User login
Node-positive breast cancer: Internal mammary node irradiation may benefit patients with mediocentrally located tumors
Key clinical point: Including internal mammary node irradiation (IMNI) with regional node irradiation did not improve disease-free survival (DFS) significantly in the overall cohort of patients with node-positive breast cancer but benefited those with mediocentrally located tumors.
Major finding: The 7-year DFS rate was not significantly different between groups treated without vs with IMNI (81.9% vs 85.3%; hazard ratio [HR], 0.80; 95% CI, 0.57-1.14); however, it was significantly higher in patients with mediocentrally located tumor who were treated with vs without IMNI (91.8% vs 81.6%; HR, 0.42; 95% CI, 0.22-0.82).
Study details: Findings are from phase 3 KROG 08-06 study including 735 patients with histologically confirmed, node-positive breast cancer who underwent breast-conservation surgery or mastectomy and axillary dissection and were randomly assigned to receive regional nodal irradiation with or without IMNI.
Disclosures: This work was supported by the Cancer Control of the Ministry of Health, Welfare, and Family Affairs, Korea. The authors declared no conflict of interests.
Source: Kim YB et al. JAMA Oncol. 2021 Oct 25. doi: 10.1001/jamaoncol.2021.6036.
Key clinical point: Including internal mammary node irradiation (IMNI) with regional node irradiation did not improve disease-free survival (DFS) significantly in the overall cohort of patients with node-positive breast cancer but benefited those with mediocentrally located tumors.
Major finding: The 7-year DFS rate was not significantly different between groups treated without vs with IMNI (81.9% vs 85.3%; hazard ratio [HR], 0.80; 95% CI, 0.57-1.14); however, it was significantly higher in patients with mediocentrally located tumor who were treated with vs without IMNI (91.8% vs 81.6%; HR, 0.42; 95% CI, 0.22-0.82).
Study details: Findings are from phase 3 KROG 08-06 study including 735 patients with histologically confirmed, node-positive breast cancer who underwent breast-conservation surgery or mastectomy and axillary dissection and were randomly assigned to receive regional nodal irradiation with or without IMNI.
Disclosures: This work was supported by the Cancer Control of the Ministry of Health, Welfare, and Family Affairs, Korea. The authors declared no conflict of interests.
Source: Kim YB et al. JAMA Oncol. 2021 Oct 25. doi: 10.1001/jamaoncol.2021.6036.
Key clinical point: Including internal mammary node irradiation (IMNI) with regional node irradiation did not improve disease-free survival (DFS) significantly in the overall cohort of patients with node-positive breast cancer but benefited those with mediocentrally located tumors.
Major finding: The 7-year DFS rate was not significantly different between groups treated without vs with IMNI (81.9% vs 85.3%; hazard ratio [HR], 0.80; 95% CI, 0.57-1.14); however, it was significantly higher in patients with mediocentrally located tumor who were treated with vs without IMNI (91.8% vs 81.6%; HR, 0.42; 95% CI, 0.22-0.82).
Study details: Findings are from phase 3 KROG 08-06 study including 735 patients with histologically confirmed, node-positive breast cancer who underwent breast-conservation surgery or mastectomy and axillary dissection and were randomly assigned to receive regional nodal irradiation with or without IMNI.
Disclosures: This work was supported by the Cancer Control of the Ministry of Health, Welfare, and Family Affairs, Korea. The authors declared no conflict of interests.
Source: Kim YB et al. JAMA Oncol. 2021 Oct 25. doi: 10.1001/jamaoncol.2021.6036.
Impact of COVID-19 pandemic on breast cancer stage at diagnosis and management strategies
Key clinical point: COVID-19 pandemic has changed breast cancer (BC) management strategies, with the use of neoadjuvant endocrine therapy (NET) increasing significantly during the pandemic; however, no effect was observed on BC stage at diagnosis.
Major finding: The use of NET increased significantly during COVID-19 pandemic period (P = .002), particularly in patients with stage I hormone receptor-positive, human epidermal growth factor receptor 2-negative BC where the use of NET increased from 10% pre-COVID-19 to 23% during COVID-19 pandemic (P = .001). The pandemic had no effect on clinical prognostic stage (P = 0.39) and proportion of patients with clinical nodal status+ BC (P = 0.38).
Study details: This was a retrospective chart review including patients with newly diagnosed BC who presented at Mayo Clinic, Rochester during (March-August 2020; n=197) or before (March-August 2019; n=376) the COVID-19 pandemic.
Disclosures: Dr. Boughey declared receiving research funding from Lilly and was on a data and safety monitoring board for Cairns Surgical.
Source: Tonneson JE et al. Ann Surg Oncol. 2021 Nov 23. doi: 10.1245/s10434-021-11088-6.
Key clinical point: COVID-19 pandemic has changed breast cancer (BC) management strategies, with the use of neoadjuvant endocrine therapy (NET) increasing significantly during the pandemic; however, no effect was observed on BC stage at diagnosis.
Major finding: The use of NET increased significantly during COVID-19 pandemic period (P = .002), particularly in patients with stage I hormone receptor-positive, human epidermal growth factor receptor 2-negative BC where the use of NET increased from 10% pre-COVID-19 to 23% during COVID-19 pandemic (P = .001). The pandemic had no effect on clinical prognostic stage (P = 0.39) and proportion of patients with clinical nodal status+ BC (P = 0.38).
Study details: This was a retrospective chart review including patients with newly diagnosed BC who presented at Mayo Clinic, Rochester during (March-August 2020; n=197) or before (March-August 2019; n=376) the COVID-19 pandemic.
Disclosures: Dr. Boughey declared receiving research funding from Lilly and was on a data and safety monitoring board for Cairns Surgical.
Source: Tonneson JE et al. Ann Surg Oncol. 2021 Nov 23. doi: 10.1245/s10434-021-11088-6.
Key clinical point: COVID-19 pandemic has changed breast cancer (BC) management strategies, with the use of neoadjuvant endocrine therapy (NET) increasing significantly during the pandemic; however, no effect was observed on BC stage at diagnosis.
Major finding: The use of NET increased significantly during COVID-19 pandemic period (P = .002), particularly in patients with stage I hormone receptor-positive, human epidermal growth factor receptor 2-negative BC where the use of NET increased from 10% pre-COVID-19 to 23% during COVID-19 pandemic (P = .001). The pandemic had no effect on clinical prognostic stage (P = 0.39) and proportion of patients with clinical nodal status+ BC (P = 0.38).
Study details: This was a retrospective chart review including patients with newly diagnosed BC who presented at Mayo Clinic, Rochester during (March-August 2020; n=197) or before (March-August 2019; n=376) the COVID-19 pandemic.
Disclosures: Dr. Boughey declared receiving research funding from Lilly and was on a data and safety monitoring board for Cairns Surgical.
Source: Tonneson JE et al. Ann Surg Oncol. 2021 Nov 23. doi: 10.1245/s10434-021-11088-6.
Intense dose-dense epirubicin, paclitaxel, cyclophosphamide improves survival in HR+/HER2- BC
Key clinical point: Patients with hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2-) breast cancer (BC) significantly benefitted from neoadjuvant chemotherapy with intense dose-dense epirubicin, paclitaxel and cyclophosphamide (iddPEC) vs paclitaxel plus non-pegylated liposomal doxorubicin (PM) plus carboplatin ([Cb], triple-negative BC only).
Major finding: Although the 4-year invasive disease-free survival (iDFS; P log-rank = .334) and overall survival (OS, P log-rank = .637) was not significantly different between iddEPC vs PM(Cb) arms in the entire cohort, the subgroup of patients with HR+/HER-2-, BC, showed significantly improved iDFS (hazard ratio [HR], 2.11; P log-rank = .025) and OS (HR, 3.26; P log-rank = .029).with iddEPC.
Study details: Findings are from phase 3 GeparOcto trial including 961 patients with high-risk early BC, who were randomly assigned 1:1 to receive iddEPC or PM(Cb), of which 706 patients completed treatment.
Disclosures: This study was funded by Roche, Amgen, TEVA, and Vifor. The authors reported receiving research grants, personal fees, consulting fees, honoraria and/ or travel support from the above companies and other sources.
Source: Schneeweiss A et al. Eur J Cancer. 2021 Nov 17. doi: 10.1016/j.ejca.2021.10.011.
Key clinical point: Patients with hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2-) breast cancer (BC) significantly benefitted from neoadjuvant chemotherapy with intense dose-dense epirubicin, paclitaxel and cyclophosphamide (iddPEC) vs paclitaxel plus non-pegylated liposomal doxorubicin (PM) plus carboplatin ([Cb], triple-negative BC only).
Major finding: Although the 4-year invasive disease-free survival (iDFS; P log-rank = .334) and overall survival (OS, P log-rank = .637) was not significantly different between iddEPC vs PM(Cb) arms in the entire cohort, the subgroup of patients with HR+/HER-2-, BC, showed significantly improved iDFS (hazard ratio [HR], 2.11; P log-rank = .025) and OS (HR, 3.26; P log-rank = .029).with iddEPC.
