emtansine (T-DM1) plus radiotherapy “might be considered” during adjuvant locoregional radiotherapy for breast cancer but should not be offered for whole brain and ablative intracranial stereotactic radiotherapy, the ESTRO team said.
Dr. Jagsi declared the following conflicts in a recent 2024 publication: Stock options for advisory board role in Equity Quotient; grants or contracts from Genentech; and expert witness for Kleinbard, LLC, and Hawks Quindel Law. In the Keynote-522 trial publication Dr. Schmid declared relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Celgene, Eisai, Hoffmann-La Roche, Genetech, Merck, Novartis, and Pfizer. Dr. Shah reported consulting for Impedimed, Videra Surgical, and PreludeDX.
A version of this article appeared on Medscape.com.
One reason is studies of new drugs typically exclude concurrent radiotherapy, said Kathy Miller, MD, a contributor to this news organization and professor of oncology and medicine at the Indiana University School of Medicine, Indianapolis, Indiana.
If trials evaluating new targeted therapies included concurrent radiotherapy, it would be challenging to identify whether toxicities came from the drug itself, the radiation, or the combination, Dr. Miller explained.
Given the limited evidence, “we tend to be cautious and conservative” and not combine therapies that “we don’t know are safe or appropriate for patients,” said Chirag Shah, MD, director of breast radiology at the Cleveland Clinic, Cleveland, Ohio.
Below is a guide to what we do and don’t know about combining radiotherapy and systemic treatments in breast cancer.
1. Immunotherapy plus radiotherapy likely safe but evidence is limited
Safety data on combining immune checkpoint inhibitors and radiotherapy in breast cancer are limited because concurrent radiotherapy has typically been excluded in pivotal trials.
The 2020 KEYNOTE-522 trial did provide a rare look at concurrent radiotherapy and immunotherapy in early triple-negative breast cancer. The analysis found “no safety concerns” with concurrent radiotherapy and pembrolizumab, lead investigator Peter Schmid, MD, of Queen Mary University of London, England, told this news organization.
Research on other solid tumor types also suggests that radiotherapy “can be considered safe” alongside immunotherapy, the authors of a recent ESTRO consensus said.
Despite evidence indicating radiotherapy alongside immunotherapy can be safe in patients with breast cancer, “certain aspects, such as patient selection, total dose, and dose per fraction, remain open for debate to achieve the best therapeutic outcomes,” the ESTRO experts cautioned.
2. CDK4/6 inhibitors may be offered with radiotherapy in some settings, not others
CDK4/6 inhibitors are now standard of care for first- or second-line treatment in patients with advanced or metastatic hormone receptor–positive, human epidermal growth factor receptor 2 (HER2)–negative breast cancer.
“Unfortunately, we found no information regarding concurrent radiotherapy in the adjuvant setting” in pivotal trials for palbociclib, abemaciclib, and ribociclib, the ESTRO authors said. In the pivotal trials for palbociclib and abemaciclib, patients had to discontinue immunotherapy before initiating radiotherapy, and in the trial for ribociclib, palliative radiotherapy was allowed for relieving bone pain only.
However, in 2023, a team of experts from 12 countries attempted to piece together the available evidence, publishing a meta-analysis of 11 retrospective studies on the safety of CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic disease.
Although most of these studies had small patient populations, the analysis revealed that CDK4/6 inhibitors given concurrently with radiotherapy in patients with metastatic breast cancer led to a similar side-effect profile to that observed in trials of the inhibitors given sequentially with adjuvant radiotherapy.
“These findings suggest that the simultaneous administration of CDK4/6 inhibitors and radiotherapy is generally well tolerated,” the ESTRO authors concluded but added that CDK4/6 inhibitors and concomitant radiotherapy should be investigated more in the adjuvant locoregional, whole brain, and intracranial stereotactic radiotherapy settings.
The expert panel did note, however, that CDK4/6 inhibitors and concomitant radiotherapy “could be offered” during palliative and ablative extracranial radiotherapy.
3. Only offer poly (ADP-ribose) polymerase (PARP) inhibitors plus radiotherapy in clinical trial setting
PARP inhibitors olaparib (Lynparza) and talazoprib (Talzenna) are standard of care in patients with metastatic breast cancer who have BRCA1/2 gene mutations. Olaparib is also indicated for high-risk early breast cancer following neoadjuvant or adjuvant chemotherapy.
But data on combining PARP inhibitors with radiotherapy in breast cancer also remain limited.
One ongoing phase 2 trial, comparing olaparib plus radiotherapy to radiotherapy alone in 300 people with inflammatory breast cancer, is aiming to tease out the safety of the combination and whether it improves local control in patients with aggressive disease.
“The desire is to explore the exciting possibility that low doses of PARP inhibition may radiosensitize tumor cells more than normal tissues,” Reshma Jagsi, MD, chair of the Department of Radiation Oncology at Emory University School of Medicine in Atlanta, Georgia, who is leading the study.
Because of potential good or bad interactions between new systemic therapies and radiotherapy, “intentional trial design” is important, Dr. Jagsi said, so we “know the best way to combine treatments in practice to optimize outcomes.”
But given the evidence to date, the ESTRO experts advised waiting until “further research provides more comprehensive safety and efficacy data” in the primary, adjuvant, and metastatic settings. The experts also advised not offering PARP inhibitors and concomitant radiotherapy to treat advanced breast cancer outside of clinical trials.
4. Phosphoinositide 3-kinase inhibitors (PI3K) inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and newer targeted agents should not be offered concurrently with radiotherapy
Clinical trial data on the safety of combining PI3K and mTOR inhibitors with radiation are thin, especially in advanced breast cancer. Typically, radiotherapy within 4 weeks before randomization, or 2 weeks for palliative radiation, was excluded in pivotal trials.
For this reason, the ESTRO team recommended that concurrent radiation with either PI3K inhibitors or mTOR inhibitors “should not be offered.”
ESTRO also cautioned against providing radiation concurrently with newer anti-HER2 tyrosine-kinase drugs, such as neratinib or tucatinib, or newer antibody-drug conjugates such as trastuzumab deruxtecan, until more data emerge on the safety of these combinations.
5. Combining older HER2-targeted drugs and radiotherapy generally safe
The ESTRO authors agreed that older anti-HER2 drugs trastuzumab (Herceptin), pertuzumab (Perjeta), and lapatinib (Tykerb) can be safely used concurrently with locoregional radiotherapy as well.
One of the biggest concerns in the field is how to combine radiation with systemic therapies in the setting of brain metastases, and the data on these older anti-HER2 drugs are relatively clear that it’s safe, Dr. Miller said.
For instance, in a 2019 study of 84 patients with 487 brain metastases, stereotactic radiosurgery given alongside lapatinib led to significantly higher rates of complete responses than stereotactic radiosurgery alone (35% vs 11%) with no increased risk for radiation necrosis.
