User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Biologics linked to fewer hospitalizations after asthma exacerbation
In a real-world study of asthma patients,
The data fill a gap, according to Sushan Gupta, MD, who presented the results at the annual meeting of the American College of Chest Physicians. “There’s some ample real-world data that shows that biologics reduce the incidence of asthma exacerbation, but the data regarding what happens after an exacerbation is still lacking, especially real-world data,” said Dr. Gupta, who is a resident at Carle Foundation Hospital in Champaign, Ill.
The findings were encouraging. “Patients with severe asthma on biologics fare well even after an exacerbation event, which includes a reduced incidence of hospitalization, ICU admission, and need for mechanical ventilation. We did not have any patient in the biologic group that required intubation, so that is pretty significant as compared to other patients who did not receive biologics,” said Dr. Gupta.
The results weren’t surprising, but underscore the benefits of biologics, according to Brittany Duchene, MD, who moderated the session where the results were presented. “I think it reinforced that they’re really good drugs,” said Dr. Duchene, who is a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
Although the study was retrospective, it suggests that the threshold for initiating biologics could potentially be lowered for patients with uncontrolled asthma despite adequate use of inhalers, according to Dr. Gupta. “Should that threshold be lower, and would that improve the overall morbidity and eventually the health care cost of utilization? Our study does not prove any of those data, but moving forward that data will also come out.”
Dr. Duchene noted that the accumulating scientific and clinical data for biologics is “really, really strong.” She also speculated that biologics could be used increasingly in the acute setting, which she admitted is a controversial topic. “I think there’s going to be a lot more push to early initiation, and you can see from the [new] study that it decreased a lot of hospitalizations.”
Dr. Gupta emphasized the need for prospective studies, and Dr. Duchene agreed that any such change would need to be patient centric, considering the diversity of available biologics. “It depends what their true issue is. The broader the biologic [mechanism of action], probably the more success you’ll have. I’ve found there’s not a pure allergic or a pure eosinophilic asthma patient. They’re usually more a combination.”
Some key questions remain about biologics treatment, especially in the long term. These include when a patient should be switched from one biologic to another, and whether biologic treatment should be continued over the patient’s lifetime and potential long-term side effects. “I think that data is still evolving and will come to us with time,” said Dr. Gupta.
The researchers analyzed retrospective data from 316 asthma patients treated with biologics and 9,645 treated with nonbiologic therapy between February 2018 and February 2023 at a tertiary care teaching hospital in the Midwest. There was a higher proportion of females in the biologics (69.7%) and nonbiologics groups (63.8%, P = .032), but there was no significant difference in the proportion of Whites in the biologics and nonbiologics groups (78.2% vs. 74.3%, P = .103).
The lack of a difference in racial groups was a surprise, according to Dr. Duchene, especially since other studies have noted disparities in biologic therapy among asthma patients.
Among the biologics group, 0.9% were hospitalized during the study period, compared with 6.5% of the nonbiologics group (P = .00006). They also had fewer ICU visits (0.3% vs. 1.8%; P = .04).
Dr. Gupta’s team attempted to subdivide the data by individual biologic, but there was no statistical significance in outcomes between biologics, perhaps because of the relatively small sample size.
Dr. Gupta noted that his group’s results are generally similar to other studies, including a U.S. study that found a decrease in exacerbation rates after staring or switching biologics and a slightly higher prevalence of biologics use among White patients (77% of biologic users versus 71% of nonbiologics users). A study in southwestern England found fewer ED visits and hospitalizations among patients on biologics.
Dr. Gupta and Dr. Duchene have no relevant financial disclosures.
In a real-world study of asthma patients,
The data fill a gap, according to Sushan Gupta, MD, who presented the results at the annual meeting of the American College of Chest Physicians. “There’s some ample real-world data that shows that biologics reduce the incidence of asthma exacerbation, but the data regarding what happens after an exacerbation is still lacking, especially real-world data,” said Dr. Gupta, who is a resident at Carle Foundation Hospital in Champaign, Ill.
The findings were encouraging. “Patients with severe asthma on biologics fare well even after an exacerbation event, which includes a reduced incidence of hospitalization, ICU admission, and need for mechanical ventilation. We did not have any patient in the biologic group that required intubation, so that is pretty significant as compared to other patients who did not receive biologics,” said Dr. Gupta.
The results weren’t surprising, but underscore the benefits of biologics, according to Brittany Duchene, MD, who moderated the session where the results were presented. “I think it reinforced that they’re really good drugs,” said Dr. Duchene, who is a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
Although the study was retrospective, it suggests that the threshold for initiating biologics could potentially be lowered for patients with uncontrolled asthma despite adequate use of inhalers, according to Dr. Gupta. “Should that threshold be lower, and would that improve the overall morbidity and eventually the health care cost of utilization? Our study does not prove any of those data, but moving forward that data will also come out.”
Dr. Duchene noted that the accumulating scientific and clinical data for biologics is “really, really strong.” She also speculated that biologics could be used increasingly in the acute setting, which she admitted is a controversial topic. “I think there’s going to be a lot more push to early initiation, and you can see from the [new] study that it decreased a lot of hospitalizations.”
Dr. Gupta emphasized the need for prospective studies, and Dr. Duchene agreed that any such change would need to be patient centric, considering the diversity of available biologics. “It depends what their true issue is. The broader the biologic [mechanism of action], probably the more success you’ll have. I’ve found there’s not a pure allergic or a pure eosinophilic asthma patient. They’re usually more a combination.”
Some key questions remain about biologics treatment, especially in the long term. These include when a patient should be switched from one biologic to another, and whether biologic treatment should be continued over the patient’s lifetime and potential long-term side effects. “I think that data is still evolving and will come to us with time,” said Dr. Gupta.
The researchers analyzed retrospective data from 316 asthma patients treated with biologics and 9,645 treated with nonbiologic therapy between February 2018 and February 2023 at a tertiary care teaching hospital in the Midwest. There was a higher proportion of females in the biologics (69.7%) and nonbiologics groups (63.8%, P = .032), but there was no significant difference in the proportion of Whites in the biologics and nonbiologics groups (78.2% vs. 74.3%, P = .103).
The lack of a difference in racial groups was a surprise, according to Dr. Duchene, especially since other studies have noted disparities in biologic therapy among asthma patients.
Among the biologics group, 0.9% were hospitalized during the study period, compared with 6.5% of the nonbiologics group (P = .00006). They also had fewer ICU visits (0.3% vs. 1.8%; P = .04).
Dr. Gupta’s team attempted to subdivide the data by individual biologic, but there was no statistical significance in outcomes between biologics, perhaps because of the relatively small sample size.
Dr. Gupta noted that his group’s results are generally similar to other studies, including a U.S. study that found a decrease in exacerbation rates after staring or switching biologics and a slightly higher prevalence of biologics use among White patients (77% of biologic users versus 71% of nonbiologics users). A study in southwestern England found fewer ED visits and hospitalizations among patients on biologics.
Dr. Gupta and Dr. Duchene have no relevant financial disclosures.
In a real-world study of asthma patients,
The data fill a gap, according to Sushan Gupta, MD, who presented the results at the annual meeting of the American College of Chest Physicians. “There’s some ample real-world data that shows that biologics reduce the incidence of asthma exacerbation, but the data regarding what happens after an exacerbation is still lacking, especially real-world data,” said Dr. Gupta, who is a resident at Carle Foundation Hospital in Champaign, Ill.
The findings were encouraging. “Patients with severe asthma on biologics fare well even after an exacerbation event, which includes a reduced incidence of hospitalization, ICU admission, and need for mechanical ventilation. We did not have any patient in the biologic group that required intubation, so that is pretty significant as compared to other patients who did not receive biologics,” said Dr. Gupta.
The results weren’t surprising, but underscore the benefits of biologics, according to Brittany Duchene, MD, who moderated the session where the results were presented. “I think it reinforced that they’re really good drugs,” said Dr. Duchene, who is a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
Although the study was retrospective, it suggests that the threshold for initiating biologics could potentially be lowered for patients with uncontrolled asthma despite adequate use of inhalers, according to Dr. Gupta. “Should that threshold be lower, and would that improve the overall morbidity and eventually the health care cost of utilization? Our study does not prove any of those data, but moving forward that data will also come out.”
Dr. Duchene noted that the accumulating scientific and clinical data for biologics is “really, really strong.” She also speculated that biologics could be used increasingly in the acute setting, which she admitted is a controversial topic. “I think there’s going to be a lot more push to early initiation, and you can see from the [new] study that it decreased a lot of hospitalizations.”
Dr. Gupta emphasized the need for prospective studies, and Dr. Duchene agreed that any such change would need to be patient centric, considering the diversity of available biologics. “It depends what their true issue is. The broader the biologic [mechanism of action], probably the more success you’ll have. I’ve found there’s not a pure allergic or a pure eosinophilic asthma patient. They’re usually more a combination.”
Some key questions remain about biologics treatment, especially in the long term. These include when a patient should be switched from one biologic to another, and whether biologic treatment should be continued over the patient’s lifetime and potential long-term side effects. “I think that data is still evolving and will come to us with time,” said Dr. Gupta.
The researchers analyzed retrospective data from 316 asthma patients treated with biologics and 9,645 treated with nonbiologic therapy between February 2018 and February 2023 at a tertiary care teaching hospital in the Midwest. There was a higher proportion of females in the biologics (69.7%) and nonbiologics groups (63.8%, P = .032), but there was no significant difference in the proportion of Whites in the biologics and nonbiologics groups (78.2% vs. 74.3%, P = .103).
The lack of a difference in racial groups was a surprise, according to Dr. Duchene, especially since other studies have noted disparities in biologic therapy among asthma patients.
Among the biologics group, 0.9% were hospitalized during the study period, compared with 6.5% of the nonbiologics group (P = .00006). They also had fewer ICU visits (0.3% vs. 1.8%; P = .04).
Dr. Gupta’s team attempted to subdivide the data by individual biologic, but there was no statistical significance in outcomes between biologics, perhaps because of the relatively small sample size.
Dr. Gupta noted that his group’s results are generally similar to other studies, including a U.S. study that found a decrease in exacerbation rates after staring or switching biologics and a slightly higher prevalence of biologics use among White patients (77% of biologic users versus 71% of nonbiologics users). A study in southwestern England found fewer ED visits and hospitalizations among patients on biologics.
Dr. Gupta and Dr. Duchene have no relevant financial disclosures.
FROM CHEST 2023
Running vs. meds for depression: Is there a clear winner?
BARCELONA – However, running provides greater physical health benefits while adherence is greater with drug treatment.
“Both interventions helped with the depression to around the same extent,” study presenter Brenda W.J.H. Penninx, PhD, professor of psychiatric epidemiology at the VU University Medical Center in Amsterdam said in a release.
However, medication “generally had worse impact on body weight, heart rate variability, and blood pressure, whereas running therapy led to improved effect on general fitness and heart rate,” Dr. Penninx added.
The findings were presented at the annual congress of the European College of Neuropsychopharmacology and recently published in the Journal of Affective Disorders.
Research gap
Previous research suggests exercise interventions can have a therapeutic effect equivalent to antidepressants, but their impact on physical health has been “poorly examined in a psychiatric population, the investigators note.
The authors note that depressive and anxiety disorders “cause immense suffering by compromising both mental and physical health,” and the need for effective treatments is “pressing.”
Although antidepressant medication is considered a “standard first-line treatment” alongside psychotherapy, the drugs are “not effective for all and [are] often associated with side effects.”
The Mood Treatment with Antidepressant or Running (MOTAR) study was a partially randomized pragmatic trial in adults with depression and/or anxiety disorder, as determined using the DSM-IV algorithms with the Composite International Diagnostic Interview (CIDI).
The 16-week intervention study included 141 patients with depression and/or anxiety. The mean age was 38.2 years and 58% were women. Participants were offered a choice of treatment: 16 weeks of treatment with the selective serotonin reuptake inhibitor (SSRI) escitalopram (Lexapro) or a 16-week group-based running therapy.
Patients without a strong preference for treatment allocation were randomly assigned to either antidepressant medication or running therapy, while those unwilling to be randomized were allocated to their preferred intervention.
A total of 22 patients were randomly assigned to receive antidepressant treatment and 13 to running therapy. A total of 36 participants chose antidepressant treatment, while 83 chose the running therapy.
Running therapy involved 16 weeks of supervised 45-minute outdoor running sessions to a target of two to three sessions per week, in line with U.S. Centers for Disease Control and Prevention/American College of Sports Medicine recommendations.
Physical health benefits
Treatment adherence in the antidepressant group, defined as still using treatment at the posttreatment assessment, was 82.2% vs. 52.1% among running therapy participants, where adherence was specified as completing more than 22 sessions.
Remission was defined as no longer meeting the criteria of a current depressive or anxiety disorder via CIDI at week 16.
On intention-to-treat analysis, this requirement was met by 44.8% of patients taking antidepressants and 43.3% of those in the running therapy group (P = .88).
However, running therapy patients showed significant improvements in weight (P = .001), waist circumference (P = .011), systolic and diastolic blood pressure (P = .011 and P = .002, respectively), heart rate (P = .033), and heart rate variability (P = .006).
The investigators note the more favorable physical health changes in the running therapy group were attributable to “larger improvements in the running therapy group but also due to larger deterioration in the antidepressant group.”
Antidepressants are generally safe and effective and work for most people, said Dr. Penninx. She also noted that untreated depression leads to worse outcomes, so “antidepressants are generally a good choice.”
Nevertheless, she said, “we need to extend our treatment arsenal as not all patients respond to antidepressants or are willing to take them.”
The study’s results, she added, suggest that “implementing exercise therapy is something we should take much more seriously, as it could be a good, and maybe even better, choice for some of our patients.”
Francesca Cirulli, PhD, senior researcher and group leader at the National Institute of Health, Rome, said in an interview that the study is notable because it is one of the first to prospectively measure the effects of antidepressants and running on physical health.
Dr. Cirulli suggested that running therapy could be tried ahead of treatment with antidepressants if patients prefer physical exercise and can adhere to it. However, she said, the findings also suggest that an increase in physical activity should accompany treatment with antidepressant medications.
Overall, Dr. Cirulli said “the message should not be that everyone can be helped by running and antidepressants are bad,” but rather “these are both helpful, but not excellent, interventions against depression.”
‘Important limitations’
In a comment, Eduard Vieta, MD, PhD, chair of the department of psychiatry and psychology at the University of Barcelona Hospital Clinic, noted the study has “very important limitations.”
Among the limitations: the inclusion of nonrandomized patients who received the treatment of their choice, causing obvious bias and the “lack of binding and power issues” over the number of patients enrolled.
Dr. Vieta also said that the results “seem obvious, because it is known that exercise improves physical health.”
The trial therefore shows, “if you can find people who are able to do exercise while depressed and adhere to it, those would benefit from that practice,” he noted.
Also commenting on the research, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said the results are confirmatory and “again show physical health can influence mental health.”