Study details: Findings are from phase 3 GeparOcto trial including 961 patients with high-risk early BC, who were randomly assigned 1:1 to receive iddEPC or PM(Cb), of which 706 patients completed treatment.
Disclosures: This study was funded by Roche, Amgen, TEVA, and Vifor. The authors reported receiving research grants, personal fees, consulting fees, honoraria and/ or travel support from the above companies and other sources.
Source: Schneeweiss A et al. Eur J Cancer. 2021 Nov 17. doi: 10.1016/j.ejca.2021.10.011.
Key clinical point: Patients with hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2-) breast cancer (BC) significantly benefitted from neoadjuvant chemotherapy with intense dose-dense epirubicin, paclitaxel and cyclophosphamide (iddPEC) vs paclitaxel plus non-pegylated liposomal doxorubicin (PM) plus carboplatin ([Cb], triple-negative BC only).
Major finding: Although the 4-year invasive disease-free survival (iDFS; P log-rank = .334) and overall survival (OS, P log-rank = .637) was not significantly different between iddEPC vs PM(Cb) arms in the entire cohort, the subgroup of patients with HR+/HER-2-, BC, showed significantly improved iDFS (hazard ratio [HR], 2.11; P log-rank = .025) and OS (HR, 3.26; P log-rank = .029).with iddEPC.
Study details: Findings are from phase 3 GeparOcto trial including 961 patients with high-risk early BC, who were randomly assigned 1:1 to receive iddEPC or PM(Cb), of which 706 patients completed treatment.
Disclosures: This study was funded by Roche, Amgen, TEVA, and Vifor. The authors reported receiving research grants, personal fees, consulting fees, honoraria and/ or travel support from the above companies and other sources.
Source: Schneeweiss A et al. Eur J Cancer. 2021 Nov 17. doi: 10.1016/j.ejca.2021.10.011.
HER2-negative advanced breast cancer: LY2780301 + paclitaxel combo shows promise in phase 1b/2
Key clinical point: Preliminary evidence indicated feasibility of LY2780301, a dual inhibitor of p70 ribosomal protein S6 kinase and protein kinase B (AKT) and paclitaxel combination in patients with hormone-resistant2 (HER2)-negative advanced breast cancer (BC).
Major finding: The recommended phase 2 dose was LY2780301 500 mg once daily + weekly paclitaxel 80 mg/m2. The 6-month objective response rate for phase 2 was 63.9% (90% CI, 48.8-76.8) in the overall population and 55% (90% CI, 35.0-73.7) in phosphatidylinositol-3-kinase/AKT positive patients. The common drug-related adverse events were neuropathy, asthenia, ungual toxicity and pneumonitis.
Study details: Findings are from a prospective, multi-centred, phase 1b/2 TAKTIC trial including 48 patients with HER2-negative advanced BC with (phase 1B; n=12) or without (phase 2; n=36) previous cytotoxic treatment for advanced disease who were administered oral LY2780301 + intravenous paclitaxel.
Disclosures: This study was funded by the French National Cancer Institute, the Caritative Foundation and the Ligue Nationale Contre le Cancer. Three authors declared serving as advisory board member and/or receiving research grants and non-financial support from various pharmaceutical companies.
Source: Vicier C et al. Eur J Cancer. 2021 Nov 12. doi: 10.1016/j.ejca.2021.09.040.
Key clinical point: Preliminary evidence indicated feasibility of LY2780301, a dual inhibitor of p70 ribosomal protein S6 kinase and protein kinase B (AKT) and paclitaxel combination in patients with hormone-resistant2 (HER2)-negative advanced breast cancer (BC).
Major finding: The recommended phase 2 dose was LY2780301 500 mg once daily + weekly paclitaxel 80 mg/m2. The 6-month objective response rate for phase 2 was 63.9% (90% CI, 48.8-76.8) in the overall population and 55% (90% CI, 35.0-73.7) in phosphatidylinositol-3-kinase/AKT positive patients. The common drug-related adverse events were neuropathy, asthenia, ungual toxicity and pneumonitis.
Study details: Findings are from a prospective, multi-centred, phase 1b/2 TAKTIC trial including 48 patients with HER2-negative advanced BC with (phase 1B; n=12) or without (phase 2; n=36) previous cytotoxic treatment for advanced disease who were administered oral LY2780301 + intravenous paclitaxel.
Disclosures: This study was funded by the French National Cancer Institute, the Caritative Foundation and the Ligue Nationale Contre le Cancer. Three authors declared serving as advisory board member and/or receiving research grants and non-financial support from various pharmaceutical companies.
Source: Vicier C et al. Eur J Cancer. 2021 Nov 12. doi: 10.1016/j.ejca.2021.09.040.
Key clinical point: Preliminary evidence indicated feasibility of LY2780301, a dual inhibitor of p70 ribosomal protein S6 kinase and protein kinase B (AKT) and paclitaxel combination in patients with hormone-resistant2 (HER2)-negative advanced breast cancer (BC).
Major finding: The recommended phase 2 dose was LY2780301 500 mg once daily + weekly paclitaxel 80 mg/m2. The 6-month objective response rate for phase 2 was 63.9% (90% CI, 48.8-76.8) in the overall population and 55% (90% CI, 35.0-73.7) in phosphatidylinositol-3-kinase/AKT positive patients. The common drug-related adverse events were neuropathy, asthenia, ungual toxicity and pneumonitis.
Study details: Findings are from a prospective, multi-centred, phase 1b/2 TAKTIC trial including 48 patients with HER2-negative advanced BC with (phase 1B; n=12) or without (phase 2; n=36) previous cytotoxic treatment for advanced disease who were administered oral LY2780301 + intravenous paclitaxel.
Disclosures: This study was funded by the French National Cancer Institute, the Caritative Foundation and the Ligue Nationale Contre le Cancer. Three authors declared serving as advisory board member and/or receiving research grants and non-financial support from various pharmaceutical companies.
Source: Vicier C et al. Eur J Cancer. 2021 Nov 12. doi: 10.1016/j.ejca.2021.09.040.
HER2-negative breast cancer: Adding dalpiciclib to fulvestrant prolongs PFS in phase 3
Key clinical point: Dalpiciclib plus fulvestrant prolonged progression-free survival (PFS) compared with placebo+fulvestrant in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer who progressed during or after endocrine therapy.
Major finding: Patients receiving dalpiciclib+fulvestrant showed significantly prolonged investigator-assessed progression-free survival than those who received placebo+fulvestrant (median, 15.7 months vs 7.2 months; hazard ratio, 0.42; P < .0001). Serious adverse events were reported by 5.8% vs 6.7% of patients recieving dalpiciclib+fulvestrant vs placebo+fulvestrant.
Study details: Findings are interim results from phase 3 DAWNA-1 trial, including 361 patients with HR-positive, HER2-negative locally advanced breast cancer who progressed on endocrine therapy and were randomly assigned to dalpiciclib+fulvestrant or placebo+fulvestrant.
Disclosures: This study was funded by Jiangsu Hengrui Pharmaceuticals. The authors reported receiving research grants, advisory fees from Hengrui and other sources. Four authors declared being employees of Hengrui.
Source: Xu B et al. Nat Med. 2021 Nov 4. doi: 10.1038/s41591-021-01562-9.
Key clinical point: Dalpiciclib plus fulvestrant prolonged progression-free survival (PFS) compared with placebo+fulvestrant in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer who progressed during or after endocrine therapy.
Major finding: Patients receiving dalpiciclib+fulvestrant showed significantly prolonged investigator-assessed progression-free survival than those who received placebo+fulvestrant (median, 15.7 months vs 7.2 months; hazard ratio, 0.42; P < .0001). Serious adverse events were reported by 5.8% vs 6.7% of patients recieving dalpiciclib+fulvestrant vs placebo+fulvestrant.
Study details: Findings are interim results from phase 3 DAWNA-1 trial, including 361 patients with HR-positive, HER2-negative locally advanced breast cancer who progressed on endocrine therapy and were randomly assigned to dalpiciclib+fulvestrant or placebo+fulvestrant.
Disclosures: This study was funded by Jiangsu Hengrui Pharmaceuticals. The authors reported receiving research grants, advisory fees from Hengrui and other sources. Four authors declared being employees of Hengrui.
Source: Xu B et al. Nat Med. 2021 Nov 4. doi: 10.1038/s41591-021-01562-9.
Key clinical point: Dalpiciclib plus fulvestrant prolonged progression-free survival (PFS) compared with placebo+fulvestrant in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer who progressed during or after endocrine therapy.
Major finding: Patients receiving dalpiciclib+fulvestrant showed significantly prolonged investigator-assessed progression-free survival than those who received placebo+fulvestrant (median, 15.7 months vs 7.2 months; hazard ratio, 0.42; P < .0001). Serious adverse events were reported by 5.8% vs 6.7% of patients recieving dalpiciclib+fulvestrant vs placebo+fulvestrant.
Study details: Findings are interim results from phase 3 DAWNA-1 trial, including 361 patients with HR-positive, HER2-negative locally advanced breast cancer who progressed on endocrine therapy and were randomly assigned to dalpiciclib+fulvestrant or placebo+fulvestrant.