The ESTRO team agreed, noting that the latest evidence supports the use of trastuzumab, pertuzumab, or lapatinib alongside radiotherapy for whole brain and ablative intracranial stereotactic radiotherapy.
As for older antibody-drug conjugates, trastuzumab emtansine (T-DM1) plus radiotherapy “might be considered” during adjuvant locoregional radiotherapy for breast cancer but should not be offered for whole brain and ablative intracranial stereotactic radiotherapy, the ESTRO team said.
Dr. Jagsi declared the following conflicts in a recent 2024 publication: Stock options for advisory board role in Equity Quotient; grants or contracts from Genentech; and expert witness for Kleinbard, LLC, and Hawks Quindel Law. In the Keynote-522 trial publication Dr. Schmid declared relationships with AstraZeneca, Bayer, Boehringer Ingelheim, Celgene, Eisai, Hoffmann-La Roche, Genetech, Merck, Novartis, and Pfizer. Dr. Shah reported consulting for Impedimed, Videra Surgical, and PreludeDX.
A version of this article appeared on Medscape.com.
Cancer Data Trends 2024: Breast Cancer
1. US Department of Veterans Affairs. Mammogram/breast health. March 28, 2022. Accessed January 10, 2024. https://www.womenshealth.va.gov/topics/mammogram-breast-health.asp
2. First anniversary of Mammography and Medical Options Act (MAMMO Act). VA News. June 6, 2023. Accessed January 10, 2024. https://news.va.gov/120476/anniversary-mammography-and-medicaloptions-act/
3. Moss HA, Rasmussen, KM, Patil, V, et al. Demographic characteristics of veterans diagnosed with breast and gynecologic cancers: a comparative analysis with the general population. Abstract presented at: Annual Meeting of the Association of VA Hematology/ Oncology (AVAHO); September 29–October 1, 2023; Chicago, IL. Abstract 47.
4. US Department of Veterans Affairs. Racial and ethnic minority veterans. Updated July 9, 2020. Accessed January 10, 2024. https:// www.va.gov/HEALTHEQUITY/Race_Ethnicity.asp
5. Stringer-Reasor EM, Elkhanany A, Khoury K, Simon MA, Newman LA. Disparities in breast cancer associated with African American identity. Am Soc Clin Oncol Educ Book. 2021;41:e29-e46. doi:10.1200/EDBK_319929
6. Landry I, Sumbly V, Vest M. Advancements in the treatment of triple- CANCER DATA TRENDS 2024 MARCH 2024 • FEDERAL PRACTITIONER negative breast cancer: a narrative review of the literature. Cureus. 2022;14(2):e21970. doi:10.7759/cureus.21970
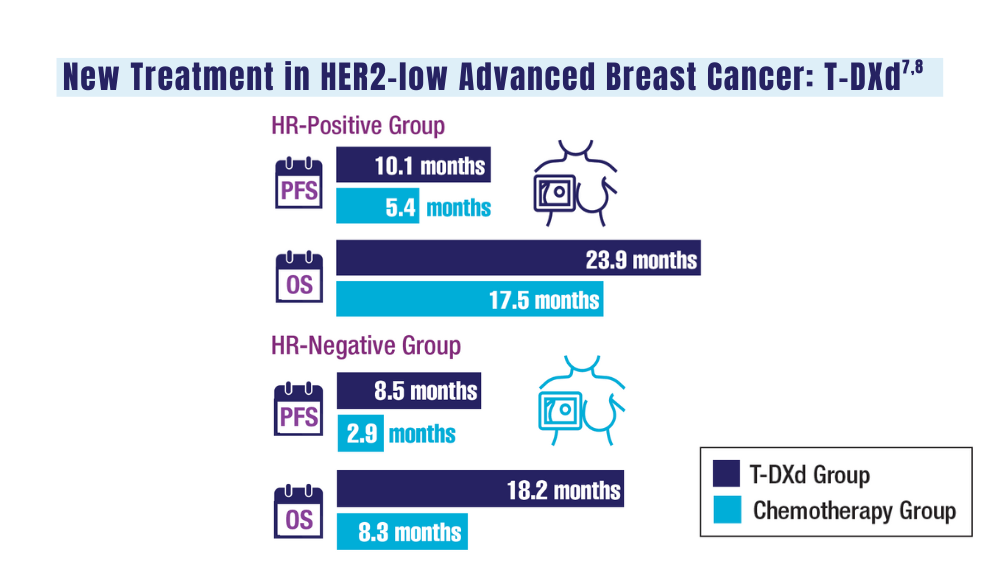
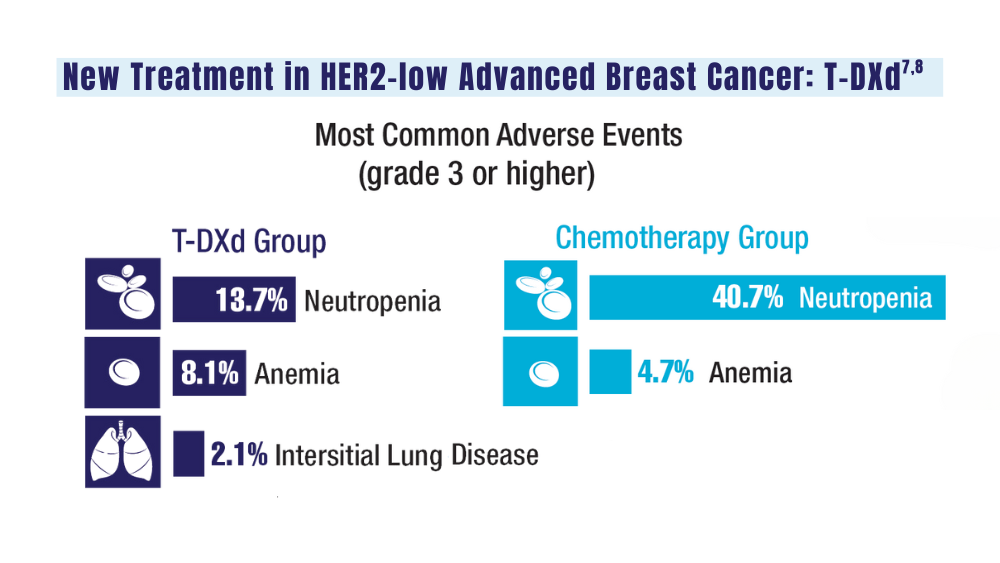
7. Schlam I, Tolaney SM, Tarantino P. How I treat HER2-low advanced breast cancer. Breast. 2023;67:116-123. doi:10.1016/j.breast.2023.01.005
8. Modi S, Jacot W, Yamashita T, et al; for the DESTINY-Breast04 Trial Investigators. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9-20. doi:10.1056/NEJMoa2203690
1. US Department of Veterans Affairs. Mammogram/breast health. March 28, 2022. Accessed January 10, 2024. https://www.womenshealth.va.gov/topics/mammogram-breast-health.asp
2. First anniversary of Mammography and Medical Options Act (MAMMO Act). VA News. June 6, 2023. Accessed January 10, 2024. https://news.va.gov/120476/anniversary-mammography-and-medicaloptions-act/
3. Moss HA, Rasmussen, KM, Patil, V, et al. Demographic characteristics of veterans diagnosed with breast and gynecologic cancers: a comparative analysis with the general population. Abstract presented at: Annual Meeting of the Association of VA Hematology/ Oncology (AVAHO); September 29–October 1, 2023; Chicago, IL. Abstract 47.