However, Dr. Ruhe underlined, while it is “common practice” to allow patients to follow their treatment preference and is “understandable from a pragmatic point of view,” the group comparison may be “biased,” compared with a “truly randomized study.”
“For example, patients in the antidepressant group were more depressed, which might be associated with less chance of persisting engagement in the exercises,” he said. “So, we have to be careful not to overinterpret the comparisons between groups, which the authors acknowledge properly.”
Turning to the difference in adherence between the two interventions, Dr. Ruhe said the results show adopting, and adhering to, a lifestyle habit is more difficult than taking a pill.
“This is not exclusively found in psychiatry, indicating that we also have to focus on how to improve compliance to healthy behavior. This could have tremendous impact on health care more generally, but also on psychiatric diseases,” Dr. Ruhe said.
The MOTAR study was funded by a NWO-VICI grant. Funding for the inflammatory markers was provided by ZonMw: The Netherlands Organization for Health Research and Development. The study authors and clinicians interviewed for this story declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BARCELONA – However, running provides greater physical health benefits while adherence is greater with drug treatment.
“Both interventions helped with the depression to around the same extent,” study presenter Brenda W.J.H. Penninx, PhD, professor of psychiatric epidemiology at the VU University Medical Center in Amsterdam said in a release.
However, medication “generally had worse impact on body weight, heart rate variability, and blood pressure, whereas running therapy led to improved effect on general fitness and heart rate,” Dr. Penninx added.
The findings were presented at the annual congress of the European College of Neuropsychopharmacology and recently published in the Journal of Affective Disorders.
Research gap
Previous research suggests exercise interventions can have a therapeutic effect equivalent to antidepressants, but their impact on physical health has been “poorly examined in a psychiatric population, the investigators note.
The authors note that depressive and anxiety disorders “cause immense suffering by compromising both mental and physical health,” and the need for effective treatments is “pressing.”
Although antidepressant medication is considered a “standard first-line treatment” alongside psychotherapy, the drugs are “not effective for all and [are] often associated with side effects.”
The Mood Treatment with Antidepressant or Running (MOTAR) study was a partially randomized pragmatic trial in adults with depression and/or anxiety disorder, as determined using the DSM-IV algorithms with the Composite International Diagnostic Interview (CIDI).
The 16-week intervention study included 141 patients with depression and/or anxiety. The mean age was 38.2 years and 58% were women. Participants were offered a choice of treatment: 16 weeks of treatment with the selective serotonin reuptake inhibitor (SSRI) escitalopram (Lexapro) or a 16-week group-based running therapy.
Patients without a strong preference for treatment allocation were randomly assigned to either antidepressant medication or running therapy, while those unwilling to be randomized were allocated to their preferred intervention.
A total of 22 patients were randomly assigned to receive antidepressant treatment and 13 to running therapy. A total of 36 participants chose antidepressant treatment, while 83 chose the running therapy.
Running therapy involved 16 weeks of supervised 45-minute outdoor running sessions to a target of two to three sessions per week, in line with U.S. Centers for Disease Control and Prevention/American College of Sports Medicine recommendations.
Physical health benefits
Treatment adherence in the antidepressant group, defined as still using treatment at the posttreatment assessment, was 82.2% vs. 52.1% among running therapy participants, where adherence was specified as completing more than 22 sessions.
Remission was defined as no longer meeting the criteria of a current depressive or anxiety disorder via CIDI at week 16.
On intention-to-treat analysis, this requirement was met by 44.8% of patients taking antidepressants and 43.3% of those in the running therapy group (P = .88).
However, running therapy patients showed significant improvements in weight (P = .001), waist circumference (P = .011), systolic and diastolic blood pressure (P = .011 and P = .002, respectively), heart rate (P = .033), and heart rate variability (P = .006).
The investigators note the more favorable physical health changes in the running therapy group were attributable to “larger improvements in the running therapy group but also due to larger deterioration in the antidepressant group.”
Antidepressants are generally safe and effective and work for most people, said Dr. Penninx. She also noted that untreated depression leads to worse outcomes, so “antidepressants are generally a good choice.”
Nevertheless, she said, “we need to extend our treatment arsenal as not all patients respond to antidepressants or are willing to take them.”
The study’s results, she added, suggest that “implementing exercise therapy is something we should take much more seriously, as it could be a good, and maybe even better, choice for some of our patients.”
Francesca Cirulli, PhD, senior researcher and group leader at the National Institute of Health, Rome, said in an interview that the study is notable because it is one of the first to prospectively measure the effects of antidepressants and running on physical health.
Dr. Cirulli suggested that running therapy could be tried ahead of treatment with antidepressants if patients prefer physical exercise and can adhere to it. However, she said, the findings also suggest that an increase in physical activity should accompany treatment with antidepressant medications.
Overall, Dr. Cirulli said “the message should not be that everyone can be helped by running and antidepressants are bad,” but rather “these are both helpful, but not excellent, interventions against depression.”
‘Important limitations’
In a comment, Eduard Vieta, MD, PhD, chair of the department of psychiatry and psychology at the University of Barcelona Hospital Clinic, noted the study has “very important limitations.”
Among the limitations: the inclusion of nonrandomized patients who received the treatment of their choice, causing obvious bias and the “lack of binding and power issues” over the number of patients enrolled.
Dr. Vieta also said that the results “seem obvious, because it is known that exercise improves physical health.”
The trial therefore shows, “if you can find people who are able to do exercise while depressed and adhere to it, those would benefit from that practice,” he noted.
Also commenting on the research, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said the results are confirmatory and “again show physical health can influence mental health.”
However, Dr. Ruhe underlined, while it is “common practice” to allow patients to follow their treatment preference and is “understandable from a pragmatic point of view,” the group comparison may be “biased,” compared with a “truly randomized study.”
“For example, patients in the antidepressant group were more depressed, which might be associated with less chance of persisting engagement in the exercises,” he said. “So, we have to be careful not to overinterpret the comparisons between groups, which the authors acknowledge properly.”
Turning to the difference in adherence between the two interventions, Dr. Ruhe said the results show adopting, and adhering to, a lifestyle habit is more difficult than taking a pill.
“This is not exclusively found in psychiatry, indicating that we also have to focus on how to improve compliance to healthy behavior. This could have tremendous impact on health care more generally, but also on psychiatric diseases,” Dr. Ruhe said.
The MOTAR study was funded by a NWO-VICI grant. Funding for the inflammatory markers was provided by ZonMw: The Netherlands Organization for Health Research and Development. The study authors and clinicians interviewed for this story declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BARCELONA – However, running provides greater physical health benefits while adherence is greater with drug treatment.
“Both interventions helped with the depression to around the same extent,” study presenter Brenda W.J.H. Penninx, PhD, professor of psychiatric epidemiology at the VU University Medical Center in Amsterdam said in a release.
However, medication “generally had worse impact on body weight, heart rate variability, and blood pressure, whereas running therapy led to improved effect on general fitness and heart rate,” Dr. Penninx added.
The findings were presented at the annual congress of the European College of Neuropsychopharmacology and recently published in the Journal of Affective Disorders.
Research gap
Previous research suggests exercise interventions can have a therapeutic effect equivalent to antidepressants, but their impact on physical health has been “poorly examined in a psychiatric population, the investigators note.
The authors note that depressive and anxiety disorders “cause immense suffering by compromising both mental and physical health,” and the need for effective treatments is “pressing.”
Although antidepressant medication is considered a “standard first-line treatment” alongside psychotherapy, the drugs are “not effective for all and [are] often associated with side effects.”
The Mood Treatment with Antidepressant or Running (MOTAR) study was a partially randomized pragmatic trial in adults with depression and/or anxiety disorder, as determined using the DSM-IV algorithms with the Composite International Diagnostic Interview (CIDI).
The 16-week intervention study included 141 patients with depression and/or anxiety. The mean age was 38.2 years and 58% were women. Participants were offered a choice of treatment: 16 weeks of treatment with the selective serotonin reuptake inhibitor (SSRI) escitalopram (Lexapro) or a 16-week group-based running therapy.
Patients without a strong preference for treatment allocation were randomly assigned to either antidepressant medication or running therapy, while those unwilling to be randomized were allocated to their preferred intervention.
A total of 22 patients were randomly assigned to receive antidepressant treatment and 13 to running therapy. A total of 36 participants chose antidepressant treatment, while 83 chose the running therapy.
Running therapy involved 16 weeks of supervised 45-minute outdoor running sessions to a target of two to three sessions per week, in line with U.S. Centers for Disease Control and Prevention/American College of Sports Medicine recommendations.
Physical health benefits
Treatment adherence in the antidepressant group, defined as still using treatment at the posttreatment assessment, was 82.2% vs. 52.1% among running therapy participants, where adherence was specified as completing more than 22 sessions.
Remission was defined as no longer meeting the criteria of a current depressive or anxiety disorder via CIDI at week 16.
On intention-to-treat analysis, this requirement was met by 44.8% of patients taking antidepressants and 43.3% of those in the running therapy group (P = .88).
However, running therapy patients showed significant improvements in weight (P = .001), waist circumference (P = .011), systolic and diastolic blood pressure (P = .011 and P = .002, respectively), heart rate (P = .033), and heart rate variability (P = .006).
The investigators note the more favorable physical health changes in the running therapy group were attributable to “larger improvements in the running therapy group but also due to larger deterioration in the antidepressant group.”
Antidepressants are generally safe and effective and work for most people, said Dr. Penninx. She also noted that untreated depression leads to worse outcomes, so “antidepressants are generally a good choice.”
Nevertheless, she said, “we need to extend our treatment arsenal as not all patients respond to antidepressants or are willing to take them.”
The study’s results, she added, suggest that “implementing exercise therapy is something we should take much more seriously, as it could be a good, and maybe even better, choice for some of our patients.”
Francesca Cirulli, PhD, senior researcher and group leader at the National Institute of Health, Rome, said in an interview that the study is notable because it is one of the first to prospectively measure the effects of antidepressants and running on physical health.
Dr. Cirulli suggested that running therapy could be tried ahead of treatment with antidepressants if patients prefer physical exercise and can adhere to it. However, she said, the findings also suggest that an increase in physical activity should accompany treatment with antidepressant medications.
Overall, Dr. Cirulli said “the message should not be that everyone can be helped by running and antidepressants are bad,” but rather “these are both helpful, but not excellent, interventions against depression.”
‘Important limitations’
In a comment, Eduard Vieta, MD, PhD, chair of the department of psychiatry and psychology at the University of Barcelona Hospital Clinic, noted the study has “very important limitations.”
Among the limitations: the inclusion of nonrandomized patients who received the treatment of their choice, causing obvious bias and the “lack of binding and power issues” over the number of patients enrolled.
Dr. Vieta also said that the results “seem obvious, because it is known that exercise improves physical health.”
The trial therefore shows, “if you can find people who are able to do exercise while depressed and adhere to it, those would benefit from that practice,” he noted.
Also commenting on the research, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said the results are confirmatory and “again show physical health can influence mental health.”
However, Dr. Ruhe underlined, while it is “common practice” to allow patients to follow their treatment preference and is “understandable from a pragmatic point of view,” the group comparison may be “biased,” compared with a “truly randomized study.”
“For example, patients in the antidepressant group were more depressed, which might be associated with less chance of persisting engagement in the exercises,” he said. “So, we have to be careful not to overinterpret the comparisons between groups, which the authors acknowledge properly.”
Turning to the difference in adherence between the two interventions, Dr. Ruhe said the results show adopting, and adhering to, a lifestyle habit is more difficult than taking a pill.
“This is not exclusively found in psychiatry, indicating that we also have to focus on how to improve compliance to healthy behavior. This could have tremendous impact on health care more generally, but also on psychiatric diseases,” Dr. Ruhe said.
The MOTAR study was funded by a NWO-VICI grant. Funding for the inflammatory markers was provided by ZonMw: The Netherlands Organization for Health Research and Development. The study authors and clinicians interviewed for this story declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ECNP 2023
Nintedanib dose reductions in IPF may do no harm
HONOLULU – nintedanib (Ofev) for patients with idiopathic pulmonary fibrosis (IPF) who can’t tolerate the full 150-mg twice-daily dose.
An analysis of data from a large administrative claims database showed that there were no significant differences in either all-cause mortality or hospitalization rates between patients with IPF treated at the full 150-mg twice-daily dose and those treated with a reduced twice-daily dose of 100 mg nintedanib.
Although the results need to be confirmed by additional prospective and registry studies, they suggest that patients with IPF can still fare just as well with a reduced-dose nintedanib regimen, ideally with fewer gastrointestinal side effects such as diarrhea, reported Andrew Limper, MD, of the Mayo Clinic in Rochester, Minn.
“At least on this preliminary data you could ... rest assured,” Dr. Limper told his colleagues in an oral abstract session at the American College of Chest Physicians (CHEST) 2023 annual meeting.
“This is not definitive proof, I’m not making more out of this than it is, but we all put people on 100 mg twice daily because their guts don’t tolerate it; they live in the bathroom and they don’t want to live that way,” Dr. Limper said.
Hard to take
Nintedanib is approved in the United States for the treatment of IPF, chronic fibrosing interstitial lung diseases (ILD) with a progressive phenotype, and systemic sclerosis-associated ILD. For IPF, the standard dose established in randomized clinical trials is 150 mg twice daily.
However, nintedanib is associated with a number of side effects, including hepatic and other gastrointestinal toxicities, arterial thromboembolic events, and proteinuria within the nephrotic range. As a result, clinicians often reduce the dose to 100 mg twice daily, but there is a lack of data to indicate whether it’s safe to do so or if efficacy will be compromised.
To see whether dose reductions might result in poorer outcomes for patients with IPF, Dr. Limper and colleagues analyzed data from the OptumLabs Data Warehouse, a large administrative claims database, to compare outcomes for patients treated with IPF at either the 150-mg or 100-mg twice-daily doses.
They used propensity-score matching to account for differences among individuals according to age, sex, race/ethnicity, residence, insurance type, additional medication use, oxygen use, smoking status, health care use, and comorbidities. The final cohort included 346 patients in each dosing group.
There was no difference between the dosing groups for the primary outcome of all-cause mortality at 18 months, with a nonsignificant hazard ratio of 0.65 (P = .313), and no significant difference over 24 months in risk of hospitalization, with a hazard ratio of 0.98 (P = .899).
“This is not randomized controlled data; I doubt that [nintedanib maker Boehringer Ingelheim] is ever going to do a 150 vs. 100 milligram head-to-head trial, but it does give us some ground to start to look at this,” Dr. Limper said.
Not so sure
Session comoderator Misbah Baqir, MBBS, also from the Mayo Clinic, told this news organization that she would need to see more data from prospective studies using endpoints other than mortality before she could be convinced that nintedanib dose reductions do not adversely affect efficacy. She was not involved in the study.
“I feel that the endpoint should be different, either it should be forced vital capacity change, quality of life, or something else. The problem with a database study is that you don’t have everything in it. You have to play with what you have, and you don’t have forced vital capacity. You have to go into the charts to get it,” she said.