Disclosures: This study was funded by Jiangsu Hengrui Pharmaceuticals. The authors reported receiving research grants, advisory fees from Hengrui and other sources. Four authors declared being employees of Hengrui.
Source: Xu B et al. Nat Med. 2021 Nov 4. doi: 10.1038/s41591-021-01562-9.
Long-term ovarian suppression with GnRHa safe in premenopausal early breast cancer
Key clinical point: Final 12-year results from the PROMISE-GIM6 study reassures safety of concurrent administration of gonadotropin-releasing hormone agonist (GnRHa), triptorelin during chemotherapy in premenopausal women with early breast cancer (BC).
Major finding: The 12-year disease-free survival (65.7 % vs 69.2%; hazard ratio [HR], 1.16; P = .50), overall survival (81.2 % vs 81.3%; HR, 1.17; P = .58), and posttreatment pregnancy (9 vs 4 patients; HR, 2.14; P = .20) were not significantly different in GnRHa+chemotherapy vs chemotherapy-only groups.
Study details: PROMISE-GIM6, a phase 3 superiority trial included 281 premenopausal women with hormone receptor-positive or -negative early BC who were randomly assigned to receive GnRHa+chemotherapy or chemotherapy alone.
Disclosures: This study was funded by IRCCS Ospedale Policlinico San Martino and Associazione Italiana per la Ricerca sul Cancro and the Italian Ministry of Health. Some of the authors declared serving as a consultant and/or receiving speaker honoraria and travel accommodation from various pharmaceutical companies.
Source: Lambertini M et al. J Natl Cancer Inst. 2021 Nov 25. doi: 10.1093/jnci/djab213.
Key clinical point: Final 12-year results from the PROMISE-GIM6 study reassures safety of concurrent administration of gonadotropin-releasing hormone agonist (GnRHa), triptorelin during chemotherapy in premenopausal women with early breast cancer (BC).
Major finding: The 12-year disease-free survival (65.7 % vs 69.2%; hazard ratio [HR], 1.16; P = .50), overall survival (81.2 % vs 81.3%; HR, 1.17; P = .58), and posttreatment pregnancy (9 vs 4 patients; HR, 2.14; P = .20) were not significantly different in GnRHa+chemotherapy vs chemotherapy-only groups.
Study details: PROMISE-GIM6, a phase 3 superiority trial included 281 premenopausal women with hormone receptor-positive or -negative early BC who were randomly assigned to receive GnRHa+chemotherapy or chemotherapy alone.
Disclosures: This study was funded by IRCCS Ospedale Policlinico San Martino and Associazione Italiana per la Ricerca sul Cancro and the Italian Ministry of Health. Some of the authors declared serving as a consultant and/or receiving speaker honoraria and travel accommodation from various pharmaceutical companies.
Source: Lambertini M et al. J Natl Cancer Inst. 2021 Nov 25. doi: 10.1093/jnci/djab213.
Key clinical point: Final 12-year results from the PROMISE-GIM6 study reassures safety of concurrent administration of gonadotropin-releasing hormone agonist (GnRHa), triptorelin during chemotherapy in premenopausal women with early breast cancer (BC).
Major finding: The 12-year disease-free survival (65.7 % vs 69.2%; hazard ratio [HR], 1.16; P = .50), overall survival (81.2 % vs 81.3%; HR, 1.17; P = .58), and posttreatment pregnancy (9 vs 4 patients; HR, 2.14; P = .20) were not significantly different in GnRHa+chemotherapy vs chemotherapy-only groups.
Study details: PROMISE-GIM6, a phase 3 superiority trial included 281 premenopausal women with hormone receptor-positive or -negative early BC who were randomly assigned to receive GnRHa+chemotherapy or chemotherapy alone.
Disclosures: This study was funded by IRCCS Ospedale Policlinico San Martino and Associazione Italiana per la Ricerca sul Cancro and the Italian Ministry of Health. Some of the authors declared serving as a consultant and/or receiving speaker honoraria and travel accommodation from various pharmaceutical companies.
Source: Lambertini M et al. J Natl Cancer Inst. 2021 Nov 25. doi: 10.1093/jnci/djab213.
Chemoendocrine therapy beneficial in premenopausal women with node+ breast cancer and low recurrence score
Key clinical point: Chemoendocrine therapy vs endocrine-only therapy conferred longer invasive disease-free survival (iDFS) in premenopausal women with node-positive (node+) breast cancer (BC) and a recurrence score (RS) of ≤25 on a 21-gene assay.
Major finding: The 5-year iDFS was 93.9% in chemoendocrine group vs 89% in endocrine-only group with a significant chemotherapy benefit in premenopausal women (hazard ratio, 0.60; P = .002).
Study details: Findings are from RxPONDER, a prospective, ongoing phase 3 study, including 5,083 women with hormone receptor-positive/human epidermal growth factor receptor 2-negative BC, positive axillary lymph nodes, and RS of ≤25 who were randomly assigned to endocrine-only therapy or chemoendocrine therapy.
Disclosures: This study was supported by the National Cancer Institute, Susan G. Komen for the Cure Research Program, Hope Foundation for Cancer Research, Breast Cancer Research Foundation, and Genomic Health. The authors declared serving as a consultant, advisory board member, investigator and/or receiving grants and travel allowance from several sources.
Source: Kalinsky K et al. New Eng J Med. 2021 Dec 1. doi: 10.1056/NEJMoa2108873.
Key clinical point: Chemoendocrine therapy vs endocrine-only therapy conferred longer invasive disease-free survival (iDFS) in premenopausal women with node-positive (node+) breast cancer (BC) and a recurrence score (RS) of ≤25 on a 21-gene assay.
Major finding: The 5-year iDFS was 93.9% in chemoendocrine group vs 89% in endocrine-only group with a significant chemotherapy benefit in premenopausal women (hazard ratio, 0.60; P = .002).
Study details: Findings are from RxPONDER, a prospective, ongoing phase 3 study, including 5,083 women with hormone receptor-positive/human epidermal growth factor receptor 2-negative BC, positive axillary lymph nodes, and RS of ≤25 who were randomly assigned to endocrine-only therapy or chemoendocrine therapy.
Disclosures: This study was supported by the National Cancer Institute, Susan G. Komen for the Cure Research Program, Hope Foundation for Cancer Research, Breast Cancer Research Foundation, and Genomic Health. The authors declared serving as a consultant, advisory board member, investigator and/or receiving grants and travel allowance from several sources.
Source: Kalinsky K et al. New Eng J Med. 2021 Dec 1. doi: 10.1056/NEJMoa2108873.
Key clinical point: Chemoendocrine therapy vs endocrine-only therapy conferred longer invasive disease-free survival (iDFS) in premenopausal women with node-positive (node+) breast cancer (BC) and a recurrence score (RS) of ≤25 on a 21-gene assay.
Major finding: The 5-year iDFS was 93.9% in chemoendocrine group vs 89% in endocrine-only group with a significant chemotherapy benefit in premenopausal women (hazard ratio, 0.60; P = .002).
Study details: Findings are from RxPONDER, a prospective, ongoing phase 3 study, including 5,083 women with hormone receptor-positive/human epidermal growth factor receptor 2-negative BC, positive axillary lymph nodes, and RS of ≤25 who were randomly assigned to endocrine-only therapy or chemoendocrine therapy.
Disclosures: This study was supported by the National Cancer Institute, Susan G. Komen for the Cure Research Program, Hope Foundation for Cancer Research, Breast Cancer Research Foundation, and Genomic Health. The authors declared serving as a consultant, advisory board member, investigator and/or receiving grants and travel allowance from several sources.
Source: Kalinsky K et al. New Eng J Med. 2021 Dec 1. doi: 10.1056/NEJMoa2108873.
Postmenopausal women with early breast cancer can go chemo-free
New results from the phase 3 RxPONDER trial add to mounting evidence that most postmenopausal women with early-stage breast cancer derive no added benefits from chemotherapy and can be effectively treated with endocrine therapy alone.
The study, published in The New England Journal of Medicine, conversely shows that premenopausal women do benefit from adjuvant chemotherapy, theorized by many to largely be the result of chemotherapy-induced ovarian function suppression.
The RxPONDER trial results are in line with those from the practice-changing TAILORx trial and underscore that “postmenopausal women with 1 to 3 positive nodes and [a recurrence score] of 0 to 25 can likely safely forgo adjuvant chemotherapy without compromising invasive disease-free survival,” first author Kevin Kalinsky, MD, of the Winship Cancer Institute at Emory University, Atlanta, told this news organization. “This will save tens of thousands of women the time, expense, and potentially harmful side effects that can be associated with chemotherapy infusions.”
However, the authors note, “premenopausal women with 1-3 positive lymph nodes had a significant benefit from chemotherapy.”
The study, conducted by the Southwest Oncology Group (SWOG) Cancer Research Network, involved 5,018 women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancer with one to three positive axillary lymph nodes – a breast cancer profile that represents approximately 20% of cases in the U.S.
All women had recurrence scores on the 100-point 21-gene breast cancer assay (Oncotype Dx) under 25, which is considered the lowest risk of recurrence. Patients were randomized to treatment with endocrine therapy only (n = 2,507) or chemotherapy followed by endocrine therapy (n = 2,511).