4. US Department of Veterans Affairs. Racial and ethnic minority veterans. Updated July 9, 2020. Accessed January 10, 2024. https:// www.va.gov/HEALTHEQUITY/Race_Ethnicity.asp
5. Stringer-Reasor EM, Elkhanany A, Khoury K, Simon MA, Newman LA. Disparities in breast cancer associated with African American identity. Am Soc Clin Oncol Educ Book. 2021;41:e29-e46. doi:10.1200/EDBK_319929
6. Landry I, Sumbly V, Vest M. Advancements in the treatment of triple- CANCER DATA TRENDS 2024 MARCH 2024 • FEDERAL PRACTITIONER negative breast cancer: a narrative review of the literature. Cureus. 2022;14(2):e21970. doi:10.7759/cureus.21970
7. Schlam I, Tolaney SM, Tarantino P. How I treat HER2-low advanced breast cancer. Breast. 2023;67:116-123. doi:10.1016/j.breast.2023.01.005
8. Modi S, Jacot W, Yamashita T, et al; for the DESTINY-Breast04 Trial Investigators. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9-20. doi:10.1056/NEJMoa2203690
1. US Department of Veterans Affairs. Mammogram/breast health. March 28, 2022. Accessed January 10, 2024. https://www.womenshealth.va.gov/topics/mammogram-breast-health.asp
2. First anniversary of Mammography and Medical Options Act (MAMMO Act). VA News. June 6, 2023. Accessed January 10, 2024. https://news.va.gov/120476/anniversary-mammography-and-medicaloptions-act/
3. Moss HA, Rasmussen, KM, Patil, V, et al. Demographic characteristics of veterans diagnosed with breast and gynecologic cancers: a comparative analysis with the general population. Abstract presented at: Annual Meeting of the Association of VA Hematology/ Oncology (AVAHO); September 29–October 1, 2023; Chicago, IL. Abstract 47.