It would be more helpful to objectively compare, for example, diarrhea episodes or other adverse events to see whether they were significantly reduced with the 100-mg dose, she added.
In an interview, Dr. Limper said that he and his colleagues plan to gather additional observational data including the newly available Medicare fee-for-service data set, registry data, and other sources.
“If we get all of that, and it really still looks compelling – and that’s an if – then I think that would be the foothold to go back to the manufacturer and say, ‘Hey, maybe you ought to think about doing a prospective trial to prove it with lung function and other endpoints such as 6-minute walks,’ ” he said.
The study was supported by a grant from Three Lakes Foundation. Dr. Limper and Dr. Baqir have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
HONOLULU – nintedanib (Ofev) for patients with idiopathic pulmonary fibrosis (IPF) who can’t tolerate the full 150-mg twice-daily dose.
An analysis of data from a large administrative claims database showed that there were no significant differences in either all-cause mortality or hospitalization rates between patients with IPF treated at the full 150-mg twice-daily dose and those treated with a reduced twice-daily dose of 100 mg nintedanib.
Although the results need to be confirmed by additional prospective and registry studies, they suggest that patients with IPF can still fare just as well with a reduced-dose nintedanib regimen, ideally with fewer gastrointestinal side effects such as diarrhea, reported Andrew Limper, MD, of the Mayo Clinic in Rochester, Minn.
“At least on this preliminary data you could ... rest assured,” Dr. Limper told his colleagues in an oral abstract session at the American College of Chest Physicians (CHEST) 2023 annual meeting.
“This is not definitive proof, I’m not making more out of this than it is, but we all put people on 100 mg twice daily because their guts don’t tolerate it; they live in the bathroom and they don’t want to live that way,” Dr. Limper said.
Hard to take
Nintedanib is approved in the United States for the treatment of IPF, chronic fibrosing interstitial lung diseases (ILD) with a progressive phenotype, and systemic sclerosis-associated ILD. For IPF, the standard dose established in randomized clinical trials is 150 mg twice daily.
However, nintedanib is associated with a number of side effects, including hepatic and other gastrointestinal toxicities, arterial thromboembolic events, and proteinuria within the nephrotic range. As a result, clinicians often reduce the dose to 100 mg twice daily, but there is a lack of data to indicate whether it’s safe to do so or if efficacy will be compromised.
To see whether dose reductions might result in poorer outcomes for patients with IPF, Dr. Limper and colleagues analyzed data from the OptumLabs Data Warehouse, a large administrative claims database, to compare outcomes for patients treated with IPF at either the 150-mg or 100-mg twice-daily doses.
They used propensity-score matching to account for differences among individuals according to age, sex, race/ethnicity, residence, insurance type, additional medication use, oxygen use, smoking status, health care use, and comorbidities. The final cohort included 346 patients in each dosing group.
There was no difference between the dosing groups for the primary outcome of all-cause mortality at 18 months, with a nonsignificant hazard ratio of 0.65 (P = .313), and no significant difference over 24 months in risk of hospitalization, with a hazard ratio of 0.98 (P = .899).
“This is not randomized controlled data; I doubt that [nintedanib maker Boehringer Ingelheim] is ever going to do a 150 vs. 100 milligram head-to-head trial, but it does give us some ground to start to look at this,” Dr. Limper said.
Not so sure
Session comoderator Misbah Baqir, MBBS, also from the Mayo Clinic, told this news organization that she would need to see more data from prospective studies using endpoints other than mortality before she could be convinced that nintedanib dose reductions do not adversely affect efficacy. She was not involved in the study.
“I feel that the endpoint should be different, either it should be forced vital capacity change, quality of life, or something else. The problem with a database study is that you don’t have everything in it. You have to play with what you have, and you don’t have forced vital capacity. You have to go into the charts to get it,” she said.
It would be more helpful to objectively compare, for example, diarrhea episodes or other adverse events to see whether they were significantly reduced with the 100-mg dose, she added.
In an interview, Dr. Limper said that he and his colleagues plan to gather additional observational data including the newly available Medicare fee-for-service data set, registry data, and other sources.
“If we get all of that, and it really still looks compelling – and that’s an if – then I think that would be the foothold to go back to the manufacturer and say, ‘Hey, maybe you ought to think about doing a prospective trial to prove it with lung function and other endpoints such as 6-minute walks,’ ” he said.
The study was supported by a grant from Three Lakes Foundation. Dr. Limper and Dr. Baqir have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
HONOLULU – nintedanib (Ofev) for patients with idiopathic pulmonary fibrosis (IPF) who can’t tolerate the full 150-mg twice-daily dose.
An analysis of data from a large administrative claims database showed that there were no significant differences in either all-cause mortality or hospitalization rates between patients with IPF treated at the full 150-mg twice-daily dose and those treated with a reduced twice-daily dose of 100 mg nintedanib.
Although the results need to be confirmed by additional prospective and registry studies, they suggest that patients with IPF can still fare just as well with a reduced-dose nintedanib regimen, ideally with fewer gastrointestinal side effects such as diarrhea, reported Andrew Limper, MD, of the Mayo Clinic in Rochester, Minn.
“At least on this preliminary data you could ... rest assured,” Dr. Limper told his colleagues in an oral abstract session at the American College of Chest Physicians (CHEST) 2023 annual meeting.
“This is not definitive proof, I’m not making more out of this than it is, but we all put people on 100 mg twice daily because their guts don’t tolerate it; they live in the bathroom and they don’t want to live that way,” Dr. Limper said.
Hard to take
Nintedanib is approved in the United States for the treatment of IPF, chronic fibrosing interstitial lung diseases (ILD) with a progressive phenotype, and systemic sclerosis-associated ILD. For IPF, the standard dose established in randomized clinical trials is 150 mg twice daily.
However, nintedanib is associated with a number of side effects, including hepatic and other gastrointestinal toxicities, arterial thromboembolic events, and proteinuria within the nephrotic range. As a result, clinicians often reduce the dose to 100 mg twice daily, but there is a lack of data to indicate whether it’s safe to do so or if efficacy will be compromised.
To see whether dose reductions might result in poorer outcomes for patients with IPF, Dr. Limper and colleagues analyzed data from the OptumLabs Data Warehouse, a large administrative claims database, to compare outcomes for patients treated with IPF at either the 150-mg or 100-mg twice-daily doses.
They used propensity-score matching to account for differences among individuals according to age, sex, race/ethnicity, residence, insurance type, additional medication use, oxygen use, smoking status, health care use, and comorbidities. The final cohort included 346 patients in each dosing group.
There was no difference between the dosing groups for the primary outcome of all-cause mortality at 18 months, with a nonsignificant hazard ratio of 0.65 (P = .313), and no significant difference over 24 months in risk of hospitalization, with a hazard ratio of 0.98 (P = .899).
“This is not randomized controlled data; I doubt that [nintedanib maker Boehringer Ingelheim] is ever going to do a 150 vs. 100 milligram head-to-head trial, but it does give us some ground to start to look at this,” Dr. Limper said.
Not so sure
Session comoderator Misbah Baqir, MBBS, also from the Mayo Clinic, told this news organization that she would need to see more data from prospective studies using endpoints other than mortality before she could be convinced that nintedanib dose reductions do not adversely affect efficacy. She was not involved in the study.
“I feel that the endpoint should be different, either it should be forced vital capacity change, quality of life, or something else. The problem with a database study is that you don’t have everything in it. You have to play with what you have, and you don’t have forced vital capacity. You have to go into the charts to get it,” she said.
It would be more helpful to objectively compare, for example, diarrhea episodes or other adverse events to see whether they were significantly reduced with the 100-mg dose, she added.
In an interview, Dr. Limper said that he and his colleagues plan to gather additional observational data including the newly available Medicare fee-for-service data set, registry data, and other sources.
“If we get all of that, and it really still looks compelling – and that’s an if – then I think that would be the foothold to go back to the manufacturer and say, ‘Hey, maybe you ought to think about doing a prospective trial to prove it with lung function and other endpoints such as 6-minute walks,’ ” he said.
The study was supported by a grant from Three Lakes Foundation. Dr. Limper and Dr. Baqir have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
AT CHEST 2023
Are women and men with rheumatism treated equally?
LEIPZIG, GERMANY – Women eat more healthily, visit their physician more often, and accept offers of prophylactic treatment more frequently than their male counterparts. Nevertheless, they are generally diagnosed with a rheumatic disease much later. “With systemic sclerosis for example, diagnosis occurs a whole year later than for male patients,” said Uta Kiltz, MD, senior physician at the Ruhrgebiet Rheumatism Center in Bochum, Germany, at a press conference for the annual congress of the German Society for Rheumatology.
In addition, certain markers and antibodies can be detected earlier in men’s blood – for example in systemic sclerosis. “What’s more, women exhibit a more diverse array of symptoms, which can make an unequivocal diagnosis difficult,” Dr. Kiltz explained.
Differences between the sexes in terms of disease progression and clinical presentation have been described for most rheumatic diseases. Roughly speaking, women often exhibit a much wider range of symptoms and report a higher disease burden, whereas men tend to experience a more severe progression of the disease.
Comorbidities also occur at different rates between the sexes. Whereas women with rheumatoid arthritis suffer more frequently from osteoporosis and depression, men are more likely to develop cardiovascular diseases and diabetes.
Gender-sensitive approach
Like Dr. Kiltz, Susanna Späthling-Mestekemper, MD, PhD, of the Munich-Pasing (Germany) Rheumatology Practice, also advocates a gender-sensitive approach to diagnosis and therapy. Dr. Späthling-Mestekemper referred to this during the conference, stating that women are still treated more poorly than men. The difference in treatment quality results from gaps in knowledge in the following areas:
- Sex-specific differences in the diagnosis and therapy of rheumatic diseases and in basic and clinical research
- Sex-specific differences in communication between male and female patients and between male and female physicians.
Dr. Späthling-Mestekemper used axial spondyloarthritis (axSpA) as a “prominent example” of false diagnoses. “Men more commonly fulfill the modified New York criteria – involvement of the axial skeleton, the lumbar spine, and increasing radiological progression.”
In contrast, women with axSpA exhibit the following differences:
- It is more likely for the cervical spine to be affected.
- Women are more likely to suffer from peripheral joint involvement.
- They suffer more from whole body pain.
- They have fatigue and exhaustion.
- They exhibit fewer humoral signs of inflammation (lower C-reactive protein).
- They are rarely HLA-B27 positive.
“We also have to completely rethink how we make the diagnosis in women,” said Dr. Späthling-Mestekemper. The current approach leads to women with axSpA being diagnosed much later than men. “Depending on the study, the difference can range from 7 months to 2 years,” according to Dr. Späthling-Mestekemper.
A 2018 Spanish study reported that the most common incorrect diagnoses in women with axSpA were sciatica, osteoarthritis, and fibromyalgia.
However, it is not just in axSpA that there are significant differences between men and women. There is evidence that women with systemic lupus erythematosus suffer more from musculoskeletal symptoms, while men with lupus exhibit more severe organ involvement (especially more serositis and nephritis).
For systemic sclerosis, women have the higher survival rate. They also exhibit skin involvement more frequently. Men, however, are more likely to have organ involvement, especially with the lungs.
TNF blockers
Using the example of axSpA, Dr. Späthling-Mestekemper also showed that men and women respond differently to tumor necrosis factor (TNF) blocker therapy. “The duration of therapy with TNF blockers is shorter for women: 33.4 months versus 44.9 months. They respond less to this therapy; they stop and change more frequently.”
Data from March 2023 show that, in contrast, there is no evidence of a difference in response to Janus kinase inhibitor treatment.
The presence of enthesitis has been discussed as one reason for the worse response to TNF blockers in women, since they have it more often than men do. “In fact, a better response to TNF blockers is associated with HLA-B27 positivity, with the absence of enthesitis and with TNF blocker naivety. In women, higher fat-mass index could also play a part, or even abdominal weight gain, which also increases in women after menopause,” said Dr. Späthling-Mestekemper.
She mentioned the following other potential reasons for a delayed therapy response to biological drugs in women:
- Genetic, physical, or hormonal causes
- Widespread pain or fibromyalgia
- Late diagnosis or late application of therapy, which lowers the chances of remission.
Even the science itself has shown the following sex-specific shortcomings:
- Disregarding sex-specific differences in animal-experimental studies (which, until recently, were only conducted in male mice to avoid hormone fluctuations)
- Women in clinical studies are still underrepresented: only 37% of the populations in phase 3 studies are women; 64% of studies do not describe any sex-specific differences
- Most of the data come from epidemiological analyses (not from basic research)
- Gaps in medical textbooks
Communication differences
Female patients are looking for explanations, whereas male patients describe specific symptoms. Female physicians talk, while male physicians treat. They sound like stereotypes, but they have been substantiated in multiple studies, said Dr. Späthling-Mestekemper. In general, the study results show that male patients behave in the following ways:
- Describe their symptoms in terms of specifics
- Do not like to admit having mental health issues
- Are three to five times more likely to commit suicide because of depression than women
On the other hand, female patients behave in the following ways:
- Look for an explanation for their symptoms
- Often do not have their physical symptoms taken seriously
- Are often pushed in a psychosomatic direction.
Female physicians focus on the following questions:
- Prevention, communication, shared decision-making, open-ended questions, “positive” discussions, patient self-management (chronic diseases such as diabetes: female physicians are better at reaching the therapy goals set by the ADA guidelines than male physicians)
- Psychosocial situations: consultations last 1 minute longer (10%).
Male physicians focus on the following questions:
- Medical history
- Physical examination (cardiac catheterizations after a heart attack are arranged much more commonly by male rather than female physicians)
- Diagnostics
Recognition and training
A large-scale surgical study in 2021 made a few waves. The study analyzed whether it makes a difference if women are operated on by men or by women. The results showed that women who had been operated on by men exhibited a higher level of risk after the surgery, compared with men who had been operated on by men or by women. The risk took the following forms:
- 15% higher risk for a worse surgery result
- 16% higher risk for complications
- 11% higher risk for repeat hospitalization
- 20% higher risk for a longer period of hospitalization
- 32% higher risk for mortality
The study authors provided the following potential reasons for these differences:
- Male physicians underestimate the severity of symptoms in their female patients
- Women are less comfortable indicating their postoperative pain to a male physician
- Different working style and treatment decisions between female and male physicians
- Unconsciously incorporated role patterns and preconceptions
“Our potential solutions are recognition and training. We need a personalized style of medicine; we need to have a closer look. We owe our male and female patients as much,” said Dr. Späthling-Mestekemper.
This article was translated from the Medscape German Edition and a version appeared on Medscape.com.
LEIPZIG, GERMANY – Women eat more healthily, visit their physician more often, and accept offers of prophylactic treatment more frequently than their male counterparts. Nevertheless, they are generally diagnosed with a rheumatic disease much later. “With systemic sclerosis for example, diagnosis occurs a whole year later than for male patients,” said Uta Kiltz, MD, senior physician at the Ruhrgebiet Rheumatism Center in Bochum, Germany, at a press conference for the annual congress of the German Society for Rheumatology.