After a median follow-up of 5.3 years, women treated with adjunctive chemotherapy plus endocrine therapy exhibited no significant improvements in invasive disease-free survival compared to those who received endocrine therapy alone.
A prespecified analysis stratifying women by menopausal status underscored those results among postmenopausal women. In this cohort, researchers reported invasive disease-free survival was 91.9% in the endocrine-only group and 91.3% in the chemotherapy group (HR, 1.02; P = .89), indicating no benefit of the adjunctive chemotherapy.
However, among premenopausal women, the invasive disease-free survival rate was significantly higher with the addition of chemotherapy – 89.0% with endocrine-only therapy and 93.9% with both therapies (HR, 0.60; P = .002). Increases in distant relapse-free survival observed in the dual-therapy group similarly favored adding chemotherapy (HR, 0.58; P = .009).
Even when the authors further stratified the women into recurrence scores of 0 to 13 or 14 to 25, the results remained consistent. Postmenopausal women in each of the recurrence score groups continued to show no difference in invasive disease recurrence, new primary cancer, or death from chemotherapy (HR, 1.01 for each score group). Conversely, premenopausal women showed significant improvements in those outcomes when chemotherapy was added to endocrine therapy.
To what degree were the effects observed in premenopausal women the result of chemotherapy-induced ovarian suppression?
“I think it’s fair to say it’s the most interesting question right now in early-stage breast cancer for ER-positive tumors,” Harold Burstein, MD, of the Dana-Farber Cancer Institute and Harvard Medical School, Boston, said during a debate at the recent San Antonio Breast Cancer Symposium.
According to Sibylle Loibl, MD, PhD, when it comes to the use of chemotherapy, “age matters.”
“I strongly believe the biology of tumors is different in younger women with HR-positive/HER2-negative breast cancer,” Dr. Loibl, an associate professor at the University of Frankfurt, said during the debate. “It’s a different disease and the effects of chemotherapy are different.”
In young women, chemotherapy has “a direct cytotoxic effect, which cannot be neglected, and an endocrine effect on ovarian function suppression,” Dr. Loibl added. “I think both are needed in young premenopausal patients.”
According to the RxPONDER authors, “whether a chemotherapy benefit in premenopausal women is due to both direct cytocidal effects and treatment-induced menopause remains unclear,” but they noted that “it is possible that the contribution of these mechanisms may vary according to age.”
Further complicating matters, Dr. Loibl added, is that age appears to be poorly represented in genetic diagnostic tools.
“I think the gene expression profiles we are currently using as standard diagnostic tools do not capture the right biology for our premenopausal patients,” she said. “We have to keep in mind that these tests were designed and validated in postmenopausal patients and were only retrospectively used in premenopausal patients.”
The study was funded by the National Cancer Institute and others. Dr. Loibl has received honoraria from Prime and Chugai and numerous institutional research grants.
A version of this article first appeared on Medscape.com.
New results from the phase 3 RxPONDER trial add to mounting evidence that most postmenopausal women with early-stage breast cancer derive no added benefits from chemotherapy and can be effectively treated with endocrine therapy alone.
The study, published in The New England Journal of Medicine, conversely shows that premenopausal women do benefit from adjuvant chemotherapy, theorized by many to largely be the result of chemotherapy-induced ovarian function suppression.
The RxPONDER trial results are in line with those from the practice-changing TAILORx trial and underscore that “postmenopausal women with 1 to 3 positive nodes and [a recurrence score] of 0 to 25 can likely safely forgo adjuvant chemotherapy without compromising invasive disease-free survival,” first author Kevin Kalinsky, MD, of the Winship Cancer Institute at Emory University, Atlanta, told this news organization. “This will save tens of thousands of women the time, expense, and potentially harmful side effects that can be associated with chemotherapy infusions.”
However, the authors note, “premenopausal women with 1-3 positive lymph nodes had a significant benefit from chemotherapy.”
The study, conducted by the Southwest Oncology Group (SWOG) Cancer Research Network, involved 5,018 women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancer with one to three positive axillary lymph nodes – a breast cancer profile that represents approximately 20% of cases in the U.S.
All women had recurrence scores on the 100-point 21-gene breast cancer assay (Oncotype Dx) under 25, which is considered the lowest risk of recurrence. Patients were randomized to treatment with endocrine therapy only (n = 2,507) or chemotherapy followed by endocrine therapy (n = 2,511).
After a median follow-up of 5.3 years, women treated with adjunctive chemotherapy plus endocrine therapy exhibited no significant improvements in invasive disease-free survival compared to those who received endocrine therapy alone.
A prespecified analysis stratifying women by menopausal status underscored those results among postmenopausal women. In this cohort, researchers reported invasive disease-free survival was 91.9% in the endocrine-only group and 91.3% in the chemotherapy group (HR, 1.02; P = .89), indicating no benefit of the adjunctive chemotherapy.
However, among premenopausal women, the invasive disease-free survival rate was significantly higher with the addition of chemotherapy – 89.0% with endocrine-only therapy and 93.9% with both therapies (HR, 0.60; P = .002). Increases in distant relapse-free survival observed in the dual-therapy group similarly favored adding chemotherapy (HR, 0.58; P = .009).
Even when the authors further stratified the women into recurrence scores of 0 to 13 or 14 to 25, the results remained consistent. Postmenopausal women in each of the recurrence score groups continued to show no difference in invasive disease recurrence, new primary cancer, or death from chemotherapy (HR, 1.01 for each score group). Conversely, premenopausal women showed significant improvements in those outcomes when chemotherapy was added to endocrine therapy.
To what degree were the effects observed in premenopausal women the result of chemotherapy-induced ovarian suppression?
“I think it’s fair to say it’s the most interesting question right now in early-stage breast cancer for ER-positive tumors,” Harold Burstein, MD, of the Dana-Farber Cancer Institute and Harvard Medical School, Boston, said during a debate at the recent San Antonio Breast Cancer Symposium.
According to Sibylle Loibl, MD, PhD, when it comes to the use of chemotherapy, “age matters.”
“I strongly believe the biology of tumors is different in younger women with HR-positive/HER2-negative breast cancer,” Dr. Loibl, an associate professor at the University of Frankfurt, said during the debate. “It’s a different disease and the effects of chemotherapy are different.”
In young women, chemotherapy has “a direct cytotoxic effect, which cannot be neglected, and an endocrine effect on ovarian function suppression,” Dr. Loibl added. “I think both are needed in young premenopausal patients.”
According to the RxPONDER authors, “whether a chemotherapy benefit in premenopausal women is due to both direct cytocidal effects and treatment-induced menopause remains unclear,” but they noted that “it is possible that the contribution of these mechanisms may vary according to age.”
Further complicating matters, Dr. Loibl added, is that age appears to be poorly represented in genetic diagnostic tools.
“I think the gene expression profiles we are currently using as standard diagnostic tools do not capture the right biology for our premenopausal patients,” she said. “We have to keep in mind that these tests were designed and validated in postmenopausal patients and were only retrospectively used in premenopausal patients.”
The study was funded by the National Cancer Institute and others. Dr. Loibl has received honoraria from Prime and Chugai and numerous institutional research grants.
A version of this article first appeared on Medscape.com.
New results from the phase 3 RxPONDER trial add to mounting evidence that most postmenopausal women with early-stage breast cancer derive no added benefits from chemotherapy and can be effectively treated with endocrine therapy alone.
The study, published in The New England Journal of Medicine, conversely shows that premenopausal women do benefit from adjuvant chemotherapy, theorized by many to largely be the result of chemotherapy-induced ovarian function suppression.
The RxPONDER trial results are in line with those from the practice-changing TAILORx trial and underscore that “postmenopausal women with 1 to 3 positive nodes and [a recurrence score] of 0 to 25 can likely safely forgo adjuvant chemotherapy without compromising invasive disease-free survival,” first author Kevin Kalinsky, MD, of the Winship Cancer Institute at Emory University, Atlanta, told this news organization. “This will save tens of thousands of women the time, expense, and potentially harmful side effects that can be associated with chemotherapy infusions.”
However, the authors note, “premenopausal women with 1-3 positive lymph nodes had a significant benefit from chemotherapy.”
The study, conducted by the Southwest Oncology Group (SWOG) Cancer Research Network, involved 5,018 women with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancer with one to three positive axillary lymph nodes – a breast cancer profile that represents approximately 20% of cases in the U.S.
All women had recurrence scores on the 100-point 21-gene breast cancer assay (Oncotype Dx) under 25, which is considered the lowest risk of recurrence. Patients were randomized to treatment with endocrine therapy only (n = 2,507) or chemotherapy followed by endocrine therapy (n = 2,511).
After a median follow-up of 5.3 years, women treated with adjunctive chemotherapy plus endocrine therapy exhibited no significant improvements in invasive disease-free survival compared to those who received endocrine therapy alone.