4. US Department of Veterans Affairs. Racial and ethnic minority veterans. Updated July 9, 2020. Accessed January 10, 2024. https:// www.va.gov/HEALTHEQUITY/Race_Ethnicity.asp
5. Stringer-Reasor EM, Elkhanany A, Khoury K, Simon MA, Newman LA. Disparities in breast cancer associated with African American identity. Am Soc Clin Oncol Educ Book. 2021;41:e29-e46. doi:10.1200/EDBK_319929
6. Landry I, Sumbly V, Vest M. Advancements in the treatment of triple- CANCER DATA TRENDS 2024 MARCH 2024 • FEDERAL PRACTITIONER negative breast cancer: a narrative review of the literature. Cureus. 2022;14(2):e21970. doi:10.7759/cureus.21970
7. Schlam I, Tolaney SM, Tarantino P. How I treat HER2-low advanced breast cancer. Breast. 2023;67:116-123. doi:10.1016/j.breast.2023.01.005
8. Modi S, Jacot W, Yamashita T, et al; for the DESTINY-Breast04 Trial Investigators. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9-20. doi:10.1056/NEJMoa2203690
Cancer Data Trends 2024

The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
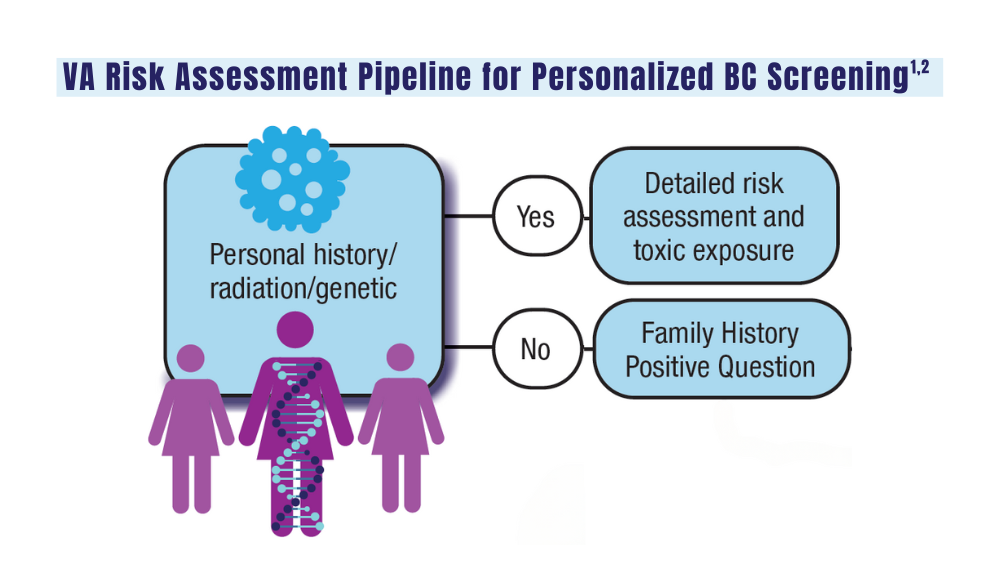
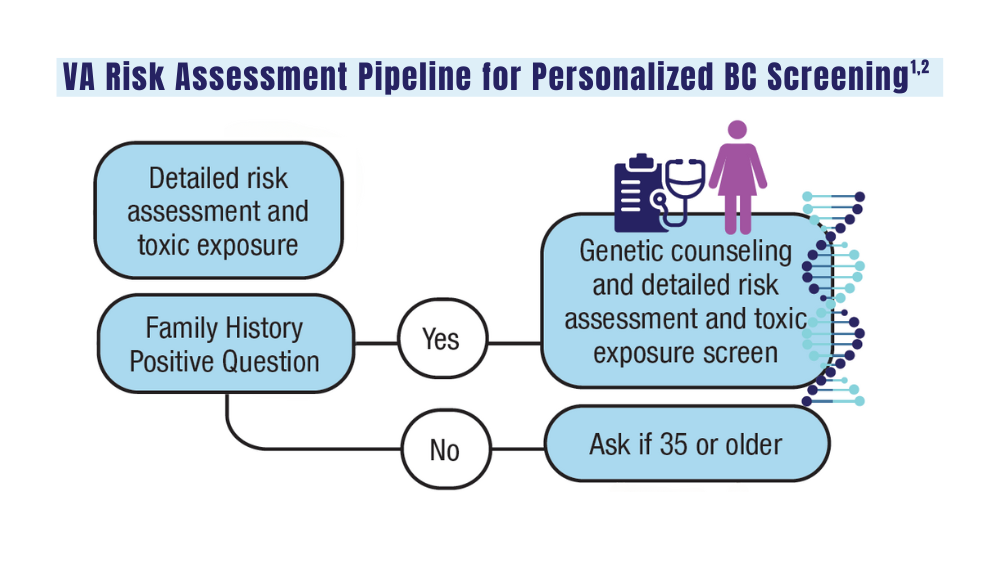
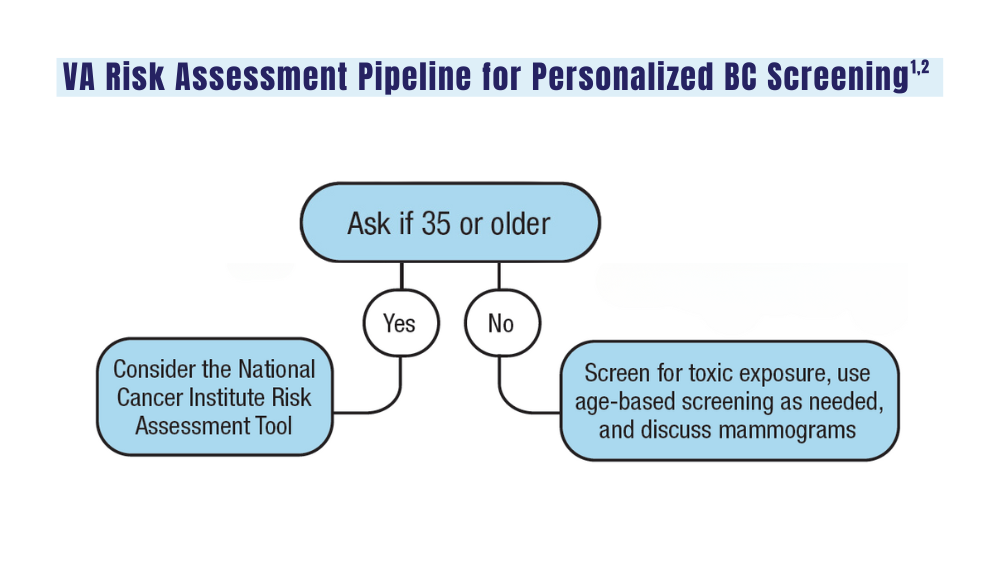
Breast Cancer
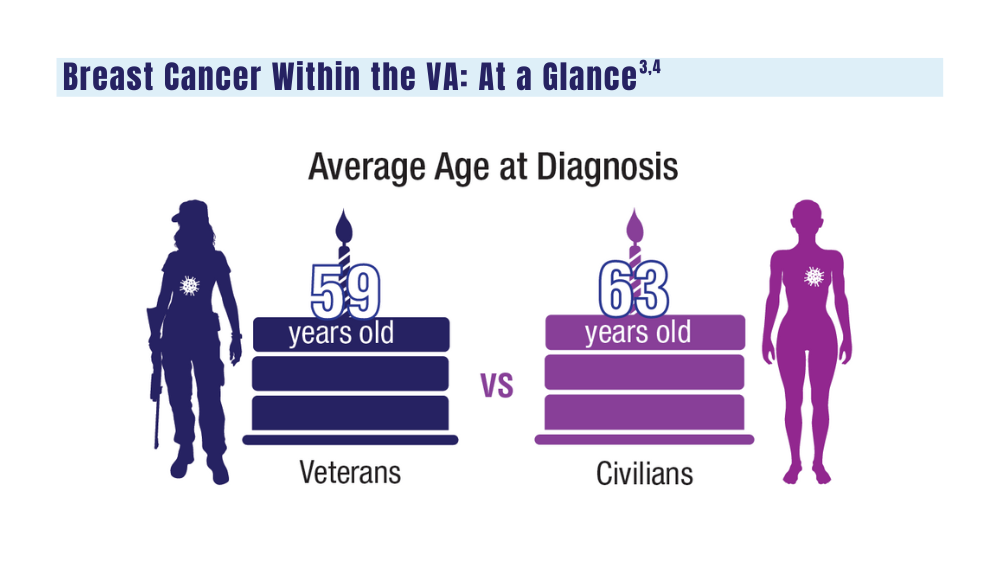
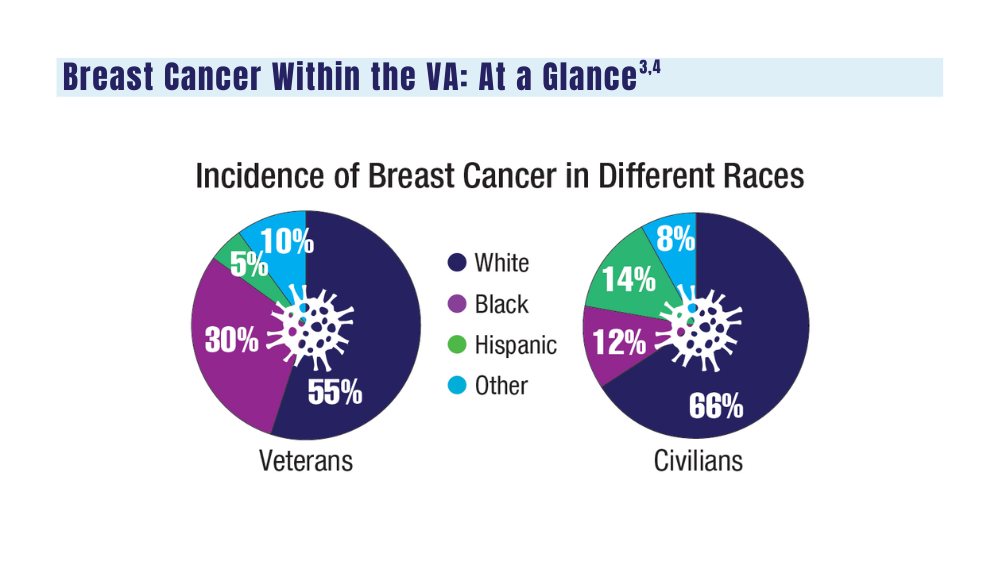
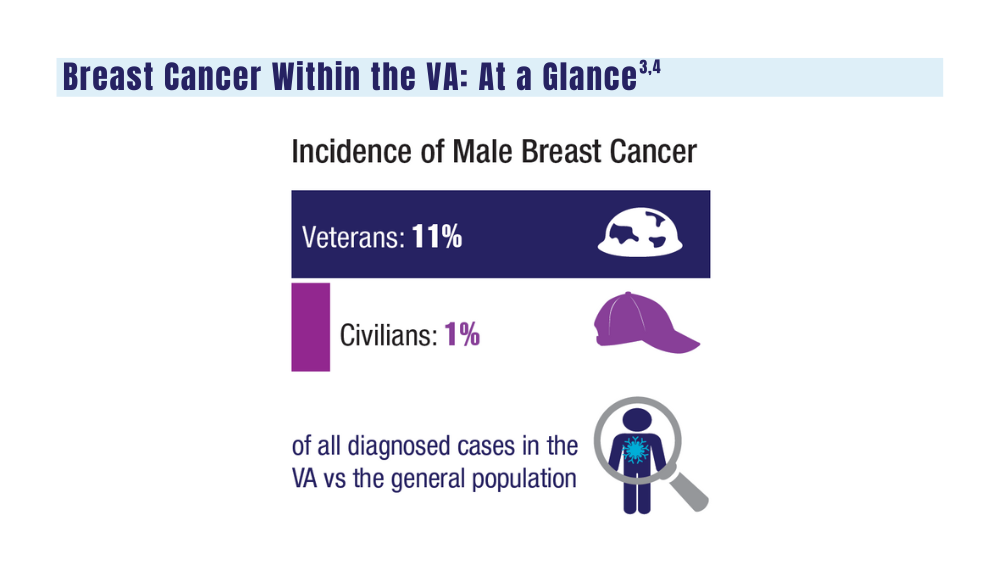
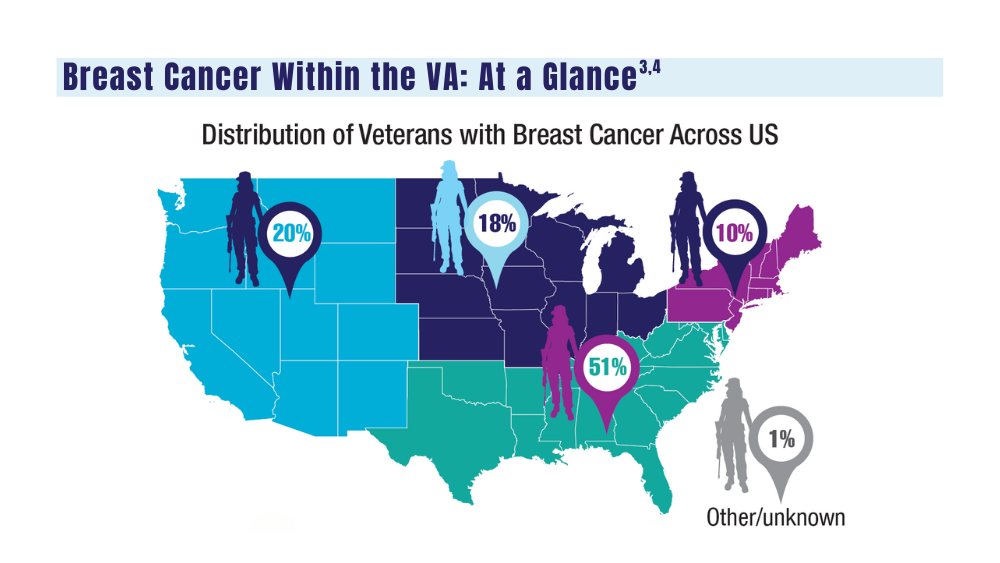
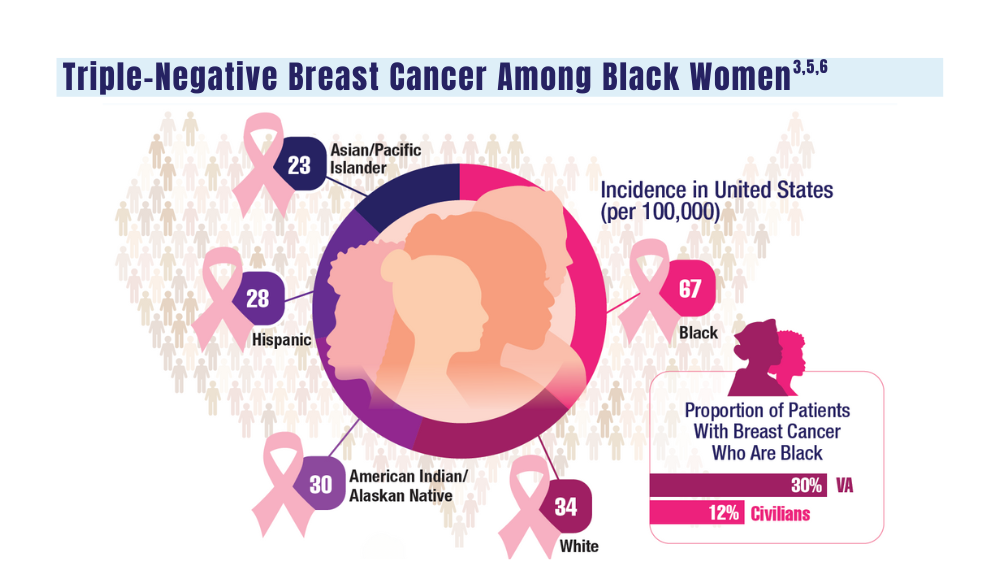
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
The annual issue of Cancer Data Trends, produced in collaboration with the Association of VA Hematology/Oncology (AVAHO), highlights the latest research in some of the top cancers impacting US veterans.