In addition, certain markers and antibodies can be detected earlier in men’s blood – for example in systemic sclerosis. “What’s more, women exhibit a more diverse array of symptoms, which can make an unequivocal diagnosis difficult,” Dr. Kiltz explained.
Differences between the sexes in terms of disease progression and clinical presentation have been described for most rheumatic diseases. Roughly speaking, women often exhibit a much wider range of symptoms and report a higher disease burden, whereas men tend to experience a more severe progression of the disease.
Comorbidities also occur at different rates between the sexes. Whereas women with rheumatoid arthritis suffer more frequently from osteoporosis and depression, men are more likely to develop cardiovascular diseases and diabetes.
Gender-sensitive approach
Like Dr. Kiltz, Susanna Späthling-Mestekemper, MD, PhD, of the Munich-Pasing (Germany) Rheumatology Practice, also advocates a gender-sensitive approach to diagnosis and therapy. Dr. Späthling-Mestekemper referred to this during the conference, stating that women are still treated more poorly than men. The difference in treatment quality results from gaps in knowledge in the following areas:
- Sex-specific differences in the diagnosis and therapy of rheumatic diseases and in basic and clinical research
- Sex-specific differences in communication between male and female patients and between male and female physicians.
Dr. Späthling-Mestekemper used axial spondyloarthritis (axSpA) as a “prominent example” of false diagnoses. “Men more commonly fulfill the modified New York criteria – involvement of the axial skeleton, the lumbar spine, and increasing radiological progression.”
In contrast, women with axSpA exhibit the following differences:
- It is more likely for the cervical spine to be affected.
- Women are more likely to suffer from peripheral joint involvement.
- They suffer more from whole body pain.
- They have fatigue and exhaustion.
- They exhibit fewer humoral signs of inflammation (lower C-reactive protein).
- They are rarely HLA-B27 positive.
“We also have to completely rethink how we make the diagnosis in women,” said Dr. Späthling-Mestekemper. The current approach leads to women with axSpA being diagnosed much later than men. “Depending on the study, the difference can range from 7 months to 2 years,” according to Dr. Späthling-Mestekemper.
A 2018 Spanish study reported that the most common incorrect diagnoses in women with axSpA were sciatica, osteoarthritis, and fibromyalgia.
However, it is not just in axSpA that there are significant differences between men and women. There is evidence that women with systemic lupus erythematosus suffer more from musculoskeletal symptoms, while men with lupus exhibit more severe organ involvement (especially more serositis and nephritis).
For systemic sclerosis, women have the higher survival rate. They also exhibit skin involvement more frequently. Men, however, are more likely to have organ involvement, especially with the lungs.
TNF blockers
Using the example of axSpA, Dr. Späthling-Mestekemper also showed that men and women respond differently to tumor necrosis factor (TNF) blocker therapy. “The duration of therapy with TNF blockers is shorter for women: 33.4 months versus 44.9 months. They respond less to this therapy; they stop and change more frequently.”
Data from March 2023 show that, in contrast, there is no evidence of a difference in response to Janus kinase inhibitor treatment.
The presence of enthesitis has been discussed as one reason for the worse response to TNF blockers in women, since they have it more often than men do. “In fact, a better response to TNF blockers is associated with HLA-B27 positivity, with the absence of enthesitis and with TNF blocker naivety. In women, higher fat-mass index could also play a part, or even abdominal weight gain, which also increases in women after menopause,” said Dr. Späthling-Mestekemper.
She mentioned the following other potential reasons for a delayed therapy response to biological drugs in women:
- Genetic, physical, or hormonal causes
- Widespread pain or fibromyalgia
- Late diagnosis or late application of therapy, which lowers the chances of remission.
Even the science itself has shown the following sex-specific shortcomings:
- Disregarding sex-specific differences in animal-experimental studies (which, until recently, were only conducted in male mice to avoid hormone fluctuations)
- Women in clinical studies are still underrepresented: only 37% of the populations in phase 3 studies are women; 64% of studies do not describe any sex-specific differences
- Most of the data come from epidemiological analyses (not from basic research)
- Gaps in medical textbooks
Communication differences
Female patients are looking for explanations, whereas male patients describe specific symptoms. Female physicians talk, while male physicians treat. They sound like stereotypes, but they have been substantiated in multiple studies, said Dr. Späthling-Mestekemper. In general, the study results show that male patients behave in the following ways:
- Describe their symptoms in terms of specifics
- Do not like to admit having mental health issues
- Are three to five times more likely to commit suicide because of depression than women
On the other hand, female patients behave in the following ways:
- Look for an explanation for their symptoms
- Often do not have their physical symptoms taken seriously
- Are often pushed in a psychosomatic direction.
Female physicians focus on the following questions:
- Prevention, communication, shared decision-making, open-ended questions, “positive” discussions, patient self-management (chronic diseases such as diabetes: female physicians are better at reaching the therapy goals set by the ADA guidelines than male physicians)
- Psychosocial situations: consultations last 1 minute longer (10%).
Male physicians focus on the following questions:
- Medical history
- Physical examination (cardiac catheterizations after a heart attack are arranged much more commonly by male rather than female physicians)
- Diagnostics
Recognition and training
A large-scale surgical study in 2021 made a few waves. The study analyzed whether it makes a difference if women are operated on by men or by women. The results showed that women who had been operated on by men exhibited a higher level of risk after the surgery, compared with men who had been operated on by men or by women. The risk took the following forms:
- 15% higher risk for a worse surgery result
- 16% higher risk for complications
- 11% higher risk for repeat hospitalization
- 20% higher risk for a longer period of hospitalization
- 32% higher risk for mortality
The study authors provided the following potential reasons for these differences:
- Male physicians underestimate the severity of symptoms in their female patients
- Women are less comfortable indicating their postoperative pain to a male physician
- Different working style and treatment decisions between female and male physicians
- Unconsciously incorporated role patterns and preconceptions
“Our potential solutions are recognition and training. We need a personalized style of medicine; we need to have a closer look. We owe our male and female patients as much,” said Dr. Späthling-Mestekemper.
This article was translated from the Medscape German Edition and a version appeared on Medscape.com.
LEIPZIG, GERMANY – Women eat more healthily, visit their physician more often, and accept offers of prophylactic treatment more frequently than their male counterparts. Nevertheless, they are generally diagnosed with a rheumatic disease much later. “With systemic sclerosis for example, diagnosis occurs a whole year later than for male patients,” said Uta Kiltz, MD, senior physician at the Ruhrgebiet Rheumatism Center in Bochum, Germany, at a press conference for the annual congress of the German Society for Rheumatology.
In addition, certain markers and antibodies can be detected earlier in men’s blood – for example in systemic sclerosis. “What’s more, women exhibit a more diverse array of symptoms, which can make an unequivocal diagnosis difficult,” Dr. Kiltz explained.
Differences between the sexes in terms of disease progression and clinical presentation have been described for most rheumatic diseases. Roughly speaking, women often exhibit a much wider range of symptoms and report a higher disease burden, whereas men tend to experience a more severe progression of the disease.
Comorbidities also occur at different rates between the sexes. Whereas women with rheumatoid arthritis suffer more frequently from osteoporosis and depression, men are more likely to develop cardiovascular diseases and diabetes.
Gender-sensitive approach
Like Dr. Kiltz, Susanna Späthling-Mestekemper, MD, PhD, of the Munich-Pasing (Germany) Rheumatology Practice, also advocates a gender-sensitive approach to diagnosis and therapy. Dr. Späthling-Mestekemper referred to this during the conference, stating that women are still treated more poorly than men. The difference in treatment quality results from gaps in knowledge in the following areas:
- Sex-specific differences in the diagnosis and therapy of rheumatic diseases and in basic and clinical research
- Sex-specific differences in communication between male and female patients and between male and female physicians.
Dr. Späthling-Mestekemper used axial spondyloarthritis (axSpA) as a “prominent example” of false diagnoses. “Men more commonly fulfill the modified New York criteria – involvement of the axial skeleton, the lumbar spine, and increasing radiological progression.”
In contrast, women with axSpA exhibit the following differences:
- It is more likely for the cervical spine to be affected.
- Women are more likely to suffer from peripheral joint involvement.
- They suffer more from whole body pain.
- They have fatigue and exhaustion.
- They exhibit fewer humoral signs of inflammation (lower C-reactive protein).
- They are rarely HLA-B27 positive.
“We also have to completely rethink how we make the diagnosis in women,” said Dr. Späthling-Mestekemper. The current approach leads to women with axSpA being diagnosed much later than men. “Depending on the study, the difference can range from 7 months to 2 years,” according to Dr. Späthling-Mestekemper.
A 2018 Spanish study reported that the most common incorrect diagnoses in women with axSpA were sciatica, osteoarthritis, and fibromyalgia.
However, it is not just in axSpA that there are significant differences between men and women. There is evidence that women with systemic lupus erythematosus suffer more from musculoskeletal symptoms, while men with lupus exhibit more severe organ involvement (especially more serositis and nephritis).
For systemic sclerosis, women have the higher survival rate. They also exhibit skin involvement more frequently. Men, however, are more likely to have organ involvement, especially with the lungs.
TNF blockers
Using the example of axSpA, Dr. Späthling-Mestekemper also showed that men and women respond differently to tumor necrosis factor (TNF) blocker therapy. “The duration of therapy with TNF blockers is shorter for women: 33.4 months versus 44.9 months. They respond less to this therapy; they stop and change more frequently.”
Data from March 2023 show that, in contrast, there is no evidence of a difference in response to Janus kinase inhibitor treatment.
The presence of enthesitis has been discussed as one reason for the worse response to TNF blockers in women, since they have it more often than men do. “In fact, a better response to TNF blockers is associated with HLA-B27 positivity, with the absence of enthesitis and with TNF blocker naivety. In women, higher fat-mass index could also play a part, or even abdominal weight gain, which also increases in women after menopause,” said Dr. Späthling-Mestekemper.
She mentioned the following other potential reasons for a delayed therapy response to biological drugs in women:
- Genetic, physical, or hormonal causes
- Widespread pain or fibromyalgia
- Late diagnosis or late application of therapy, which lowers the chances of remission.
Even the science itself has shown the following sex-specific shortcomings:
- Disregarding sex-specific differences in animal-experimental studies (which, until recently, were only conducted in male mice to avoid hormone fluctuations)
- Women in clinical studies are still underrepresented: only 37% of the populations in phase 3 studies are women; 64% of studies do not describe any sex-specific differences
- Most of the data come from epidemiological analyses (not from basic research)
- Gaps in medical textbooks
Communication differences
Female patients are looking for explanations, whereas male patients describe specific symptoms. Female physicians talk, while male physicians treat. They sound like stereotypes, but they have been substantiated in multiple studies, said Dr. Späthling-Mestekemper. In general, the study results show that male patients behave in the following ways:
- Describe their symptoms in terms of specifics
- Do not like to admit having mental health issues
- Are three to five times more likely to commit suicide because of depression than women
On the other hand, female patients behave in the following ways:
- Look for an explanation for their symptoms
- Often do not have their physical symptoms taken seriously
- Are often pushed in a psychosomatic direction.
Female physicians focus on the following questions:
- Prevention, communication, shared decision-making, open-ended questions, “positive” discussions, patient self-management (chronic diseases such as diabetes: female physicians are better at reaching the therapy goals set by the ADA guidelines than male physicians)
- Psychosocial situations: consultations last 1 minute longer (10%).
Male physicians focus on the following questions:
- Medical history
- Physical examination (cardiac catheterizations after a heart attack are arranged much more commonly by male rather than female physicians)
- Diagnostics
Recognition and training
A large-scale surgical study in 2021 made a few waves. The study analyzed whether it makes a difference if women are operated on by men or by women. The results showed that women who had been operated on by men exhibited a higher level of risk after the surgery, compared with men who had been operated on by men or by women. The risk took the following forms:
- 15% higher risk for a worse surgery result
- 16% higher risk for complications
- 11% higher risk for repeat hospitalization
- 20% higher risk for a longer period of hospitalization
- 32% higher risk for mortality
The study authors provided the following potential reasons for these differences:
- Male physicians underestimate the severity of symptoms in their female patients
- Women are less comfortable indicating their postoperative pain to a male physician
- Different working style and treatment decisions between female and male physicians
- Unconsciously incorporated role patterns and preconceptions
“Our potential solutions are recognition and training. We need a personalized style of medicine; we need to have a closer look. We owe our male and female patients as much,” said Dr. Späthling-Mestekemper.
This article was translated from the Medscape German Edition and a version appeared on Medscape.com.
AT THE GERMAN RHEUMATOLOGY CONGRESS 2023
New hyperglycemia emergency guidance updates DKA definition
HAMBURG, GERMANY – along with many other updates to the last statement on the topic, published 14 years ago.
Based on extensive literature reviews and observations of current trends, the new document – due to be published soon – will cover diagnosis and management of the two most serious acute hyperglycemic emergencies seen in adults, DKA and hyperosmolar hyperglycemic state (HHS).
New to the 2023 version will be a strong emphasis on the excess morbidity and mortality risks associated with the increasingly common “hybrid” presentation of the two conditions together, now seen in about a third of cases.
The new report will also more strongly urge clinicians to investigate why the person experienced the emergency.
While new-onset diabetes and infection are recognized precipitating causes for DKA, insulin omission related to finances, mental health, and social determinants should be identified, and patients directed to appropriate resources, said experts previewing the upcoming new report at the annual meeting of the European Association for the Study of Diabetes.
“The challenge is, although we were making progress for a long time in terms of those hyperglycemic crises, we’ve really plateaued and there are still people being admitted in large numbers, and when you look more globally even more so,” said American Diabetes Association Chief Science and Medical Officer Robert A. Gabbay, MD, PhD.
The new consensus report will be jointly endorsed by the ADA, the EASD, the American Association of Clinical Endocrinology, the Diabetes Technology Society, and the Joint British Diabetes Societies for Inpatient Care. The previous consensus statement on the subject was published in 2009 by the ADA alone.
New DKA and HHS definitions reflect emerging trends
The statement will revise the definition of DKA, partly spurred by the increasing occurrence and recognition of euglycemic ketoacidosis arising from the use of sodium-glucose cotransporter 2 (SGLT2) inhibitors. For all patients with hyperglycemic crisis, the hyperglycemia cutoff is now lowered to 200 mg/dL (11.1 mmol/L) from the previous 250 mg/dL.
However, the glucose cutoff has been removed entirely for people with a history of diabetes.
“Both of these changes are recognizing the wide range of glucose levels at the presence of DKA. Approximately 10% of DKA occurs with euglycemia or near-normoglycemia,” noted coauthor Shivani Misra, MD, PhD, senior clinical lecturer and honorary consultant in Metabolic Medicine at Imperial College, London.