A prespecified analysis stratifying women by menopausal status underscored those results among postmenopausal women. In this cohort, researchers reported invasive disease-free survival was 91.9% in the endocrine-only group and 91.3% in the chemotherapy group (HR, 1.02; P = .89), indicating no benefit of the adjunctive chemotherapy.
However, among premenopausal women, the invasive disease-free survival rate was significantly higher with the addition of chemotherapy – 89.0% with endocrine-only therapy and 93.9% with both therapies (HR, 0.60; P = .002). Increases in distant relapse-free survival observed in the dual-therapy group similarly favored adding chemotherapy (HR, 0.58; P = .009).
Even when the authors further stratified the women into recurrence scores of 0 to 13 or 14 to 25, the results remained consistent. Postmenopausal women in each of the recurrence score groups continued to show no difference in invasive disease recurrence, new primary cancer, or death from chemotherapy (HR, 1.01 for each score group). Conversely, premenopausal women showed significant improvements in those outcomes when chemotherapy was added to endocrine therapy.
To what degree were the effects observed in premenopausal women the result of chemotherapy-induced ovarian suppression?
“I think it’s fair to say it’s the most interesting question right now in early-stage breast cancer for ER-positive tumors,” Harold Burstein, MD, of the Dana-Farber Cancer Institute and Harvard Medical School, Boston, said during a debate at the recent San Antonio Breast Cancer Symposium.
According to Sibylle Loibl, MD, PhD, when it comes to the use of chemotherapy, “age matters.”
“I strongly believe the biology of tumors is different in younger women with HR-positive/HER2-negative breast cancer,” Dr. Loibl, an associate professor at the University of Frankfurt, said during the debate. “It’s a different disease and the effects of chemotherapy are different.”
In young women, chemotherapy has “a direct cytotoxic effect, which cannot be neglected, and an endocrine effect on ovarian function suppression,” Dr. Loibl added. “I think both are needed in young premenopausal patients.”
According to the RxPONDER authors, “whether a chemotherapy benefit in premenopausal women is due to both direct cytocidal effects and treatment-induced menopause remains unclear,” but they noted that “it is possible that the contribution of these mechanisms may vary according to age.”
Further complicating matters, Dr. Loibl added, is that age appears to be poorly represented in genetic diagnostic tools.
“I think the gene expression profiles we are currently using as standard diagnostic tools do not capture the right biology for our premenopausal patients,” she said. “We have to keep in mind that these tests were designed and validated in postmenopausal patients and were only retrospectively used in premenopausal patients.”
The study was funded by the National Cancer Institute and others. Dr. Loibl has received honoraria from Prime and Chugai and numerous institutional research grants.
A version of this article first appeared on Medscape.com.
Cardiovascular effects of breast cancer treatment vary based on weight, menopausal status

For example, certain chemotherapy drugs may confer higher risk in breast cancer survivors of normal weight, whereas they may lower stroke risk in those who are obese, according to Heather Greenlee, ND, PhD, a public health researcher and naturopathic physician with the Fred Hutchinson Cancer Research Center in Seattle.
In postmenopausal women with breast cancer, aromatase inhibitors may increase cardiovascular risk, while tamoxifen appears to reduce the risk of incident dyslipidemia, she said.
The findings are from separate analyses of data from studies presented during a poster discussion session at the symposium.
Breast cancer treatment and cardiovascular effects: The role of weight
In one analysis, Dr. Greenlee and colleagues examined outcomes in 13,582 breast cancer survivors with a median age of 60 years and median follow-up of 7 years to assess whether cardiovascular disease (CVD) risk associated with specific breast cancer therapies varies by body mass index (BMI) category at diagnosis.
Many routinely used breast cancer therapies are cardiotoxic, and being overweight or obese are known risk factors for CVD, but few studies have assessed whether BMI modifies the effect of these treatment on cardiovascular risk, Dr. Greenlee explained.
After adjusting for baseline demographic and health-related factors, and other breast cancer treatment, they found that:
- Ischemic heart disease risk was higher among normal-weight women who received anthracyclines, compared with those who did not (hazard ratio, 4.2). No other risk associations were observed for other breast cancer therapies and BMI groups.
- Heart failure/cardiomyopathy risk was higher among women with normal weight who received anthracyclines, cyclophosphamides, or left-sided radiation, compared with those who did not (HRs, 5.24, 3.27, and 2.05, respectively), and among overweight women who received anthracyclines, compared with those who did not (HR, 2.18). No risk associations were observed for women who received trastuzumab, taxanes, endocrine therapy, or radiation on any side, and no risk associations were observed for women who were obese.
- Stroke risk was higher in normal-weight women who received taxanes, cyclophosphamides, or left-sided radiation versus those who did not (HRs, 2.14, 2.35, and 1.31, respectively), and stroke risk was lower in obese women who received anthracyclines, taxanes, or cyclophosphamide, compared with those who did not (HRs, 0.32, 0.41, and 0.29, respectively). No risk associations were observed for trastuzumab, endocrine therapy, or radiation on any side, and no risk associations were observed for women who were overweight.
The lack of associations noted between treatments and heart failure risk among obese patients could be caused by the “obesity paradox” observed in prior obese populations, the investigators noted, adding that additional analyses are planned to “examine whether different dosage and duration of breast cancer therapy exposures across the BMI groups contributed to these risk associations.”
Breast cancer treatment and cardiometabolic effects: The role of menopausal status
In a separate analysis, Dr. Greenlee and colleagues looked at the association between endocrine therapies and cardiometabolic risk based on menopausal status.
Endocrine therapy is associated with CVD in breast cancer survivors and may be associated with developing cardiometabolic risk factors like diabetes, dyslipidemia, and hypertension, they noted, explaining that tamoxifen has mixed estrogenic and antiestrogenic activity, while aromatase inhibitors deplete endogenous estrogen.
Since most studies have compared tamoxifen with aromatase inhibitor use, it has been a challenge challenging to discern the effects of each, Dr. Greenlee said.
She and her colleagues reviewed records for 14,942 breast cancer survivors who were diagnosed between 2005 and 2013. The patients had a mean age of 61 years at baseline, and 24.9% were premenopausal at the time of diagnosis. Of the premenopausal women, 27.3% used tamoxifen, 19.2% used aromatase inhibitors, and 53.5% did not use endocrine therapy, and of the postmenopausal women, 6.6% used tamoxifen, 47.7% used aromatase inhibitors, and 45.7% did not use endocrine therapy.
After adjusting for baseline demographics and health factors, the investigators found that:
- The use of tamoxifen or aromatase inhibitors was not associated with a risk of developing diabetes, dyslipidemia, or hypertension in premenopausal women, or with a risk of developing diabetes or hypertension in postmenopausal women.
- The risk of dyslipidemia was higher in postmenopausal aromatase inhibitor users, and lower in postmenopausal tamoxifen users, compared with postmenopausal non-users of endocrine therapy (HRs, 1.15 and 0.75, respectively).
The lack of associations between endocrine therapy and CVD risk in premenopausal women may be from low power, Dr. Greenlee said, noting that analyses in larger sample sizes are needed.
She and her colleagues plan to conduct further analyses looking at treatment dosage and duration, and comparing steroidal versus nonsteroidal aromatase inhibitors.
Future studies should examine the implications of these associations on long-term CVD and how best to manage lipid profiles in postmenopausal breast cancer survivors who have a history of endocrine therapy treatment, they concluded.
This research was funded by grants from the National Cancer Institute.
For example, certain chemotherapy drugs may confer higher risk in breast cancer survivors of normal weight, whereas they may lower stroke risk in those who are obese, according to Heather Greenlee, ND, PhD, a public health researcher and naturopathic physician with the Fred Hutchinson Cancer Research Center in Seattle.
In postmenopausal women with breast cancer, aromatase inhibitors may increase cardiovascular risk, while tamoxifen appears to reduce the risk of incident dyslipidemia, she said.
The findings are from separate analyses of data from studies presented during a poster discussion session at the symposium.
Breast cancer treatment and cardiovascular effects: The role of weight
In one analysis, Dr. Greenlee and colleagues examined outcomes in 13,582 breast cancer survivors with a median age of 60 years and median follow-up of 7 years to assess whether cardiovascular disease (CVD) risk associated with specific breast cancer therapies varies by body mass index (BMI) category at diagnosis.
Many routinely used breast cancer therapies are cardiotoxic, and being overweight or obese are known risk factors for CVD, but few studies have assessed whether BMI modifies the effect of these treatment on cardiovascular risk, Dr. Greenlee explained.
After adjusting for baseline demographic and health-related factors, and other breast cancer treatment, they found that:
- Ischemic heart disease risk was higher among normal-weight women who received anthracyclines, compared with those who did not (hazard ratio, 4.2). No other risk associations were observed for other breast cancer therapies and BMI groups.
- Heart failure/cardiomyopathy risk was higher among women with normal weight who received anthracyclines, cyclophosphamides, or left-sided radiation, compared with those who did not (HRs, 5.24, 3.27, and 2.05, respectively), and among overweight women who received anthracyclines, compared with those who did not (HR, 2.18). No risk associations were observed for women who received trastuzumab, taxanes, endocrine therapy, or radiation on any side, and no risk associations were observed for women who were obese.