Click to view the Digital Edition.
In this issue:
Hepatocellular Carcinoma
Special care for veterans, changes in staging, and biomarkers for early diagnosis
Lung Cancer
Guideline updates and racial disparities in veterans
Multiple Myeloma
Improving survival in the VA
Colorectal Cancer
Barriers to follow-up colonoscopies after FIT testing
B-Cell Lymphomas
Findings from the VA's National TeleOncology Program and recent therapy updates
Breast Cancer
A look at the VA's Risk Assessment Pipeline and incidence among veterans vs the general population
Genitourinary Cancers
Molecular testing in prostate cancer, improving survival for metastatic RCC, and links between bladder cancer and Agent Orange exposure
Consider These Factors in an Academic Radiation Oncology Position
TOPLINE:
— and accept an offer if the practice is “great” in at least two of those areas and “good” in the third, experts say in a recent editorial.
METHODOLOGY:
- Many physicians choose to go into academic medicine because they want to stay involved in research and education while still treating patients.
- However, graduating radiation oncology residents often lack or have limited guidance on what to look for in a prospective job and how to assess their contract.
- This recent editorial provides guidance to radiation oncologists seeking academic positions. The authors advise prospective employees to evaluate three main factors — compensation, daily duties, and location — as well as provide tips for identifying red flags in each category.