For assessing ketosis in DKA, the new statement strongly recommends use of beta-hydroxybutyrate – either via point-of-care test or serum level measured in a laboratory – with a low cutoff of ≥ 3.0 mmol/L. Alternatively, a urine ketone strip value of 2+ or greater can be used.
However, beta-hydroxybutyrate testing is more widely available now than it was in 2009 and is strongly preferred over urine ketone measurement because it’s the predominant ketone during acidosis. Moreover, urine acetoacetate – measured by the strips – paradoxically increases during resolution of DKA, and drug interferences can occur with urine ketone measurement, Dr. Misra noted.
Metabolic acidosis is now defined as a pH < 7.3 and/or a bicarbonate concentration < 18 mmol/L, up from 15 in some prior guidelines including the United Kingdom’s. Also, anion gap has been removed from the main definition but, the document will say, can still be used in settings where ketone testing is unavailable.
As previously, the new statement will classify DKA by mild, moderate, and severe but now for the first time there are recommendations of care for each of those levels, as well as for HHS.
For HHS, the glucose cutoff of ≥ 600 mg/dL will stay the same. But now, the effective serum osmolality has been lowered from > 320 to > 300 mOsml/L to account for the effect of dehydration, along with an alternative criteria of total serum osmolality > 320 mOsm/L. The same two changes as with DKA for both ketones and acidosis have also been included for HHS.
Asked to comment, session audience member and independent diabetes industry consultant Charles Alexander, MD, told this news organization, “I liked the proposal to eliminate the anion gap in decision-making and to focus on measurement of blood ketones, principally beta-hydroxybutyrate, in the diagnosis of DKA and monitoring the effect of treatment.
“If someone is on an SGLT2 inhibitor, there is no need to look at blood glucose levels, which may be normal or near normal in the setting of DKA.”
But Dr. Alexander thinks that they should have eliminated glucose levels entirely as part of the DKA/HHS definition even for people without diabetes.
“The problem is that medical education for many years has taught us that DKA is a condition of high blood glucose, but it may not be. It is good that they said blood glucose levels were not important if the patient had a history of diabetes. However, a glucose of 200mg/dL may not be low enough if someone is on an SGLT2 inhibitor. There needs to be a much lower threshold for measuring blood ketones in anyone with nausea, vomiting, and abdominal pain, regardless of the blood glucose level.”
Acute management: IV fluids, insulin, and potassium
Like the 2009 statement, the new one will include detailed management flowcharts for DKA and HHS, but this time in color. This new statement includes individual algorithms for management with intravenous fluids, insulin, and potassium. Bicarbonate has been removed and relegated to a note at the bottom saying that it should only be considered if pH is < 7.0.
Under fluid treatment, the new statement offers more information about using crystalloids to treat dehydration and a recommendation to add dextrose to IV fluid therapy as a substrate when the glucose drops below 250 mg/dL, in order to prevent hypoglycemia. For euglycemic DKA, the recommendation is to include dextrose and normal saline simultaneously.
And for the first time, subcutaneous rather than IV insulin is considered acceptable for mild, but not moderate or severe, DKA.
Two options are suggested for IV insulin in HHS: The fluid can be given first and low-dose fixed-rate insulin infusion added, or fluids and insulin can be given at the same time.
Criteria for resolution of DKA are a venous pH of ≥ 7.3 or bicarbonate > 18 mmol/L, ketones < 0.6 mmol/L, and glucose ideally < 200 mg/dL (11.0 mmol/L). For HHS, resolution is suggested when the measured or calculated serum osmolality falls to < 300 mosm/kg, blood glucose is < 250mg/dL (13.9 mmol/L), urine output > 0.5 mL/kg/hour, and cognitive status is improved.
The statement also will provide detailed recommended options for transitioning from IV to subcutaneous insulin, but defers to clinical judgment for deciding when the patient can be discharged. The initiation or continuation of SGLT2 inhibitors is not recommended at any time during hospitalization for hyperglycemic crises.
Mitigating complications, preventing recurrence
In addition to listing potential complications of treating hyperglycemic crises, just as the 2009 statement did, the new one will offer mitigation strategies for some of the more common ones. For preventing hypoglycemia, frequent blood glucose monitoring is advised along with adding dextrose to the IV fluids when glucose drops below 250 mg/dL.
For prevention of hypokalemia, which occurs in about half of patients treated for DKA and HHS, the statement recommends potassium monitoring every 4 hours and replacement added to fluids.
Acute kidney injury, also occurring in about half of people treated for DKA and/or HHS, usually resolves with hydration. Daily renal function monitoring is advised.
Preventing recurrence: Many factors beyond clinical
Prevention of recurrence with readmission for DKA and/or HHS, occurring in up to 22% of U.S. patients within 30 days, entails close follow-up within 2-4 weeks after discharge (including via telemedicine), and assessment of possible causes, including mental health disorders and social determinants of health.
Appropriate education should be provided, including “structured education” involving problem-solving, sick day rules, injection techniques, a review of insulin doses, consideration of continuous glucose monitoring (CGM), and home ketone testing.
Patients should be provided with an adequate supply of insulin and durable diabetes equipment, along with contact information for health care professionals who can assist them. Social service professionals can be helpful for patients who lack reliable access.
Dr. Gabbay told this news organization, “The eye-opening thing is we tend to typically think of DKA as how people tend to get diagnosed with diabetes and, yes, that’s true, but that’s only a minority of people. Those might be preventable by early screening, but all these other people and the number of recurrent episodes, that’s an area where it’s really a failure of the system where we can do better in ensuring that doesn’t happen.”
Education is only part of it, he stressed. “It’s not just an intelligence thing. It’s social factors, and there can be complex psychological issues and mental health issues. We need to screen for those things when we see someone coming back the second, third, fifth, or sixth time. We’ve all seen that. Just educating them to take their insulin is not the answer. …You’ve got to ask the questions and engage them to go a little deeper.”
Dr. Gabbay is an employee of the ADA. Dr. Alexander has reported being a nonpaid advisor for diaTribe and a consultant for Kinexum. Dr. Misra has received speaker fees from Sanofi and ABCD and an investigator-initiated research grant from Dexcom, and is a trustee for the Diabetes Research and Wellness Foundation in the United Kingdom.
A version of this article appeared on Medscape.com.
HAMBURG, GERMANY – along with many other updates to the last statement on the topic, published 14 years ago.
Based on extensive literature reviews and observations of current trends, the new document – due to be published soon – will cover diagnosis and management of the two most serious acute hyperglycemic emergencies seen in adults, DKA and hyperosmolar hyperglycemic state (HHS).
New to the 2023 version will be a strong emphasis on the excess morbidity and mortality risks associated with the increasingly common “hybrid” presentation of the two conditions together, now seen in about a third of cases.
The new report will also more strongly urge clinicians to investigate why the person experienced the emergency.
While new-onset diabetes and infection are recognized precipitating causes for DKA, insulin omission related to finances, mental health, and social determinants should be identified, and patients directed to appropriate resources, said experts previewing the upcoming new report at the annual meeting of the European Association for the Study of Diabetes.
“The challenge is, although we were making progress for a long time in terms of those hyperglycemic crises, we’ve really plateaued and there are still people being admitted in large numbers, and when you look more globally even more so,” said American Diabetes Association Chief Science and Medical Officer Robert A. Gabbay, MD, PhD.
The new consensus report will be jointly endorsed by the ADA, the EASD, the American Association of Clinical Endocrinology, the Diabetes Technology Society, and the Joint British Diabetes Societies for Inpatient Care. The previous consensus statement on the subject was published in 2009 by the ADA alone.
New DKA and HHS definitions reflect emerging trends
The statement will revise the definition of DKA, partly spurred by the increasing occurrence and recognition of euglycemic ketoacidosis arising from the use of sodium-glucose cotransporter 2 (SGLT2) inhibitors. For all patients with hyperglycemic crisis, the hyperglycemia cutoff is now lowered to 200 mg/dL (11.1 mmol/L) from the previous 250 mg/dL.
However, the glucose cutoff has been removed entirely for people with a history of diabetes.
“Both of these changes are recognizing the wide range of glucose levels at the presence of DKA. Approximately 10% of DKA occurs with euglycemia or near-normoglycemia,” noted coauthor Shivani Misra, MD, PhD, senior clinical lecturer and honorary consultant in Metabolic Medicine at Imperial College, London.
For assessing ketosis in DKA, the new statement strongly recommends use of beta-hydroxybutyrate – either via point-of-care test or serum level measured in a laboratory – with a low cutoff of ≥ 3.0 mmol/L. Alternatively, a urine ketone strip value of 2+ or greater can be used.
However, beta-hydroxybutyrate testing is more widely available now than it was in 2009 and is strongly preferred over urine ketone measurement because it’s the predominant ketone during acidosis. Moreover, urine acetoacetate – measured by the strips – paradoxically increases during resolution of DKA, and drug interferences can occur with urine ketone measurement, Dr. Misra noted.
Metabolic acidosis is now defined as a pH < 7.3 and/or a bicarbonate concentration < 18 mmol/L, up from 15 in some prior guidelines including the United Kingdom’s. Also, anion gap has been removed from the main definition but, the document will say, can still be used in settings where ketone testing is unavailable.
As previously, the new statement will classify DKA by mild, moderate, and severe but now for the first time there are recommendations of care for each of those levels, as well as for HHS.
For HHS, the glucose cutoff of ≥ 600 mg/dL will stay the same. But now, the effective serum osmolality has been lowered from > 320 to > 300 mOsml/L to account for the effect of dehydration, along with an alternative criteria of total serum osmolality > 320 mOsm/L. The same two changes as with DKA for both ketones and acidosis have also been included for HHS.
Asked to comment, session audience member and independent diabetes industry consultant Charles Alexander, MD, told this news organization, “I liked the proposal to eliminate the anion gap in decision-making and to focus on measurement of blood ketones, principally beta-hydroxybutyrate, in the diagnosis of DKA and monitoring the effect of treatment.
“If someone is on an SGLT2 inhibitor, there is no need to look at blood glucose levels, which may be normal or near normal in the setting of DKA.”
But Dr. Alexander thinks that they should have eliminated glucose levels entirely as part of the DKA/HHS definition even for people without diabetes.
“The problem is that medical education for many years has taught us that DKA is a condition of high blood glucose, but it may not be. It is good that they said blood glucose levels were not important if the patient had a history of diabetes. However, a glucose of 200mg/dL may not be low enough if someone is on an SGLT2 inhibitor. There needs to be a much lower threshold for measuring blood ketones in anyone with nausea, vomiting, and abdominal pain, regardless of the blood glucose level.”
Acute management: IV fluids, insulin, and potassium
Like the 2009 statement, the new one will include detailed management flowcharts for DKA and HHS, but this time in color. This new statement includes individual algorithms for management with intravenous fluids, insulin, and potassium. Bicarbonate has been removed and relegated to a note at the bottom saying that it should only be considered if pH is < 7.0.
Under fluid treatment, the new statement offers more information about using crystalloids to treat dehydration and a recommendation to add dextrose to IV fluid therapy as a substrate when the glucose drops below 250 mg/dL, in order to prevent hypoglycemia. For euglycemic DKA, the recommendation is to include dextrose and normal saline simultaneously.
And for the first time, subcutaneous rather than IV insulin is considered acceptable for mild, but not moderate or severe, DKA.
Two options are suggested for IV insulin in HHS: The fluid can be given first and low-dose fixed-rate insulin infusion added, or fluids and insulin can be given at the same time.
Criteria for resolution of DKA are a venous pH of ≥ 7.3 or bicarbonate > 18 mmol/L, ketones < 0.6 mmol/L, and glucose ideally < 200 mg/dL (11.0 mmol/L). For HHS, resolution is suggested when the measured or calculated serum osmolality falls to < 300 mosm/kg, blood glucose is < 250mg/dL (13.9 mmol/L), urine output > 0.5 mL/kg/hour, and cognitive status is improved.
The statement also will provide detailed recommended options for transitioning from IV to subcutaneous insulin, but defers to clinical judgment for deciding when the patient can be discharged. The initiation or continuation of SGLT2 inhibitors is not recommended at any time during hospitalization for hyperglycemic crises.
Mitigating complications, preventing recurrence
In addition to listing potential complications of treating hyperglycemic crises, just as the 2009 statement did, the new one will offer mitigation strategies for some of the more common ones. For preventing hypoglycemia, frequent blood glucose monitoring is advised along with adding dextrose to the IV fluids when glucose drops below 250 mg/dL.
For prevention of hypokalemia, which occurs in about half of patients treated for DKA and HHS, the statement recommends potassium monitoring every 4 hours and replacement added to fluids.
Acute kidney injury, also occurring in about half of people treated for DKA and/or HHS, usually resolves with hydration. Daily renal function monitoring is advised.
Preventing recurrence: Many factors beyond clinical
Prevention of recurrence with readmission for DKA and/or HHS, occurring in up to 22% of U.S. patients within 30 days, entails close follow-up within 2-4 weeks after discharge (including via telemedicine), and assessment of possible causes, including mental health disorders and social determinants of health.
Appropriate education should be provided, including “structured education” involving problem-solving, sick day rules, injection techniques, a review of insulin doses, consideration of continuous glucose monitoring (CGM), and home ketone testing.
Patients should be provided with an adequate supply of insulin and durable diabetes equipment, along with contact information for health care professionals who can assist them. Social service professionals can be helpful for patients who lack reliable access.
Dr. Gabbay told this news organization, “The eye-opening thing is we tend to typically think of DKA as how people tend to get diagnosed with diabetes and, yes, that’s true, but that’s only a minority of people. Those might be preventable by early screening, but all these other people and the number of recurrent episodes, that’s an area where it’s really a failure of the system where we can do better in ensuring that doesn’t happen.”
Education is only part of it, he stressed. “It’s not just an intelligence thing. It’s social factors, and there can be complex psychological issues and mental health issues. We need to screen for those things when we see someone coming back the second, third, fifth, or sixth time. We’ve all seen that. Just educating them to take their insulin is not the answer. …You’ve got to ask the questions and engage them to go a little deeper.”
Dr. Gabbay is an employee of the ADA. Dr. Alexander has reported being a nonpaid advisor for diaTribe and a consultant for Kinexum. Dr. Misra has received speaker fees from Sanofi and ABCD and an investigator-initiated research grant from Dexcom, and is a trustee for the Diabetes Research and Wellness Foundation in the United Kingdom.
A version of this article appeared on Medscape.com.
HAMBURG, GERMANY – along with many other updates to the last statement on the topic, published 14 years ago.
Based on extensive literature reviews and observations of current trends, the new document – due to be published soon – will cover diagnosis and management of the two most serious acute hyperglycemic emergencies seen in adults, DKA and hyperosmolar hyperglycemic state (HHS).
New to the 2023 version will be a strong emphasis on the excess morbidity and mortality risks associated with the increasingly common “hybrid” presentation of the two conditions together, now seen in about a third of cases.
The new report will also more strongly urge clinicians to investigate why the person experienced the emergency.