- Stroke risk was higher in normal-weight women who received taxanes, cyclophosphamides, or left-sided radiation versus those who did not (HRs, 2.14, 2.35, and 1.31, respectively), and stroke risk was lower in obese women who received anthracyclines, taxanes, or cyclophosphamide, compared with those who did not (HRs, 0.32, 0.41, and 0.29, respectively). No risk associations were observed for trastuzumab, endocrine therapy, or radiation on any side, and no risk associations were observed for women who were overweight.
The lack of associations noted between treatments and heart failure risk among obese patients could be caused by the “obesity paradox” observed in prior obese populations, the investigators noted, adding that additional analyses are planned to “examine whether different dosage and duration of breast cancer therapy exposures across the BMI groups contributed to these risk associations.”
Breast cancer treatment and cardiometabolic effects: The role of menopausal status
In a separate analysis, Dr. Greenlee and colleagues looked at the association between endocrine therapies and cardiometabolic risk based on menopausal status.
Endocrine therapy is associated with CVD in breast cancer survivors and may be associated with developing cardiometabolic risk factors like diabetes, dyslipidemia, and hypertension, they noted, explaining that tamoxifen has mixed estrogenic and antiestrogenic activity, while aromatase inhibitors deplete endogenous estrogen.
Since most studies have compared tamoxifen with aromatase inhibitor use, it has been a challenge challenging to discern the effects of each, Dr. Greenlee said.
She and her colleagues reviewed records for 14,942 breast cancer survivors who were diagnosed between 2005 and 2013. The patients had a mean age of 61 years at baseline, and 24.9% were premenopausal at the time of diagnosis. Of the premenopausal women, 27.3% used tamoxifen, 19.2% used aromatase inhibitors, and 53.5% did not use endocrine therapy, and of the postmenopausal women, 6.6% used tamoxifen, 47.7% used aromatase inhibitors, and 45.7% did not use endocrine therapy.
After adjusting for baseline demographics and health factors, the investigators found that:
- The use of tamoxifen or aromatase inhibitors was not associated with a risk of developing diabetes, dyslipidemia, or hypertension in premenopausal women, or with a risk of developing diabetes or hypertension in postmenopausal women.
- The risk of dyslipidemia was higher in postmenopausal aromatase inhibitor users, and lower in postmenopausal tamoxifen users, compared with postmenopausal non-users of endocrine therapy (HRs, 1.15 and 0.75, respectively).
The lack of associations between endocrine therapy and CVD risk in premenopausal women may be from low power, Dr. Greenlee said, noting that analyses in larger sample sizes are needed.
She and her colleagues plan to conduct further analyses looking at treatment dosage and duration, and comparing steroidal versus nonsteroidal aromatase inhibitors.
Future studies should examine the implications of these associations on long-term CVD and how best to manage lipid profiles in postmenopausal breast cancer survivors who have a history of endocrine therapy treatment, they concluded.
This research was funded by grants from the National Cancer Institute.
For example, certain chemotherapy drugs may confer higher risk in breast cancer survivors of normal weight, whereas they may lower stroke risk in those who are obese, according to Heather Greenlee, ND, PhD, a public health researcher and naturopathic physician with the Fred Hutchinson Cancer Research Center in Seattle.
In postmenopausal women with breast cancer, aromatase inhibitors may increase cardiovascular risk, while tamoxifen appears to reduce the risk of incident dyslipidemia, she said.
The findings are from separate analyses of data from studies presented during a poster discussion session at the symposium.
Breast cancer treatment and cardiovascular effects: The role of weight
In one analysis, Dr. Greenlee and colleagues examined outcomes in 13,582 breast cancer survivors with a median age of 60 years and median follow-up of 7 years to assess whether cardiovascular disease (CVD) risk associated with specific breast cancer therapies varies by body mass index (BMI) category at diagnosis.
Many routinely used breast cancer therapies are cardiotoxic, and being overweight or obese are known risk factors for CVD, but few studies have assessed whether BMI modifies the effect of these treatment on cardiovascular risk, Dr. Greenlee explained.
After adjusting for baseline demographic and health-related factors, and other breast cancer treatment, they found that:
- Ischemic heart disease risk was higher among normal-weight women who received anthracyclines, compared with those who did not (hazard ratio, 4.2). No other risk associations were observed for other breast cancer therapies and BMI groups.
- Heart failure/cardiomyopathy risk was higher among women with normal weight who received anthracyclines, cyclophosphamides, or left-sided radiation, compared with those who did not (HRs, 5.24, 3.27, and 2.05, respectively), and among overweight women who received anthracyclines, compared with those who did not (HR, 2.18). No risk associations were observed for women who received trastuzumab, taxanes, endocrine therapy, or radiation on any side, and no risk associations were observed for women who were obese.
- Stroke risk was higher in normal-weight women who received taxanes, cyclophosphamides, or left-sided radiation versus those who did not (HRs, 2.14, 2.35, and 1.31, respectively), and stroke risk was lower in obese women who received anthracyclines, taxanes, or cyclophosphamide, compared with those who did not (HRs, 0.32, 0.41, and 0.29, respectively). No risk associations were observed for trastuzumab, endocrine therapy, or radiation on any side, and no risk associations were observed for women who were overweight.
The lack of associations noted between treatments and heart failure risk among obese patients could be caused by the “obesity paradox” observed in prior obese populations, the investigators noted, adding that additional analyses are planned to “examine whether different dosage and duration of breast cancer therapy exposures across the BMI groups contributed to these risk associations.”
Breast cancer treatment and cardiometabolic effects: The role of menopausal status
In a separate analysis, Dr. Greenlee and colleagues looked at the association between endocrine therapies and cardiometabolic risk based on menopausal status.
Endocrine therapy is associated with CVD in breast cancer survivors and may be associated with developing cardiometabolic risk factors like diabetes, dyslipidemia, and hypertension, they noted, explaining that tamoxifen has mixed estrogenic and antiestrogenic activity, while aromatase inhibitors deplete endogenous estrogen.
Since most studies have compared tamoxifen with aromatase inhibitor use, it has been a challenge challenging to discern the effects of each, Dr. Greenlee said.
She and her colleagues reviewed records for 14,942 breast cancer survivors who were diagnosed between 2005 and 2013. The patients had a mean age of 61 years at baseline, and 24.9% were premenopausal at the time of diagnosis. Of the premenopausal women, 27.3% used tamoxifen, 19.2% used aromatase inhibitors, and 53.5% did not use endocrine therapy, and of the postmenopausal women, 6.6% used tamoxifen, 47.7% used aromatase inhibitors, and 45.7% did not use endocrine therapy.
After adjusting for baseline demographics and health factors, the investigators found that:
- The use of tamoxifen or aromatase inhibitors was not associated with a risk of developing diabetes, dyslipidemia, or hypertension in premenopausal women, or with a risk of developing diabetes or hypertension in postmenopausal women.
- The risk of dyslipidemia was higher in postmenopausal aromatase inhibitor users, and lower in postmenopausal tamoxifen users, compared with postmenopausal non-users of endocrine therapy (HRs, 1.15 and 0.75, respectively).
The lack of associations between endocrine therapy and CVD risk in premenopausal women may be from low power, Dr. Greenlee said, noting that analyses in larger sample sizes are needed.
She and her colleagues plan to conduct further analyses looking at treatment dosage and duration, and comparing steroidal versus nonsteroidal aromatase inhibitors.
Future studies should examine the implications of these associations on long-term CVD and how best to manage lipid profiles in postmenopausal breast cancer survivors who have a history of endocrine therapy treatment, they concluded.
This research was funded by grants from the National Cancer Institute.
FROM SABCS 2021
Average-risk women with dense breasts—What breast screening is appropriate?
Text copyright DenseBreast-info.org.
Answer
A. For women with extremely dense breasts who are not otherwise at increased risk for breast cancer, screening magnetic resonance imaging (MRI) is preferred, plus her mammogram or tomosynthesis. If MRI is not an option, consider ultrasonography or contrast-enhanced mammography.
The same screening considerations apply to women with heterogeneously dense breasts; however, there is limited capacity for MRI or even ultrasound screening at many facilities. Research supports MRI in dense breasts, and abbreviated, lower-cost protocols have been validated that address some of the barriers to MRI.1 Although not yet widely available, abbreviated MRI will likely have a greater role in screening women with dense breasts who are not high risk. It is important to note that preauthorization from insurance may be required for screening MRI, and in most US states, deductibles and copays apply.
The exam
Contrast-enhanced MRI requires IV injection of gadolinium-based contrast to look at the anatomy and blood flow patterns of the breast tissue. The patient lies face down with the breasts placed in two rectangular openings, or “coils.” The exam takes place inside the tunnel of the scanner, with the head facing out.After initial images are obtained, the contrast agent is injected into a vein in the arm, and additional images are taken, which will show areas of enhancement. The exam takes about 20 to 40 minutes. An “abbreviated” MRI can be performed for screening in some centers, which uses fewer sequences and takes about 10 minutes.