TAKEAWAY:
- Compensation: Prospective faculty should assess both direct compensation, that is, salary, and indirect compensation, which typically includes retirement contributions and other perks. For direct compensation, what is the base salary? Is extra work compensated? How does the salary offer measure up to salary data reported by national agencies? Also: Don’t overlook uncompensated duties, such as time in tumor boards or in meetings, which may be time-consuming, and make sure compensation terms are clearly delineated in a contract and equitable among physicians in a specific rank.
- Daily duties: When it comes to daily life on the job, a prospective employee should consider many factors, including the cancer center’s excitement to hire you, the reputation of the faculty and leaders at the organization, employee turnover rates, diversity among faculty, and the time line of career advancement.
- Location: The location of the job encompasses the geography — such as distance from home to work, the number of practices covered, cost of living, and the area itself — as well as the atmosphere for conducting research and publishing.
- Finally, carefully review the job contract. All the key aspects of the job, including compensation and benefits, should be clearly stated in the contract to “improve communication of expectations.”
IN PRACTICE:
“A prospective faculty member can ask 100 questions, but they can’t make 100 demands; consideration of the three domains can help to focus negotiation efforts where the efforts are needed,” the authors noted.
SOURCE:
This editorial, led by Nicholas G. Zaorsky from the Department of Radiation Oncology, University Hospitals Seidman Cancer Center, Case Western Reserve School of Medicine, Cleveland, Ohio, was published online in Practical Radiation Oncology
DISCLOSURES:
The lead author declared being supported by the American Cancer Society and National Institutes of Health. He also reported having ties with many other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
— and accept an offer if the practice is “great” in at least two of those areas and “good” in the third, experts say in a recent editorial.
METHODOLOGY:
- Many physicians choose to go into academic medicine because they want to stay involved in research and education while still treating patients.
- However, graduating radiation oncology residents often lack or have limited guidance on what to look for in a prospective job and how to assess their contract.
- This recent editorial provides guidance to radiation oncologists seeking academic positions. The authors advise prospective employees to evaluate three main factors — compensation, daily duties, and location — as well as provide tips for identifying red flags in each category.
TAKEAWAY:
- Compensation: Prospective faculty should assess both direct compensation, that is, salary, and indirect compensation, which typically includes retirement contributions and other perks. For direct compensation, what is the base salary? Is extra work compensated? How does the salary offer measure up to salary data reported by national agencies? Also: Don’t overlook uncompensated duties, such as time in tumor boards or in meetings, which may be time-consuming, and make sure compensation terms are clearly delineated in a contract and equitable among physicians in a specific rank.
- Daily duties: When it comes to daily life on the job, a prospective employee should consider many factors, including the cancer center’s excitement to hire you, the reputation of the faculty and leaders at the organization, employee turnover rates, diversity among faculty, and the time line of career advancement.
- Location: The location of the job encompasses the geography — such as distance from home to work, the number of practices covered, cost of living, and the area itself — as well as the atmosphere for conducting research and publishing.
- Finally, carefully review the job contract. All the key aspects of the job, including compensation and benefits, should be clearly stated in the contract to “improve communication of expectations.”
IN PRACTICE:
“A prospective faculty member can ask 100 questions, but they can’t make 100 demands; consideration of the three domains can help to focus negotiation efforts where the efforts are needed,” the authors noted.
SOURCE:
This editorial, led by Nicholas G. Zaorsky from the Department of Radiation Oncology, University Hospitals Seidman Cancer Center, Case Western Reserve School of Medicine, Cleveland, Ohio, was published online in Practical Radiation Oncology
DISCLOSURES:
The lead author declared being supported by the American Cancer Society and National Institutes of Health. He also reported having ties with many other sources.
A version of this article appeared on Medscape.com.
TOPLINE:
— and accept an offer if the practice is “great” in at least two of those areas and “good” in the third, experts say in a recent editorial.
METHODOLOGY:
- Many physicians choose to go into academic medicine because they want to stay involved in research and education while still treating patients.
- However, graduating radiation oncology residents often lack or have limited guidance on what to look for in a prospective job and how to assess their contract.
- This recent editorial provides guidance to radiation oncologists seeking academic positions. The authors advise prospective employees to evaluate three main factors — compensation, daily duties, and location — as well as provide tips for identifying red flags in each category.
TAKEAWAY:
- Compensation: Prospective faculty should assess both direct compensation, that is, salary, and indirect compensation, which typically includes retirement contributions and other perks. For direct compensation, what is the base salary? Is extra work compensated? How does the salary offer measure up to salary data reported by national agencies? Also: Don’t overlook uncompensated duties, such as time in tumor boards or in meetings, which may be time-consuming, and make sure compensation terms are clearly delineated in a contract and equitable among physicians in a specific rank.
- Daily duties: When it comes to daily life on the job, a prospective employee should consider many factors, including the cancer center’s excitement to hire you, the reputation of the faculty and leaders at the organization, employee turnover rates, diversity among faculty, and the time line of career advancement.
- Location: The location of the job encompasses the geography — such as distance from home to work, the number of practices covered, cost of living, and the area itself — as well as the atmosphere for conducting research and publishing.
- Finally, carefully review the job contract. All the key aspects of the job, including compensation and benefits, should be clearly stated in the contract to “improve communication of expectations.”
IN PRACTICE:
“A prospective faculty member can ask 100 questions, but they can’t make 100 demands; consideration of the three domains can help to focus negotiation efforts where the efforts are needed,” the authors noted.
SOURCE:
This editorial, led by Nicholas G. Zaorsky from the Department of Radiation Oncology, University Hospitals Seidman Cancer Center, Case Western Reserve School of Medicine, Cleveland, Ohio, was published online in Practical Radiation Oncology
DISCLOSURES:
The lead author declared being supported by the American Cancer Society and National Institutes of Health. He also reported having ties with many other sources.
A version of this article appeared on Medscape.com.
Meta-analysis Identifies Unique Risk Factors of Triple-Negative Breast Cancer
Key clinical point: The risk factors for overall breast cancer (such as parity, menopausal hormone therapy use, and alcohol consumption) did not increase the risk for triple-negative breast cancer (TNBC), which had a distinct risk factor profile.
Major finding: Parity, menopausal hormone therapy use, alcohol consumption, smoking, and higher body mass index were not significantly associated with TNBC risk (all P > .05); instead, family history (odds ratio [OR] 1.55; P < .001), longer duration of oral contraceptive use (OR 1.29; P < .001), and higher breast density (OR 2.19; P < .001) were significantly associated with an increased risk for TNBC.
Study details: This meta-analysis evaluated the association between TNBC incidence and established BC risk factors using data from 33 studies.