While new-onset diabetes and infection are recognized precipitating causes for DKA, insulin omission related to finances, mental health, and social determinants should be identified, and patients directed to appropriate resources, said experts previewing the upcoming new report at the annual meeting of the European Association for the Study of Diabetes.
“The challenge is, although we were making progress for a long time in terms of those hyperglycemic crises, we’ve really plateaued and there are still people being admitted in large numbers, and when you look more globally even more so,” said American Diabetes Association Chief Science and Medical Officer Robert A. Gabbay, MD, PhD.
The new consensus report will be jointly endorsed by the ADA, the EASD, the American Association of Clinical Endocrinology, the Diabetes Technology Society, and the Joint British Diabetes Societies for Inpatient Care. The previous consensus statement on the subject was published in 2009 by the ADA alone.
New DKA and HHS definitions reflect emerging trends
The statement will revise the definition of DKA, partly spurred by the increasing occurrence and recognition of euglycemic ketoacidosis arising from the use of sodium-glucose cotransporter 2 (SGLT2) inhibitors. For all patients with hyperglycemic crisis, the hyperglycemia cutoff is now lowered to 200 mg/dL (11.1 mmol/L) from the previous 250 mg/dL.
However, the glucose cutoff has been removed entirely for people with a history of diabetes.
“Both of these changes are recognizing the wide range of glucose levels at the presence of DKA. Approximately 10% of DKA occurs with euglycemia or near-normoglycemia,” noted coauthor Shivani Misra, MD, PhD, senior clinical lecturer and honorary consultant in Metabolic Medicine at Imperial College, London.
For assessing ketosis in DKA, the new statement strongly recommends use of beta-hydroxybutyrate – either via point-of-care test or serum level measured in a laboratory – with a low cutoff of ≥ 3.0 mmol/L. Alternatively, a urine ketone strip value of 2+ or greater can be used.
However, beta-hydroxybutyrate testing is more widely available now than it was in 2009 and is strongly preferred over urine ketone measurement because it’s the predominant ketone during acidosis. Moreover, urine acetoacetate – measured by the strips – paradoxically increases during resolution of DKA, and drug interferences can occur with urine ketone measurement, Dr. Misra noted.
Metabolic acidosis is now defined as a pH < 7.3 and/or a bicarbonate concentration < 18 mmol/L, up from 15 in some prior guidelines including the United Kingdom’s. Also, anion gap has been removed from the main definition but, the document will say, can still be used in settings where ketone testing is unavailable.
As previously, the new statement will classify DKA by mild, moderate, and severe but now for the first time there are recommendations of care for each of those levels, as well as for HHS.
For HHS, the glucose cutoff of ≥ 600 mg/dL will stay the same. But now, the effective serum osmolality has been lowered from > 320 to > 300 mOsml/L to account for the effect of dehydration, along with an alternative criteria of total serum osmolality > 320 mOsm/L. The same two changes as with DKA for both ketones and acidosis have also been included for HHS.
Asked to comment, session audience member and independent diabetes industry consultant Charles Alexander, MD, told this news organization, “I liked the proposal to eliminate the anion gap in decision-making and to focus on measurement of blood ketones, principally beta-hydroxybutyrate, in the diagnosis of DKA and monitoring the effect of treatment.
“If someone is on an SGLT2 inhibitor, there is no need to look at blood glucose levels, which may be normal or near normal in the setting of DKA.”
But Dr. Alexander thinks that they should have eliminated glucose levels entirely as part of the DKA/HHS definition even for people without diabetes.
“The problem is that medical education for many years has taught us that DKA is a condition of high blood glucose, but it may not be. It is good that they said blood glucose levels were not important if the patient had a history of diabetes. However, a glucose of 200mg/dL may not be low enough if someone is on an SGLT2 inhibitor. There needs to be a much lower threshold for measuring blood ketones in anyone with nausea, vomiting, and abdominal pain, regardless of the blood glucose level.”
Acute management: IV fluids, insulin, and potassium
Like the 2009 statement, the new one will include detailed management flowcharts for DKA and HHS, but this time in color. This new statement includes individual algorithms for management with intravenous fluids, insulin, and potassium. Bicarbonate has been removed and relegated to a note at the bottom saying that it should only be considered if pH is < 7.0.
Under fluid treatment, the new statement offers more information about using crystalloids to treat dehydration and a recommendation to add dextrose to IV fluid therapy as a substrate when the glucose drops below 250 mg/dL, in order to prevent hypoglycemia. For euglycemic DKA, the recommendation is to include dextrose and normal saline simultaneously.
And for the first time, subcutaneous rather than IV insulin is considered acceptable for mild, but not moderate or severe, DKA.
Two options are suggested for IV insulin in HHS: The fluid can be given first and low-dose fixed-rate insulin infusion added, or fluids and insulin can be given at the same time.
Criteria for resolution of DKA are a venous pH of ≥ 7.3 or bicarbonate > 18 mmol/L, ketones < 0.6 mmol/L, and glucose ideally < 200 mg/dL (11.0 mmol/L). For HHS, resolution is suggested when the measured or calculated serum osmolality falls to < 300 mosm/kg, blood glucose is < 250mg/dL (13.9 mmol/L), urine output > 0.5 mL/kg/hour, and cognitive status is improved.
The statement also will provide detailed recommended options for transitioning from IV to subcutaneous insulin, but defers to clinical judgment for deciding when the patient can be discharged. The initiation or continuation of SGLT2 inhibitors is not recommended at any time during hospitalization for hyperglycemic crises.
Mitigating complications, preventing recurrence
In addition to listing potential complications of treating hyperglycemic crises, just as the 2009 statement did, the new one will offer mitigation strategies for some of the more common ones. For preventing hypoglycemia, frequent blood glucose monitoring is advised along with adding dextrose to the IV fluids when glucose drops below 250 mg/dL.
For prevention of hypokalemia, which occurs in about half of patients treated for DKA and HHS, the statement recommends potassium monitoring every 4 hours and replacement added to fluids.
Acute kidney injury, also occurring in about half of people treated for DKA and/or HHS, usually resolves with hydration. Daily renal function monitoring is advised.
Preventing recurrence: Many factors beyond clinical
Prevention of recurrence with readmission for DKA and/or HHS, occurring in up to 22% of U.S. patients within 30 days, entails close follow-up within 2-4 weeks after discharge (including via telemedicine), and assessment of possible causes, including mental health disorders and social determinants of health.
Appropriate education should be provided, including “structured education” involving problem-solving, sick day rules, injection techniques, a review of insulin doses, consideration of continuous glucose monitoring (CGM), and home ketone testing.
Patients should be provided with an adequate supply of insulin and durable diabetes equipment, along with contact information for health care professionals who can assist them. Social service professionals can be helpful for patients who lack reliable access.
Dr. Gabbay told this news organization, “The eye-opening thing is we tend to typically think of DKA as how people tend to get diagnosed with diabetes and, yes, that’s true, but that’s only a minority of people. Those might be preventable by early screening, but all these other people and the number of recurrent episodes, that’s an area where it’s really a failure of the system where we can do better in ensuring that doesn’t happen.”
Education is only part of it, he stressed. “It’s not just an intelligence thing. It’s social factors, and there can be complex psychological issues and mental health issues. We need to screen for those things when we see someone coming back the second, third, fifth, or sixth time. We’ve all seen that. Just educating them to take their insulin is not the answer. …You’ve got to ask the questions and engage them to go a little deeper.”
Dr. Gabbay is an employee of the ADA. Dr. Alexander has reported being a nonpaid advisor for diaTribe and a consultant for Kinexum. Dr. Misra has received speaker fees from Sanofi and ABCD and an investigator-initiated research grant from Dexcom, and is a trustee for the Diabetes Research and Wellness Foundation in the United Kingdom.
A version of this article appeared on Medscape.com.
AT EASD 2023
Spreading out daily meals and snacks may boost heart failure survival
CLEVELAND – , an observational study suggests.
The new findings, based primarily on 15 years of data from the National Health and Nutrition Examination Survey (NHANES), may argue against time-restricted diet interventions like intermittent fasting for patients with HF, researchers say.
The study’s nearly 1,000 participants on medical therapy for HF reported a mean daily eating window of 11 hours and daily average of four “eating occasions,” defined as meals or snacks of at least 50 kcal.
A daily eating window of 11 or more hours, compared with less than 11 hours, corresponded to a greater than 40% drop in risk for CV mortality (P = .013) over 5-6 years, reported Hayley E. Billingsley, RD, CEP, Virginia Commonwealth University, Richmond, Va,, at the annual scientific meeting of the Heart Failure Society of America.
The analysis adjusted for caloric intake, daily number of eating occasions, body mass index (BMI), history of CV disease and cancer, diabetes, and a slew of other potential confounders.
Prior evidence, mostly from healthy people, has suggested that extended fasting during the day is associated with less physical activity, Ms. Billingsley said in an interview. So it may be that people with HF who spread out their calorie intake are more active throughout the day.
A longer time window for eating, therefore, may have indirect metabolic benefits and help preserve their lean body mass, possibly reducing CV risk in a patient group at risk for muscle wasting.
The findings add to earlier evidence from Ms. Billingsley’s center that suggests that expanded daily time windows for eating, especially later final food rather than earlier first food, may help boost CV fitness for patients with obesity and HF with preserved ejection fraction.
Intermittent fasting and other practices involving the timing of food intake have been studied for weight loss and metabolic health in mostly healthy people and patients with diabetes, she noted. “But it’s really underexplored in people with established cardiovascular disease.”
On the basis of admittedly “very preliminary” findings, it may be that some patients should not shorten their daily time windows for eating or engage in intermittent fasting, Ms. Billingsley said. It’s probably worth considering, before the approach is recommended, “what their risk is for malnutrition or sarcopenia.”
The current study included 991 persons who entered the NHANES database from 2003 to 2018. The patients self-identified as having HF, reported taking medications commonly prescribed in HF, and provided at least two “reliable” dietary recalls.
The average age of the patients was 68 years, and they had had HF for a mean of 9.5 years; 47% were women, three-fourths were White persons, two thirds had dyslipidemia, and a quarter had a history of cancer.
On average, their first eating occasion of the day was at about 8:30 a.m., and the last occasion was at about 7:30 p.m., for a time window of about 11 hours; daily calorie consumption averaged about 1,830 kcal.
About 52% died over the mean follow-up of 69 months; about 44% of deaths were from CV causes.
In a model adjusted for demographics, BMI, smoking status, times of eating occasions, CV disease, diabetes, and cancer history, the all-cause mortality hazard ratio for time windows ≥ 11 hours vs. < 11 hours was 0.236 (95% confidence interval, 0.07-0.715; P = .011).
The reduction was no longer significant on further adjustment for duration of HF, a score reflecting difficulty walking, nightly hours of sleep (which averaged 7.2 hours), daily number of eating occasions, and caloric intake, Ms. Billingsley reported.
But in the fully adjusted analysis, the HR for CV mortality for the longer vs. shorter time window was 0.368 (95% CI, 0.169-0.803; P = .013).
The issue deserves further exploration in a randomized trial, Ms. Billingsley proposed, perhaps one in which patients with HF wear accelerometers to track daily activity levels. “We’d love to do a pilot study of extending their eating window that really digs into what the mechanism of any benefit might be if we assign them to a longer time window and whether it’s related to physical activity.”
Ms. Billingsley reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
CLEVELAND – , an observational study suggests.
The new findings, based primarily on 15 years of data from the National Health and Nutrition Examination Survey (NHANES), may argue against time-restricted diet interventions like intermittent fasting for patients with HF, researchers say.
The study’s nearly 1,000 participants on medical therapy for HF reported a mean daily eating window of 11 hours and daily average of four “eating occasions,” defined as meals or snacks of at least 50 kcal.
A daily eating window of 11 or more hours, compared with less than 11 hours, corresponded to a greater than 40% drop in risk for CV mortality (P = .013) over 5-6 years, reported Hayley E. Billingsley, RD, CEP, Virginia Commonwealth University, Richmond, Va,, at the annual scientific meeting of the Heart Failure Society of America.
The analysis adjusted for caloric intake, daily number of eating occasions, body mass index (BMI), history of CV disease and cancer, diabetes, and a slew of other potential confounders.
Prior evidence, mostly from healthy people, has suggested that extended fasting during the day is associated with less physical activity, Ms. Billingsley said in an interview. So it may be that people with HF who spread out their calorie intake are more active throughout the day.
A longer time window for eating, therefore, may have indirect metabolic benefits and help preserve their lean body mass, possibly reducing CV risk in a patient group at risk for muscle wasting.
The findings add to earlier evidence from Ms. Billingsley’s center that suggests that expanded daily time windows for eating, especially later final food rather than earlier first food, may help boost CV fitness for patients with obesity and HF with preserved ejection fraction.
Intermittent fasting and other practices involving the timing of food intake have been studied for weight loss and metabolic health in mostly healthy people and patients with diabetes, she noted. “But it’s really underexplored in people with established cardiovascular disease.”
On the basis of admittedly “very preliminary” findings, it may be that some patients should not shorten their daily time windows for eating or engage in intermittent fasting, Ms. Billingsley said. It’s probably worth considering, before the approach is recommended, “what their risk is for malnutrition or sarcopenia.”
The current study included 991 persons who entered the NHANES database from 2003 to 2018. The patients self-identified as having HF, reported taking medications commonly prescribed in HF, and provided at least two “reliable” dietary recalls.
The average age of the patients was 68 years, and they had had HF for a mean of 9.5 years; 47% were women, three-fourths were White persons, two thirds had dyslipidemia, and a quarter had a history of cancer.
On average, their first eating occasion of the day was at about 8:30 a.m., and the last occasion was at about 7:30 p.m., for a time window of about 11 hours; daily calorie consumption averaged about 1,830 kcal.
About 52% died over the mean follow-up of 69 months; about 44% of deaths were from CV causes.
In a model adjusted for demographics, BMI, smoking status, times of eating occasions, CV disease, diabetes, and cancer history, the all-cause mortality hazard ratio for time windows ≥ 11 hours vs. < 11 hours was 0.236 (95% confidence interval, 0.07-0.715; P = .011).
The reduction was no longer significant on further adjustment for duration of HF, a score reflecting difficulty walking, nightly hours of sleep (which averaged 7.2 hours), daily number of eating occasions, and caloric intake, Ms. Billingsley reported.
But in the fully adjusted analysis, the HR for CV mortality for the longer vs. shorter time window was 0.368 (95% CI, 0.169-0.803; P = .013).
The issue deserves further exploration in a randomized trial, Ms. Billingsley proposed, perhaps one in which patients with HF wear accelerometers to track daily activity levels. “We’d love to do a pilot study of extending their eating window that really digs into what the mechanism of any benefit might be if we assign them to a longer time window and whether it’s related to physical activity.”
Ms. Billingsley reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
CLEVELAND – , an observational study suggests.