Benefits
At least 40% of cancers are missed on mammography in women with dense breasts.2 MRI is the most widely studied technique using a contrast agent, and it produces the highest additional cancer detection of all the supplemental technologies to date, yielding, in the first year, 10-16 additional cancers per 1,000 women screened after mammography/tomosynthesis (reviewed in Berg et al.3). The cancer-detection benefit is seen across all breast density categories, even among average-risk women.4 There is no ionizing radiation, and it has been shown to reduce the rate of interval cancers (those detected due to symptoms after a negative screening mammogram), as well as the rate of late-stage disease. Axillary lymph nodes can be examined at the same screening exam.
While tomosynthesis improves cancer detection in women with fatty breasts, scattered fibroglandular breast tissue, and heterogeneously dense breasts, it does not significantly improve cancer detection in women with extremely dense breasts.5,6 Current American Cancer Society and National Comprehensive Cancer Network guidelines recommend annual screening MRI for women at high risk for breast cancer (regardless of breast density); however, increasingly, research supports the effectiveness of MRI in women with dense breasts who are otherwise considered average risk. A large randomized controlled trial in the Netherlands compared outcomes in women with extremely dense breasts invited to have screening MRI after negative mammography to those assigned to continue receiving screening mammography only. The incremental cancer detection rate was 16.5 per 1,000 (79/4,783) women screened with MRI in the first round7 and 6 per 1,000 women screened in the second round 2 years later.8 The interval cancer rate was 0.8 per 1,000 (4/4,783) women screened with MRI, compared with 4.9 per 1,000 (16/3,278) women who declined MRI and received mammography only.7
Screening ultrasound will show up to 3 additional cancers per 1,000 women screened after mammography/tomosynthesis (reviewed in Vourtsis and Berg9 and Berg and Vourtsis10), far lower than the added cancer-detection rate of MRI. Consider screening ultrasound for women who cannot tolerate or access screening MRI.11 Contrast-enhanced mammography (CEM) uses iodinated contrast (as in computed tomography). CEM is not widely available but appears to show cancer-detection similar to MRI. For further discussion, see Berg et al’s 2021 review.3
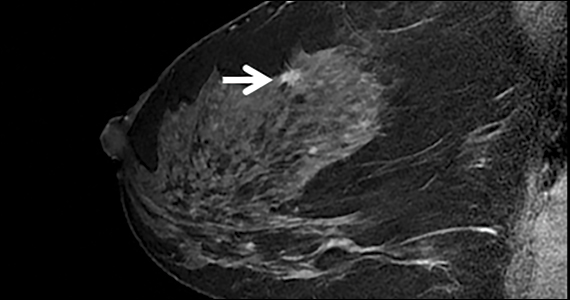
The FIGURE shows an example of an invasive cancer depicted on contrast-enhanced MRI in a 53-year-old woman with dense breasts and a family history of breast cancer that was not visible on tomosynthesis, even in retrospect, due to masking by dense tissue.

Considerations
Breast MRI increases callbacks even after mammography and ultrasound; however, such false alarms are reduced in subsequent screening rounds. MRI cannot be performed in women who have certain metal implants— some pacemakers or spinal fixation rods—and is not recommended for pregnant women. Claustrophobia may be an issue for some women. MRI is expensive and requires IV contrast. Gadolinium is known to accumulate in the brain, although the long-term effects of this are unknown and no harm has been shown.●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
- Comstock CE, Gatsonis C, Newstead GM, et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening. JAMA. 2020;323:746-756. doi: 10.1001 /jama.2020.0572
- Kerlikowske K, Zhu W, Tosteson AN, et al. Identifying women with dense breasts at high risk for interval cancer: a cohort study. Ann Intern Med. 2015;162:673-681. doi: 10.7326/M14-1465.
- Berg WA, Rafferty EA, Friedewald SM, Hruska CB, Rahbar H. Screening Algorithms in Dense Breasts: AJR Expert Panel Narrative Review. AJR Am J Roentgenol. 2021;216:275-294. doi: 10.2214/AJR.20.24436.
- Kuhl CK, Strobel K, Bieling H, et al. Supplemental breast MR imaging screening of women with average risk of breast cancer. Radiology. 2017;283:361-370. doi: 10.1148/radiol.2016161444.
- Rafferty EA, Durand MA, Conant EF, et al. Breast cancer screening using tomosynthesis and digital mammography in dense and nondense breasts. JAMA. 2016;315:1784-1786. doi: 10.1001/jama.2016.1708.
- Osteras BH, Martinsen ACT, Gullien R, et al. Digital mammography versus breast tomosynthesis: impact of breast density on diagnostic performance in population-based screening. Radiology. 2019;293:60-68. doi: 10.1148 /radiol.2019190425.
- Bakker MF, de Lange SV, Pijnappel RM, et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102. doi: 10.1056/NEJMoa1903986.
- Veenhuizen SGA, de Lange SV, Bakker MF, et al. Supplemental breast MRI for women with extremely dense breasts: results of the second screening round of the DENSE trial. Radiology. 2021;299:278-286. doi: 10.1148/radiol.2021203633.
- Vourtsis A, Berg WA. Breast density implications and supplemental screening. Eur Radiol. 2019;29:1762-1777. doi: 10.1007/s00330-018-5668-8.
- Berg WA, Vourtsis A. Screening ultrasound using handheld or automated technique in women with dense breasts. J Breast Imaging. 2019;1:283-296.
- National Comprehensive Cancer Network. Breast Cancer Screening and Diagnosis (Version 1.2021). https://www.nccn. org/professionals/physician_gls/pdf/breast-screening.pdf. Accessed November 18, 2021.
Text copyright DenseBreast-info.org.
Answer
A. For women with extremely dense breasts who are not otherwise at increased risk for breast cancer, screening magnetic resonance imaging (MRI) is preferred, plus her mammogram or tomosynthesis. If MRI is not an option, consider ultrasonography or contrast-enhanced mammography.
The same screening considerations apply to women with heterogeneously dense breasts; however, there is limited capacity for MRI or even ultrasound screening at many facilities. Research supports MRI in dense breasts, and abbreviated, lower-cost protocols have been validated that address some of the barriers to MRI.1 Although not yet widely available, abbreviated MRI will likely have a greater role in screening women with dense breasts who are not high risk. It is important to note that preauthorization from insurance may be required for screening MRI, and in most US states, deductibles and copays apply.
The exam
Contrast-enhanced MRI requires IV injection of gadolinium-based contrast to look at the anatomy and blood flow patterns of the breast tissue. The patient lies face down with the breasts placed in two rectangular openings, or “coils.” The exam takes place inside the tunnel of the scanner, with the head facing out.After initial images are obtained, the contrast agent is injected into a vein in the arm, and additional images are taken, which will show areas of enhancement. The exam takes about 20 to 40 minutes. An “abbreviated” MRI can be performed for screening in some centers, which uses fewer sequences and takes about 10 minutes.
Benefits
At least 40% of cancers are missed on mammography in women with dense breasts.2 MRI is the most widely studied technique using a contrast agent, and it produces the highest additional cancer detection of all the supplemental technologies to date, yielding, in the first year, 10-16 additional cancers per 1,000 women screened after mammography/tomosynthesis (reviewed in Berg et al.3). The cancer-detection benefit is seen across all breast density categories, even among average-risk women.4 There is no ionizing radiation, and it has been shown to reduce the rate of interval cancers (those detected due to symptoms after a negative screening mammogram), as well as the rate of late-stage disease. Axillary lymph nodes can be examined at the same screening exam.
While tomosynthesis improves cancer detection in women with fatty breasts, scattered fibroglandular breast tissue, and heterogeneously dense breasts, it does not significantly improve cancer detection in women with extremely dense breasts.5,6 Current American Cancer Society and National Comprehensive Cancer Network guidelines recommend annual screening MRI for women at high risk for breast cancer (regardless of breast density); however, increasingly, research supports the effectiveness of MRI in women with dense breasts who are otherwise considered average risk. A large randomized controlled trial in the Netherlands compared outcomes in women with extremely dense breasts invited to have screening MRI after negative mammography to those assigned to continue receiving screening mammography only. The incremental cancer detection rate was 16.5 per 1,000 (79/4,783) women screened with MRI in the first round7 and 6 per 1,000 women screened in the second round 2 years later.8 The interval cancer rate was 0.8 per 1,000 (4/4,783) women screened with MRI, compared with 4.9 per 1,000 (16/3,278) women who declined MRI and received mammography only.7
Screening ultrasound will show up to 3 additional cancers per 1,000 women screened after mammography/tomosynthesis (reviewed in Vourtsis and Berg9 and Berg and Vourtsis10), far lower than the added cancer-detection rate of MRI. Consider screening ultrasound for women who cannot tolerate or access screening MRI.11 Contrast-enhanced mammography (CEM) uses iodinated contrast (as in computed tomography). CEM is not widely available but appears to show cancer-detection similar to MRI. For further discussion, see Berg et al’s 2021 review.3
The FIGURE shows an example of an invasive cancer depicted on contrast-enhanced MRI in a 53-year-old woman with dense breasts and a family history of breast cancer that was not visible on tomosynthesis, even in retrospect, due to masking by dense tissue.