Disclosures: This study was supported by grants from the American Cancer Society and Royal College of Surgeons in Ireland - Medical University of Bahrain (RCSI-MUB Bahrain). The authors declared no conflicts of interest.
Source: Kumar N, Ehsan S, Banerjee S, et al. The unique risk factor profile of triple negative breast cancer: A comprehensive meta-analysis. J Natl Cancer Inst. 2024 (Mar 5). Doi: 10.1093/jnci/djae056 Source
Key clinical point: The risk factors for overall breast cancer (such as parity, menopausal hormone therapy use, and alcohol consumption) did not increase the risk for triple-negative breast cancer (TNBC), which had a distinct risk factor profile.
Major finding: Parity, menopausal hormone therapy use, alcohol consumption, smoking, and higher body mass index were not significantly associated with TNBC risk (all P > .05); instead, family history (odds ratio [OR] 1.55; P < .001), longer duration of oral contraceptive use (OR 1.29; P < .001), and higher breast density (OR 2.19; P < .001) were significantly associated with an increased risk for TNBC.
Study details: This meta-analysis evaluated the association between TNBC incidence and established BC risk factors using data from 33 studies.
Disclosures: This study was supported by grants from the American Cancer Society and Royal College of Surgeons in Ireland - Medical University of Bahrain (RCSI-MUB Bahrain). The authors declared no conflicts of interest.
Source: Kumar N, Ehsan S, Banerjee S, et al. The unique risk factor profile of triple negative breast cancer: A comprehensive meta-analysis. J Natl Cancer Inst. 2024 (Mar 5). Doi: 10.1093/jnci/djae056 Source
Key clinical point: The risk factors for overall breast cancer (such as parity, menopausal hormone therapy use, and alcohol consumption) did not increase the risk for triple-negative breast cancer (TNBC), which had a distinct risk factor profile.
Major finding: Parity, menopausal hormone therapy use, alcohol consumption, smoking, and higher body mass index were not significantly associated with TNBC risk (all P > .05); instead, family history (odds ratio [OR] 1.55; P < .001), longer duration of oral contraceptive use (OR 1.29; P < .001), and higher breast density (OR 2.19; P < .001) were significantly associated with an increased risk for TNBC.
Study details: This meta-analysis evaluated the association between TNBC incidence and established BC risk factors using data from 33 studies.
Disclosures: This study was supported by grants from the American Cancer Society and Royal College of Surgeons in Ireland - Medical University of Bahrain (RCSI-MUB Bahrain). The authors declared no conflicts of interest.
Source: Kumar N, Ehsan S, Banerjee S, et al. The unique risk factor profile of triple negative breast cancer: A comprehensive meta-analysis. J Natl Cancer Inst. 2024 (Mar 5). Doi: 10.1093/jnci/djae056 Source
Pro-Vegetarian Diet May Lower Risk for Breast Cancer
Key clinical point: The pro-vegetarian dietary pattern (PDP) was associated with a significantly lower risk for breast cancer (BC) in women, particularly postmenopausal women.
Major finding: Compared with women who had low adherence to PDP (score ≤ 33), the risk for BC was significantly lower among women with moderate adherence to PDP (score 34-38; adjusted odds ratio [aOR] 0.42; P = .003) and in those with high adherence to PDP (score ≥ 39; aOR 0.49; P = .017), with outcomes being similar in the subgroup of postmenopausal women.
Study details: Findings are from a case-control study including women with BC (n = 134) and those without cancer (n = 265).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Hosseini Y, Hadi Sichani P, Moslemi E, et al. Pro-vegetarian dietary pattern and risk of breast cancer: A case-control study. Breast Cancer Res Treat. 2024 (Feb 28). doi: 10.1007/s10549-024-07243-8 Source
Key clinical point: The pro-vegetarian dietary pattern (PDP) was associated with a significantly lower risk for breast cancer (BC) in women, particularly postmenopausal women.
Major finding: Compared with women who had low adherence to PDP (score ≤ 33), the risk for BC was significantly lower among women with moderate adherence to PDP (score 34-38; adjusted odds ratio [aOR] 0.42; P = .003) and in those with high adherence to PDP (score ≥ 39; aOR 0.49; P = .017), with outcomes being similar in the subgroup of postmenopausal women.
Study details: Findings are from a case-control study including women with BC (n = 134) and those without cancer (n = 265).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Hosseini Y, Hadi Sichani P, Moslemi E, et al. Pro-vegetarian dietary pattern and risk of breast cancer: A case-control study. Breast Cancer Res Treat. 2024 (Feb 28). doi: 10.1007/s10549-024-07243-8 Source
Key clinical point: The pro-vegetarian dietary pattern (PDP) was associated with a significantly lower risk for breast cancer (BC) in women, particularly postmenopausal women.
Major finding: Compared with women who had low adherence to PDP (score ≤ 33), the risk for BC was significantly lower among women with moderate adherence to PDP (score 34-38; adjusted odds ratio [aOR] 0.42; P = .003) and in those with high adherence to PDP (score ≥ 39; aOR 0.49; P = .017), with outcomes being similar in the subgroup of postmenopausal women.
Study details: Findings are from a case-control study including women with BC (n = 134) and those without cancer (n = 265).
Disclosures: This study did not receive any funding. The authors declared no conflicts of interest.
Source: Hosseini Y, Hadi Sichani P, Moslemi E, et al. Pro-vegetarian dietary pattern and risk of breast cancer: A case-control study. Breast Cancer Res Treat. 2024 (Feb 28). doi: 10.1007/s10549-024-07243-8 Source
Real-World Study Supports Everolimus + Exemestane as HR+/HER2− BC Treatment
Key clinical point: Everolimus + exemestane demonstrated good efficacy and had a manageable safety profile in postmenopausal women with hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2−) breast cancer (BC).
Major finding: Everolimus + exemestane led to a median progression-free survival (PFS) of 6.6 months (95% CI 6.3-7.0 months). PFS was more favorable among patients with a greater vs lower body mass index (≥25 vs 20 to <25 kg/m2; P < .0001); however, the survival outcomes were worse among patients with vs without visceral metastases (hazard ratio 1.417; P < .0001). Stomatitis (42.6%) and fatigue (19.8%) were the most frequent adverse events.
Study details: Findings are from a prospective, non-interventional study including 2074 postmenopausal women with HR+/HER2− advanced BC who received everolimus + exemestane.
Disclosures: This study was funded by Novartis Deutschland GmbH, Germany. Two authors declared being employees of or holding stocks in Novartis. Some authors declared receiving honoraria or personal fees or having other ties with Novartis and various other sources. Eight authors declared no conflicts of interest.