The new findings, based primarily on 15 years of data from the National Health and Nutrition Examination Survey (NHANES), may argue against time-restricted diet interventions like intermittent fasting for patients with HF, researchers say.
The study’s nearly 1,000 participants on medical therapy for HF reported a mean daily eating window of 11 hours and daily average of four “eating occasions,” defined as meals or snacks of at least 50 kcal.
A daily eating window of 11 or more hours, compared with less than 11 hours, corresponded to a greater than 40% drop in risk for CV mortality (P = .013) over 5-6 years, reported Hayley E. Billingsley, RD, CEP, Virginia Commonwealth University, Richmond, Va,, at the annual scientific meeting of the Heart Failure Society of America.
The analysis adjusted for caloric intake, daily number of eating occasions, body mass index (BMI), history of CV disease and cancer, diabetes, and a slew of other potential confounders.
Prior evidence, mostly from healthy people, has suggested that extended fasting during the day is associated with less physical activity, Ms. Billingsley said in an interview. So it may be that people with HF who spread out their calorie intake are more active throughout the day.
A longer time window for eating, therefore, may have indirect metabolic benefits and help preserve their lean body mass, possibly reducing CV risk in a patient group at risk for muscle wasting.
The findings add to earlier evidence from Ms. Billingsley’s center that suggests that expanded daily time windows for eating, especially later final food rather than earlier first food, may help boost CV fitness for patients with obesity and HF with preserved ejection fraction.
Intermittent fasting and other practices involving the timing of food intake have been studied for weight loss and metabolic health in mostly healthy people and patients with diabetes, she noted. “But it’s really underexplored in people with established cardiovascular disease.”
On the basis of admittedly “very preliminary” findings, it may be that some patients should not shorten their daily time windows for eating or engage in intermittent fasting, Ms. Billingsley said. It’s probably worth considering, before the approach is recommended, “what their risk is for malnutrition or sarcopenia.”
The current study included 991 persons who entered the NHANES database from 2003 to 2018. The patients self-identified as having HF, reported taking medications commonly prescribed in HF, and provided at least two “reliable” dietary recalls.
The average age of the patients was 68 years, and they had had HF for a mean of 9.5 years; 47% were women, three-fourths were White persons, two thirds had dyslipidemia, and a quarter had a history of cancer.
On average, their first eating occasion of the day was at about 8:30 a.m., and the last occasion was at about 7:30 p.m., for a time window of about 11 hours; daily calorie consumption averaged about 1,830 kcal.
About 52% died over the mean follow-up of 69 months; about 44% of deaths were from CV causes.
In a model adjusted for demographics, BMI, smoking status, times of eating occasions, CV disease, diabetes, and cancer history, the all-cause mortality hazard ratio for time windows ≥ 11 hours vs. < 11 hours was 0.236 (95% confidence interval, 0.07-0.715; P = .011).
The reduction was no longer significant on further adjustment for duration of HF, a score reflecting difficulty walking, nightly hours of sleep (which averaged 7.2 hours), daily number of eating occasions, and caloric intake, Ms. Billingsley reported.
But in the fully adjusted analysis, the HR for CV mortality for the longer vs. shorter time window was 0.368 (95% CI, 0.169-0.803; P = .013).
The issue deserves further exploration in a randomized trial, Ms. Billingsley proposed, perhaps one in which patients with HF wear accelerometers to track daily activity levels. “We’d love to do a pilot study of extending their eating window that really digs into what the mechanism of any benefit might be if we assign them to a longer time window and whether it’s related to physical activity.”
Ms. Billingsley reported no relevant financial relationships.
A version of this article appeared on Medscape.com.
AT HFSA 2023
Dietary changes to microbiome may improve lung function
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
HONOLULU – , and the days immediately following the 9/11 attacks.
Among NYC firefighters enrolled in the randomized FIREHOUSE (Food Intake Restriction for Health Outcome Support and Education) study who took part in a microbiome substudy, those who followed a low-calorie, Mediterranean-style diet had higher levels in stools samples at 6 months of Bacteroides ovatus, a bacterial species associated with protection against bowel inflammation.
In contrast, participants who followed a usual-care diet had elevated 6-month levels of a species associated with high-fat diets and inflammation, reported Rachel Lam, a predoctoral fellow in the Nolan Lab at NYU Langone Medical Center, at the annual meeting of the American College of Chest Physicians (CHEST).
“Overall, we found that in our validation cohort, Bacteroides ovatus was increased in the LoCalMed arm after 6 months, and this bacterial species is associated with fewer negative health effects,” she said.
Ms. Lam noted that in a murine model of high-fat diets, mice gavaged with Bacteroides ovatus had reductions in body mass index and decreased serum LDL cholesterol and triglyceride levels.
FIREHOUSE cohort
Senior author Anna Nolan, MD, whose lab members study predictors of lung function loss in a cohort of firefighters who were exposed to the particulate matter clouding the air of lower Manhattan on 9/11 and the ensuing days, told this news organization that the findings, while preliminary, support previous research findings on potential links between intestinal microbiota and lung function.
“It’s interesting that we saw this done in other models, like mouse models and such, where certain bacteria were viewed as healthy for the system, and if they were able to bring that bacteria out in larger amounts they saw anti-inflammatory effects, so we’re hoping to mirror that and also do a mouse model,” she said.
Dr. Nolan’s group has previously shown that markers for the metabolic syndrome, inflammation, and vascular injury detected in serum samples taken within 6 months of 9/11 were predictive for later abnormal lung function. In addition, their group has found that elevated serum levels of an LDL metabolite after intense World Trade Center dust exposure is a risk factor for future impaired lung function as measured by forced expiratory volume in 1 second (FEV1).
In the FIREHOUSE trial, 89 patients were randomly assigned either to a technology-supported educational and behavioral intervention targeting calorie restriction for weight loss while following a low-calorie Mediterranean diet, or to usual care. The usual-care arm included participants who were informed about their weight, BMI, and other standard measures at annual visits and were given general advice about healthy eating, but were not assigned to a specific diet.
Participants in the LoCalMed group had significant decreases in BMI and increases in FEV1, compared with those in the usual-care group. In addition, the LoCalMed group had improved vascular health, better dietary habits, decreases in fats and calories from sweets, and decreases in inflammation as measured by a lower white blood cell count.
Microbiome substudy
At CHEST 2023, Ms. Lam reported on microbiome pilot and validation substudies of FIREHOUSE.
The pilot study included five patients in each arm. The validation sample included 15 participants in the Mediterranean diet group and 16 in the usual-care diet group.
Each participant’s microbiome was assessed with genomic sequencing with sequences aligned to a bacterial database. The number and diversity of bacterial species in each sample were determined with the Chao1 Index and Shannon Index, respectively.
There were no significant differences among the study groups in mean age, exposure at the World Trade Center site, or years of service.
Although bacterial diversity did not differ between the study arms either at baseline or at 6 months, in both groups it significantly decreased over time (P = .02 in the pilot, P < .0001 in the validation arm).
In the pilot study, there was an increase over 6 months in the usual care arm only of Bilophila wadsworthia, a species associated with high-fat diets and inflammation.
In the validation study, patients in the LoCalMed arm had significant reductions in Ruminococcaceae (P = .015) and increases in both Bacteroides ovatus (P = .03) and Alistipes shahii (P = .038), a recently identified species with uncertain protective or pathogenic potential.
In contrast, there were no significant increases in species in the usual-care group, but there were significant declines in several other bacterial species; Ms.Lam, however, did not say whether these changes had clinical significance. “Future studies will assess microbial association with clinical outcomes,” Ms. Lam said.
Confounding factors
Samuel Evans, MD, a pulmonologist at Straub Medical Center in Honolulu who moderated the oral abstract session where the data were presented, commented that the data are interesting but added that associations are difficult to determine given the heterogeneity of exposures that firefighters encounter.
“I think it’s interesting that clearly diet is influencing the type of bacteria in the biome in the gut, and perhaps some are favorable, and some are not favorable,” he told this news organization “We already know that the Mediterranean diet is associated with better health outcomes, so it makes sense, but can we tease out in the microbiome which bacteria are harmful and which are helpful.”
He noted that there are a lot of confounding factors and that “it’s hard to find the right signal when you have so many variables.”
The FIREHOUSE study is supported by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety & Health and the National Heart, Lung, and Blood Institute. Ms. Lam, Dr. Nolan, and Dr. Evans report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT CHEST 2023
Semaglutide win in HFpEF with obesity regardless of ejection fraction: STEP-HFpEF
CLEVELAND – independently of baseline left-ventricular ejection fraction (LVEF).
The finding comes from a prespecified secondary analysis of the STEP-HFpEF trial of more than 500 nondiabetic patients with obesity and HF with an initial LVEF of 45% or greater.
They suggest that for patients with the obesity phenotype of HFpEF, semaglutide (Wegovy) could potentially join SGLT2 inhibitors on the short list of meds with consistent treatment effects whether LVEF is mildly reduced, preserved, or in the normal range.
That would distinguish the drug, a glucagon-like peptide-1 (GLP-1) receptor agonist, from mineralocorticoid receptor antagonists (MRA), sacubitril-valsartan (Entresto), and other renin-angiotensin-system inhibitors (RASi), whose benefits tend to taper off with rising LVEF.
The patients assigned to semaglutide showed significant improvement in both primary endpoints – change in Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS) and change in body weight at 52 weeks – whether their baseline LVEF was 45%-49%, 50%-59%, or 60% or greater.
Results were similar for improvements in 6-minute walk distance (6MWD) and levels of NT-terminal pro–brain natriuretic peptide (NT-proBNP) and C-reactive protein, observed Javed Butler, MD, when presenting the analysis at the annual meeting of the Heart Failure Society of America, Cleveland.
Dr. Butler, of Baylor Scott and White Research Institute, Dallas, and the University of Mississippi, Jackson, is also lead author of the study, which was published on the same day in the Journal of the American College of Cardiology.
In his presentation, Dr. Butler singled out the NT-proBNP finding as “very meaningful” with respect to understanding potential mechanisms of the drug effects observed in the trial.
For example, people with obesity tend to have lower than average natriuretic peptide levels that “actually go up a bit” when they lose weight, he observed. But in the trial, “we saw a reduction in NT-proBNP in spite of the weight loss,” regardless of LVEF category.
John McMurray, MD, University of Glasgow, the invited discussant for Dr. Butler’s presentation, agreed that it raises the question whether weight loss was the sole semaglutide effect responsible for the improvement in heart failure status and biomarkers. The accompanying NT-proBNP reductions – when the opposite might otherwise have been expected – may point to a possible mechanism of action that is “something more than just weight loss,” he said. “If that were the case, it becomes very important, because it means that this treatment might do good things in non-obese patients or might do good things in patients with other types of heart failure.”
‘Vital reassurance’
More definitive trials are needed “to clarify safety and efficacy of obesity-targeted therapeutics in HF across the ejection fraction spectrum,” according to an accompanying editorial).
Still, the STEP-HFpEF analysis “strengthens the role of GLP-1 [receptor agonists] to ameliorate health status” for patients with obesity and HF with mildly reduced or preserved ejection fraction, write Muthiah Vaduganathan, MD, MPH, and John W. Ostrominski, MD, Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Its findings “provide vital reassurance” on semaglutide safety and efficacy in HF with below-normal LVEF and “tentatively support the existence of a more general, LVEF-independent, obesity-related HF phenotype capable of favorable modification with incretin-based therapies.”
The lack of heterogeneity in treatment effects across LVEF subgroups “is not surprising,” but “the findings reinforce that the benefits of this therapy in those meeting trial criteria do not vary by left ventricular ejection fraction,” Gregg C. Fonarow, MD, University of California, Los Angeles, Medical Center, said in an interview.
It remains unknown, however, “whether the improvement in health status, functional status, and reduced inflammation” will translate to reduced risk of cardiovascular death or HF hospitalization, said Dr. Fonarow, who isn’t connected to STEP-HFpEF.
It’s a question for future studies, he agreed, whether semaglutide would confer similar benefits for patients with obesity and HF with LVEF less than 45% or in non-obese HF patients.
Dr. McMurray proposed that future GLP-1 receptor agonist heart-failure trials should include non-obese patients to determine whether the effects seen in STEP-HFpEF were due to something more than weight loss. Trials in patients with obesity and HF with reduced LVEF would also be important.
“If it turns out just to be about weight loss, then we need to think about the alternatives,” including diet, exercise, and bariatric surgery but also, potentially, weight-loss drugs other than semaglutide, he said.
No heterogeneity by LVEF
STEP-HFpEF randomly assigned 529 patients free of diabetes with an LVEF greater than or equal to 45%, a body mass index (BMI) of at least 30 kg/m2, and NYHA functional status of 2-4 to either a placebo injection or 2.4-mg semaglutide subcutaneously once a week (the dose used for weight reduction) atop standard care.
As previously reported, those assigned to semaglutide showed significant improvements at 1 year in symptoms and in physical limitation, per changes in KCCQ-CSS, and weight loss, compared with the control group. Their exercise capacity, as measured by 6MWD, also improved.
The more weight patients lost while taking semaglutide, the better their KCCQ-CSS and 6MWD outcomes, a prior secondary analysis suggested. But the STEP-HFpEF researchers said weight loss did not appear to explain all of their gains, compared with usual care.
For the current analysis, the 263 patients assigned to receive semaglutide and 266 control patients were divided into three groups by baseline LVEF and compared for the same outcomes.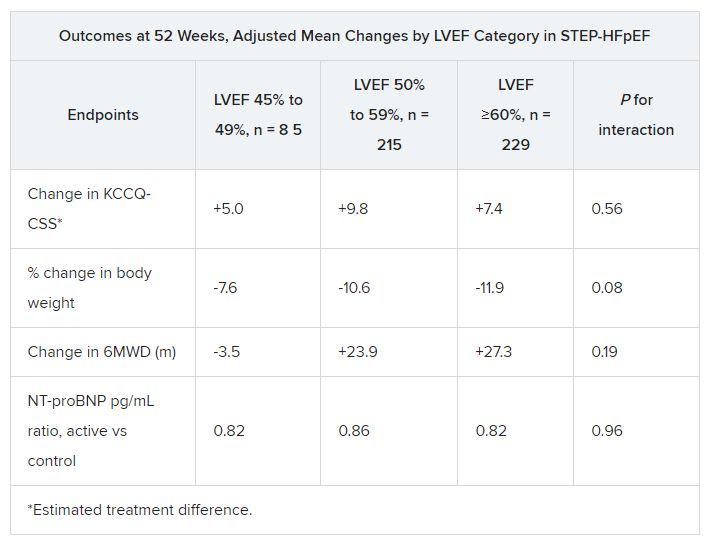
The semaglutide group, compared with control patients, also showed a significantly increased hierarchical composite win ratio, 1.72 (95% CI, 1.37-2.15; P < .001), that was consistent across LVEF categories and that accounted for all-cause mortality, HF events, KCCQ-CSS and 6MWD changes, and change in CRP.