Considerations
Breast MRI increases callbacks even after mammography and ultrasound; however, such false alarms are reduced in subsequent screening rounds. MRI cannot be performed in women who have certain metal implants— some pacemakers or spinal fixation rods—and is not recommended for pregnant women. Claustrophobia may be an issue for some women. MRI is expensive and requires IV contrast. Gadolinium is known to accumulate in the brain, although the long-term effects of this are unknown and no harm has been shown.●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
Text copyright DenseBreast-info.org.
Answer
A. For women with extremely dense breasts who are not otherwise at increased risk for breast cancer, screening magnetic resonance imaging (MRI) is preferred, plus her mammogram or tomosynthesis. If MRI is not an option, consider ultrasonography or contrast-enhanced mammography.
The same screening considerations apply to women with heterogeneously dense breasts; however, there is limited capacity for MRI or even ultrasound screening at many facilities. Research supports MRI in dense breasts, and abbreviated, lower-cost protocols have been validated that address some of the barriers to MRI.1 Although not yet widely available, abbreviated MRI will likely have a greater role in screening women with dense breasts who are not high risk. It is important to note that preauthorization from insurance may be required for screening MRI, and in most US states, deductibles and copays apply.
The exam
Contrast-enhanced MRI requires IV injection of gadolinium-based contrast to look at the anatomy and blood flow patterns of the breast tissue. The patient lies face down with the breasts placed in two rectangular openings, or “coils.” The exam takes place inside the tunnel of the scanner, with the head facing out.After initial images are obtained, the contrast agent is injected into a vein in the arm, and additional images are taken, which will show areas of enhancement. The exam takes about 20 to 40 minutes. An “abbreviated” MRI can be performed for screening in some centers, which uses fewer sequences and takes about 10 minutes.
Benefits
At least 40% of cancers are missed on mammography in women with dense breasts.2 MRI is the most widely studied technique using a contrast agent, and it produces the highest additional cancer detection of all the supplemental technologies to date, yielding, in the first year, 10-16 additional cancers per 1,000 women screened after mammography/tomosynthesis (reviewed in Berg et al.3). The cancer-detection benefit is seen across all breast density categories, even among average-risk women.4 There is no ionizing radiation, and it has been shown to reduce the rate of interval cancers (those detected due to symptoms after a negative screening mammogram), as well as the rate of late-stage disease. Axillary lymph nodes can be examined at the same screening exam.
While tomosynthesis improves cancer detection in women with fatty breasts, scattered fibroglandular breast tissue, and heterogeneously dense breasts, it does not significantly improve cancer detection in women with extremely dense breasts.5,6 Current American Cancer Society and National Comprehensive Cancer Network guidelines recommend annual screening MRI for women at high risk for breast cancer (regardless of breast density); however, increasingly, research supports the effectiveness of MRI in women with dense breasts who are otherwise considered average risk. A large randomized controlled trial in the Netherlands compared outcomes in women with extremely dense breasts invited to have screening MRI after negative mammography to those assigned to continue receiving screening mammography only. The incremental cancer detection rate was 16.5 per 1,000 (79/4,783) women screened with MRI in the first round7 and 6 per 1,000 women screened in the second round 2 years later.8 The interval cancer rate was 0.8 per 1,000 (4/4,783) women screened with MRI, compared with 4.9 per 1,000 (16/3,278) women who declined MRI and received mammography only.7
Screening ultrasound will show up to 3 additional cancers per 1,000 women screened after mammography/tomosynthesis (reviewed in Vourtsis and Berg9 and Berg and Vourtsis10), far lower than the added cancer-detection rate of MRI. Consider screening ultrasound for women who cannot tolerate or access screening MRI.11 Contrast-enhanced mammography (CEM) uses iodinated contrast (as in computed tomography). CEM is not widely available but appears to show cancer-detection similar to MRI. For further discussion, see Berg et al’s 2021 review.3
The FIGURE shows an example of an invasive cancer depicted on contrast-enhanced MRI in a 53-year-old woman with dense breasts and a family history of breast cancer that was not visible on tomosynthesis, even in retrospect, due to masking by dense tissue.
Considerations
Breast MRI increases callbacks even after mammography and ultrasound; however, such false alarms are reduced in subsequent screening rounds. MRI cannot be performed in women who have certain metal implants— some pacemakers or spinal fixation rods—and is not recommended for pregnant women. Claustrophobia may be an issue for some women. MRI is expensive and requires IV contrast. Gadolinium is known to accumulate in the brain, although the long-term effects of this are unknown and no harm has been shown.●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
- Comstock CE, Gatsonis C, Newstead GM, et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening. JAMA. 2020;323:746-756. doi: 10.1001 /jama.2020.0572
- Kerlikowske K, Zhu W, Tosteson AN, et al. Identifying women with dense breasts at high risk for interval cancer: a cohort study. Ann Intern Med. 2015;162:673-681. doi: 10.7326/M14-1465.
- Berg WA, Rafferty EA, Friedewald SM, Hruska CB, Rahbar H. Screening Algorithms in Dense Breasts: AJR Expert Panel Narrative Review. AJR Am J Roentgenol. 2021;216:275-294. doi: 10.2214/AJR.20.24436.
- Kuhl CK, Strobel K, Bieling H, et al. Supplemental breast MR imaging screening of women with average risk of breast cancer. Radiology. 2017;283:361-370. doi: 10.1148/radiol.2016161444.
- Rafferty EA, Durand MA, Conant EF, et al. Breast cancer screening using tomosynthesis and digital mammography in dense and nondense breasts. JAMA. 2016;315:1784-1786. doi: 10.1001/jama.2016.1708.
- Osteras BH, Martinsen ACT, Gullien R, et al. Digital mammography versus breast tomosynthesis: impact of breast density on diagnostic performance in population-based screening. Radiology. 2019;293:60-68. doi: 10.1148 /radiol.2019190425.
- Bakker MF, de Lange SV, Pijnappel RM, et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102. doi: 10.1056/NEJMoa1903986.
- Veenhuizen SGA, de Lange SV, Bakker MF, et al. Supplemental breast MRI for women with extremely dense breasts: results of the second screening round of the DENSE trial. Radiology. 2021;299:278-286. doi: 10.1148/radiol.2021203633.
- Vourtsis A, Berg WA. Breast density implications and supplemental screening. Eur Radiol. 2019;29:1762-1777. doi: 10.1007/s00330-018-5668-8.
- Berg WA, Vourtsis A. Screening ultrasound using handheld or automated technique in women with dense breasts. J Breast Imaging. 2019;1:283-296.
- National Comprehensive Cancer Network. Breast Cancer Screening and Diagnosis (Version 1.2021). https://www.nccn. org/professionals/physician_gls/pdf/breast-screening.pdf. Accessed November 18, 2021.
- Comstock CE, Gatsonis C, Newstead GM, et al. Comparison of abbreviated breast MRI vs digital breast tomosynthesis for breast cancer detection among women with dense breasts undergoing screening. JAMA. 2020;323:746-756. doi: 10.1001 /jama.2020.0572
- Kerlikowske K, Zhu W, Tosteson AN, et al. Identifying women with dense breasts at high risk for interval cancer: a cohort study. Ann Intern Med. 2015;162:673-681. doi: 10.7326/M14-1465.
- Berg WA, Rafferty EA, Friedewald SM, Hruska CB, Rahbar H. Screening Algorithms in Dense Breasts: AJR Expert Panel Narrative Review. AJR Am J Roentgenol. 2021;216:275-294. doi: 10.2214/AJR.20.24436.
- Kuhl CK, Strobel K, Bieling H, et al. Supplemental breast MR imaging screening of women with average risk of breast cancer. Radiology. 2017;283:361-370. doi: 10.1148/radiol.2016161444.
- Rafferty EA, Durand MA, Conant EF, et al. Breast cancer screening using tomosynthesis and digital mammography in dense and nondense breasts. JAMA. 2016;315:1784-1786. doi: 10.1001/jama.2016.1708.
- Osteras BH, Martinsen ACT, Gullien R, et al. Digital mammography versus breast tomosynthesis: impact of breast density on diagnostic performance in population-based screening. Radiology. 2019;293:60-68. doi: 10.1148 /radiol.2019190425.
- Bakker MF, de Lange SV, Pijnappel RM, et al. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102. doi: 10.1056/NEJMoa1903986.
- Veenhuizen SGA, de Lange SV, Bakker MF, et al. Supplemental breast MRI for women with extremely dense breasts: results of the second screening round of the DENSE trial. Radiology. 2021;299:278-286. doi: 10.1148/radiol.2021203633.
- Vourtsis A, Berg WA. Breast density implications and supplemental screening. Eur Radiol. 2019;29:1762-1777. doi: 10.1007/s00330-018-5668-8.
- Berg WA, Vourtsis A. Screening ultrasound using handheld or automated technique in women with dense breasts. J Breast Imaging. 2019;1:283-296.
- National Comprehensive Cancer Network. Breast Cancer Screening and Diagnosis (Version 1.2021). https://www.nccn. org/professionals/physician_gls/pdf/breast-screening.pdf. Accessed November 18, 2021.
Quiz developed in collaboration with ![]()