Source: Lüftner D, Schuetz F, Schneeweiss A, et al. Efficacy and safety of everolimus plus exemestane in patients with hormone receptor-positive, HER-2-negative advanced breast cancer: Results from the open-label, multicentre, non-interventional BRAWO study. Int J Cancer. 2024 (Mar 6). doi: 10.1002/ijc.34912 Source
Key clinical point: Everolimus + exemestane demonstrated good efficacy and had a manageable safety profile in postmenopausal women with hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2−) breast cancer (BC).
Major finding: Everolimus + exemestane led to a median progression-free survival (PFS) of 6.6 months (95% CI 6.3-7.0 months). PFS was more favorable among patients with a greater vs lower body mass index (≥25 vs 20 to <25 kg/m2; P < .0001); however, the survival outcomes were worse among patients with vs without visceral metastases (hazard ratio 1.417; P < .0001). Stomatitis (42.6%) and fatigue (19.8%) were the most frequent adverse events.
Study details: Findings are from a prospective, non-interventional study including 2074 postmenopausal women with HR+/HER2− advanced BC who received everolimus + exemestane.
Disclosures: This study was funded by Novartis Deutschland GmbH, Germany. Two authors declared being employees of or holding stocks in Novartis. Some authors declared receiving honoraria or personal fees or having other ties with Novartis and various other sources. Eight authors declared no conflicts of interest.
Source: Lüftner D, Schuetz F, Schneeweiss A, et al. Efficacy and safety of everolimus plus exemestane in patients with hormone receptor-positive, HER-2-negative advanced breast cancer: Results from the open-label, multicentre, non-interventional BRAWO study. Int J Cancer. 2024 (Mar 6). doi: 10.1002/ijc.34912 Source
Key clinical point: Everolimus + exemestane demonstrated good efficacy and had a manageable safety profile in postmenopausal women with hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2−) breast cancer (BC).
Major finding: Everolimus + exemestane led to a median progression-free survival (PFS) of 6.6 months (95% CI 6.3-7.0 months). PFS was more favorable among patients with a greater vs lower body mass index (≥25 vs 20 to <25 kg/m2; P < .0001); however, the survival outcomes were worse among patients with vs without visceral metastases (hazard ratio 1.417; P < .0001). Stomatitis (42.6%) and fatigue (19.8%) were the most frequent adverse events.
Study details: Findings are from a prospective, non-interventional study including 2074 postmenopausal women with HR+/HER2− advanced BC who received everolimus + exemestane.
Disclosures: This study was funded by Novartis Deutschland GmbH, Germany. Two authors declared being employees of or holding stocks in Novartis. Some authors declared receiving honoraria or personal fees or having other ties with Novartis and various other sources. Eight authors declared no conflicts of interest.
Source: Lüftner D, Schuetz F, Schneeweiss A, et al. Efficacy and safety of everolimus plus exemestane in patients with hormone receptor-positive, HER-2-negative advanced breast cancer: Results from the open-label, multicentre, non-interventional BRAWO study. Int J Cancer. 2024 (Mar 6). doi: 10.1002/ijc.34912 Source
Axillary Lymph Node Dissection Can Be Safely Skipped in Breast Cancer Patients Undergoing Mastectomy
Key clinical point: Sentinel lymph node biopsy (SLNB), a less invasive strategy, resulted in comparable survival and regional disease control as axillary lymph node dissection (ALND) in patients with sentinel node-positive early breast cancer (BC) who underwent total mastectomy (TM).
Major finding: There were no significant differences in 5-year ipsilateral locoregional recurrence-free survival (LRRFS; P = .21), 5-year distant metastasis-free survival (P = .96), and disease-free survival (P > .05) between the SLNB-alone and ALND groups. However, receipt vs no receipt of radiation therapy improved local disease control in the SLNB group (5-year LRRFS; 100.0% vs 92.9%; P = .02).
Study details: Findings are from a retrospective study including 643 patients with early BC with 1-3 metastatic sentinel lymph nodes who underwent total mastectomy, of which 237 and 406 patients underwent SLNB alone and completion ALND, respectively.
Disclosures: The open access funding for this study was enabled and organized by Seoul National University. The authors declared no conflicts of interest.
Source: Chun JW, Kang E, Kim H-K, et al. Oncological safety of skipping axillary lymph node dissection in patients with clinical N0, sentinel node-positive breast cancer undergoing total mastectomy. Ann Surg Oncol. 2024 (Feb 17). doi: 10.1245/s10434-024-15049-7 Source
Key clinical point: Sentinel lymph node biopsy (SLNB), a less invasive strategy, resulted in comparable survival and regional disease control as axillary lymph node dissection (ALND) in patients with sentinel node-positive early breast cancer (BC) who underwent total mastectomy (TM).
Major finding: There were no significant differences in 5-year ipsilateral locoregional recurrence-free survival (LRRFS; P = .21), 5-year distant metastasis-free survival (P = .96), and disease-free survival (P > .05) between the SLNB-alone and ALND groups. However, receipt vs no receipt of radiation therapy improved local disease control in the SLNB group (5-year LRRFS; 100.0% vs 92.9%; P = .02).
Study details: Findings are from a retrospective study including 643 patients with early BC with 1-3 metastatic sentinel lymph nodes who underwent total mastectomy, of which 237 and 406 patients underwent SLNB alone and completion ALND, respectively.
Disclosures: The open access funding for this study was enabled and organized by Seoul National University. The authors declared no conflicts of interest.
Source: Chun JW, Kang E, Kim H-K, et al. Oncological safety of skipping axillary lymph node dissection in patients with clinical N0, sentinel node-positive breast cancer undergoing total mastectomy. Ann Surg Oncol. 2024 (Feb 17). doi: 10.1245/s10434-024-15049-7 Source
Key clinical point: Sentinel lymph node biopsy (SLNB), a less invasive strategy, resulted in comparable survival and regional disease control as axillary lymph node dissection (ALND) in patients with sentinel node-positive early breast cancer (BC) who underwent total mastectomy (TM).
Major finding: There were no significant differences in 5-year ipsilateral locoregional recurrence-free survival (LRRFS; P = .21), 5-year distant metastasis-free survival (P = .96), and disease-free survival (P > .05) between the SLNB-alone and ALND groups. However, receipt vs no receipt of radiation therapy improved local disease control in the SLNB group (5-year LRRFS; 100.0% vs 92.9%; P = .02).
Study details: Findings are from a retrospective study including 643 patients with early BC with 1-3 metastatic sentinel lymph nodes who underwent total mastectomy, of which 237 and 406 patients underwent SLNB alone and completion ALND, respectively.
Disclosures: The open access funding for this study was enabled and organized by Seoul National University. The authors declared no conflicts of interest.
Source: Chun JW, Kang E, Kim H-K, et al. Oncological safety of skipping axillary lymph node dissection in patients with clinical N0, sentinel node-positive breast cancer undergoing total mastectomy. Ann Surg Oncol. 2024 (Feb 17). doi: 10.1245/s10434-024-15049-7 Source