Limitations make it hard to generalize the results, the authors caution. Well over 90% of the participants were White patients, for example, and the overall trial was not powered to show subgroup differences.
Given the many patients with HFpEF who have a cardiometabolic phenotype and are with overweight or obesity, write Dr. Butler and colleagues, their treatment approach “may ultimately include combination therapy with SGLT2 inhibitors and GLP-1 receptor agonists, given their non-overlapping and complementary mechanisms of action.”
Dr. Fonarow noted that both MRAs and sacubitril-valsartan offer clinical benefits for patients with HF and LVEF “in the 41%-60% range” that are evident “across BMI categories.”
So it’s likely, he said, that those medications as well as SGLT2 inhibitors will be used along with GLP-1 receptor agonists for patients with HFpEF and obesity.
STEP-HFpEF was funded by Novo Nordisk. Dr. Butler and the other authors disclose consulting for many companies, a list of which can be found in the report. Dr. Fonarow reports consulting for multiple companies. Dr. McMurray discloses consulting for AstraZeneca. Dr. Ostrominski reports no relevant disclosures. Dr. Vaduganathan discloses receiving grant support, serving on advisory boards, or speaking for multiple companies and serving on committees for studies sponsored by AstraZeneca, Galmed, Novartis, Bayer AG, Occlutech, and Impulse Dynamics.
A version of this article appeared on Medscape.com.
CLEVELAND – independently of baseline left-ventricular ejection fraction (LVEF).
The finding comes from a prespecified secondary analysis of the STEP-HFpEF trial of more than 500 nondiabetic patients with obesity and HF with an initial LVEF of 45% or greater.
They suggest that for patients with the obesity phenotype of HFpEF, semaglutide (Wegovy) could potentially join SGLT2 inhibitors on the short list of meds with consistent treatment effects whether LVEF is mildly reduced, preserved, or in the normal range.
That would distinguish the drug, a glucagon-like peptide-1 (GLP-1) receptor agonist, from mineralocorticoid receptor antagonists (MRA), sacubitril-valsartan (Entresto), and other renin-angiotensin-system inhibitors (RASi), whose benefits tend to taper off with rising LVEF.
The patients assigned to semaglutide showed significant improvement in both primary endpoints – change in Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS) and change in body weight at 52 weeks – whether their baseline LVEF was 45%-49%, 50%-59%, or 60% or greater.
Results were similar for improvements in 6-minute walk distance (6MWD) and levels of NT-terminal pro–brain natriuretic peptide (NT-proBNP) and C-reactive protein, observed Javed Butler, MD, when presenting the analysis at the annual meeting of the Heart Failure Society of America, Cleveland.
Dr. Butler, of Baylor Scott and White Research Institute, Dallas, and the University of Mississippi, Jackson, is also lead author of the study, which was published on the same day in the Journal of the American College of Cardiology.
In his presentation, Dr. Butler singled out the NT-proBNP finding as “very meaningful” with respect to understanding potential mechanisms of the drug effects observed in the trial.
For example, people with obesity tend to have lower than average natriuretic peptide levels that “actually go up a bit” when they lose weight, he observed. But in the trial, “we saw a reduction in NT-proBNP in spite of the weight loss,” regardless of LVEF category.
John McMurray, MD, University of Glasgow, the invited discussant for Dr. Butler’s presentation, agreed that it raises the question whether weight loss was the sole semaglutide effect responsible for the improvement in heart failure status and biomarkers. The accompanying NT-proBNP reductions – when the opposite might otherwise have been expected – may point to a possible mechanism of action that is “something more than just weight loss,” he said. “If that were the case, it becomes very important, because it means that this treatment might do good things in non-obese patients or might do good things in patients with other types of heart failure.”
‘Vital reassurance’
More definitive trials are needed “to clarify safety and efficacy of obesity-targeted therapeutics in HF across the ejection fraction spectrum,” according to an accompanying editorial).
Still, the STEP-HFpEF analysis “strengthens the role of GLP-1 [receptor agonists] to ameliorate health status” for patients with obesity and HF with mildly reduced or preserved ejection fraction, write Muthiah Vaduganathan, MD, MPH, and John W. Ostrominski, MD, Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Its findings “provide vital reassurance” on semaglutide safety and efficacy in HF with below-normal LVEF and “tentatively support the existence of a more general, LVEF-independent, obesity-related HF phenotype capable of favorable modification with incretin-based therapies.”
The lack of heterogeneity in treatment effects across LVEF subgroups “is not surprising,” but “the findings reinforce that the benefits of this therapy in those meeting trial criteria do not vary by left ventricular ejection fraction,” Gregg C. Fonarow, MD, University of California, Los Angeles, Medical Center, said in an interview.
It remains unknown, however, “whether the improvement in health status, functional status, and reduced inflammation” will translate to reduced risk of cardiovascular death or HF hospitalization, said Dr. Fonarow, who isn’t connected to STEP-HFpEF.
It’s a question for future studies, he agreed, whether semaglutide would confer similar benefits for patients with obesity and HF with LVEF less than 45% or in non-obese HF patients.
Dr. McMurray proposed that future GLP-1 receptor agonist heart-failure trials should include non-obese patients to determine whether the effects seen in STEP-HFpEF were due to something more than weight loss. Trials in patients with obesity and HF with reduced LVEF would also be important.
“If it turns out just to be about weight loss, then we need to think about the alternatives,” including diet, exercise, and bariatric surgery but also, potentially, weight-loss drugs other than semaglutide, he said.
No heterogeneity by LVEF
STEP-HFpEF randomly assigned 529 patients free of diabetes with an LVEF greater than or equal to 45%, a body mass index (BMI) of at least 30 kg/m2, and NYHA functional status of 2-4 to either a placebo injection or 2.4-mg semaglutide subcutaneously once a week (the dose used for weight reduction) atop standard care.
As previously reported, those assigned to semaglutide showed significant improvements at 1 year in symptoms and in physical limitation, per changes in KCCQ-CSS, and weight loss, compared with the control group. Their exercise capacity, as measured by 6MWD, also improved.
The more weight patients lost while taking semaglutide, the better their KCCQ-CSS and 6MWD outcomes, a prior secondary analysis suggested. But the STEP-HFpEF researchers said weight loss did not appear to explain all of their gains, compared with usual care.
For the current analysis, the 263 patients assigned to receive semaglutide and 266 control patients were divided into three groups by baseline LVEF and compared for the same outcomes.
The semaglutide group, compared with control patients, also showed a significantly increased hierarchical composite win ratio, 1.72 (95% CI, 1.37-2.15; P < .001), that was consistent across LVEF categories and that accounted for all-cause mortality, HF events, KCCQ-CSS and 6MWD changes, and change in CRP.
Limitations make it hard to generalize the results, the authors caution. Well over 90% of the participants were White patients, for example, and the overall trial was not powered to show subgroup differences.
Given the many patients with HFpEF who have a cardiometabolic phenotype and are with overweight or obesity, write Dr. Butler and colleagues, their treatment approach “may ultimately include combination therapy with SGLT2 inhibitors and GLP-1 receptor agonists, given their non-overlapping and complementary mechanisms of action.”
Dr. Fonarow noted that both MRAs and sacubitril-valsartan offer clinical benefits for patients with HF and LVEF “in the 41%-60% range” that are evident “across BMI categories.”
So it’s likely, he said, that those medications as well as SGLT2 inhibitors will be used along with GLP-1 receptor agonists for patients with HFpEF and obesity.
STEP-HFpEF was funded by Novo Nordisk. Dr. Butler and the other authors disclose consulting for many companies, a list of which can be found in the report. Dr. Fonarow reports consulting for multiple companies. Dr. McMurray discloses consulting for AstraZeneca. Dr. Ostrominski reports no relevant disclosures. Dr. Vaduganathan discloses receiving grant support, serving on advisory boards, or speaking for multiple companies and serving on committees for studies sponsored by AstraZeneca, Galmed, Novartis, Bayer AG, Occlutech, and Impulse Dynamics.
A version of this article appeared on Medscape.com.
CLEVELAND – independently of baseline left-ventricular ejection fraction (LVEF).
The finding comes from a prespecified secondary analysis of the STEP-HFpEF trial of more than 500 nondiabetic patients with obesity and HF with an initial LVEF of 45% or greater.
They suggest that for patients with the obesity phenotype of HFpEF, semaglutide (Wegovy) could potentially join SGLT2 inhibitors on the short list of meds with consistent treatment effects whether LVEF is mildly reduced, preserved, or in the normal range.
That would distinguish the drug, a glucagon-like peptide-1 (GLP-1) receptor agonist, from mineralocorticoid receptor antagonists (MRA), sacubitril-valsartan (Entresto), and other renin-angiotensin-system inhibitors (RASi), whose benefits tend to taper off with rising LVEF.
The patients assigned to semaglutide showed significant improvement in both primary endpoints – change in Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS) and change in body weight at 52 weeks – whether their baseline LVEF was 45%-49%, 50%-59%, or 60% or greater.
Results were similar for improvements in 6-minute walk distance (6MWD) and levels of NT-terminal pro–brain natriuretic peptide (NT-proBNP) and C-reactive protein, observed Javed Butler, MD, when presenting the analysis at the annual meeting of the Heart Failure Society of America, Cleveland.
Dr. Butler, of Baylor Scott and White Research Institute, Dallas, and the University of Mississippi, Jackson, is also lead author of the study, which was published on the same day in the Journal of the American College of Cardiology.
In his presentation, Dr. Butler singled out the NT-proBNP finding as “very meaningful” with respect to understanding potential mechanisms of the drug effects observed in the trial.
For example, people with obesity tend to have lower than average natriuretic peptide levels that “actually go up a bit” when they lose weight, he observed. But in the trial, “we saw a reduction in NT-proBNP in spite of the weight loss,” regardless of LVEF category.
John McMurray, MD, University of Glasgow, the invited discussant for Dr. Butler’s presentation, agreed that it raises the question whether weight loss was the sole semaglutide effect responsible for the improvement in heart failure status and biomarkers. The accompanying NT-proBNP reductions – when the opposite might otherwise have been expected – may point to a possible mechanism of action that is “something more than just weight loss,” he said. “If that were the case, it becomes very important, because it means that this treatment might do good things in non-obese patients or might do good things in patients with other types of heart failure.”
‘Vital reassurance’
More definitive trials are needed “to clarify safety and efficacy of obesity-targeted therapeutics in HF across the ejection fraction spectrum,” according to an accompanying editorial).
Still, the STEP-HFpEF analysis “strengthens the role of GLP-1 [receptor agonists] to ameliorate health status” for patients with obesity and HF with mildly reduced or preserved ejection fraction, write Muthiah Vaduganathan, MD, MPH, and John W. Ostrominski, MD, Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
Its findings “provide vital reassurance” on semaglutide safety and efficacy in HF with below-normal LVEF and “tentatively support the existence of a more general, LVEF-independent, obesity-related HF phenotype capable of favorable modification with incretin-based therapies.”
The lack of heterogeneity in treatment effects across LVEF subgroups “is not surprising,” but “the findings reinforce that the benefits of this therapy in those meeting trial criteria do not vary by left ventricular ejection fraction,” Gregg C. Fonarow, MD, University of California, Los Angeles, Medical Center, said in an interview.
It remains unknown, however, “whether the improvement in health status, functional status, and reduced inflammation” will translate to reduced risk of cardiovascular death or HF hospitalization, said Dr. Fonarow, who isn’t connected to STEP-HFpEF.
It’s a question for future studies, he agreed, whether semaglutide would confer similar benefits for patients with obesity and HF with LVEF less than 45% or in non-obese HF patients.
Dr. McMurray proposed that future GLP-1 receptor agonist heart-failure trials should include non-obese patients to determine whether the effects seen in STEP-HFpEF were due to something more than weight loss. Trials in patients with obesity and HF with reduced LVEF would also be important.
“If it turns out just to be about weight loss, then we need to think about the alternatives,” including diet, exercise, and bariatric surgery but also, potentially, weight-loss drugs other than semaglutide, he said.
No heterogeneity by LVEF
STEP-HFpEF randomly assigned 529 patients free of diabetes with an LVEF greater than or equal to 45%, a body mass index (BMI) of at least 30 kg/m2, and NYHA functional status of 2-4 to either a placebo injection or 2.4-mg semaglutide subcutaneously once a week (the dose used for weight reduction) atop standard care.
As previously reported, those assigned to semaglutide showed significant improvements at 1 year in symptoms and in physical limitation, per changes in KCCQ-CSS, and weight loss, compared with the control group. Their exercise capacity, as measured by 6MWD, also improved.
The more weight patients lost while taking semaglutide, the better their KCCQ-CSS and 6MWD outcomes, a prior secondary analysis suggested. But the STEP-HFpEF researchers said weight loss did not appear to explain all of their gains, compared with usual care.
For the current analysis, the 263 patients assigned to receive semaglutide and 266 control patients were divided into three groups by baseline LVEF and compared for the same outcomes.
The semaglutide group, compared with control patients, also showed a significantly increased hierarchical composite win ratio, 1.72 (95% CI, 1.37-2.15; P < .001), that was consistent across LVEF categories and that accounted for all-cause mortality, HF events, KCCQ-CSS and 6MWD changes, and change in CRP.
Limitations make it hard to generalize the results, the authors caution. Well over 90% of the participants were White patients, for example, and the overall trial was not powered to show subgroup differences.
Given the many patients with HFpEF who have a cardiometabolic phenotype and are with overweight or obesity, write Dr. Butler and colleagues, their treatment approach “may ultimately include combination therapy with SGLT2 inhibitors and GLP-1 receptor agonists, given their non-overlapping and complementary mechanisms of action.”
Dr. Fonarow noted that both MRAs and sacubitril-valsartan offer clinical benefits for patients with HF and LVEF “in the 41%-60% range” that are evident “across BMI categories.”
So it’s likely, he said, that those medications as well as SGLT2 inhibitors will be used along with GLP-1 receptor agonists for patients with HFpEF and obesity.
STEP-HFpEF was funded by Novo Nordisk. Dr. Butler and the other authors disclose consulting for many companies, a list of which can be found in the report. Dr. Fonarow reports consulting for multiple companies. Dr. McMurray discloses consulting for AstraZeneca. Dr. Ostrominski reports no relevant disclosures. Dr. Vaduganathan discloses receiving grant support, serving on advisory boards, or speaking for multiple companies and serving on committees for studies sponsored by AstraZeneca, Galmed, Novartis, Bayer AG, Occlutech, and Impulse Dynamics.
A version of this article appeared on Medscape.com.
AT HFSA 2023
Short, long-lasting bronchodilators similar for exacerbated COPD
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
HONOLULU – in safety and efficacy to a short-acting combination of albuterol and ipratropium.
The 2023 Gold Report on prevention, management, and diagnosis of COPD recommended switching to long-acting bronchodilators despite a lack of clinical evidence showing safety in patients hospitalized for COPD exacerbation, according to Rajiv Dhand, MD, who presented the new study at the annual meeting of the American College of Chest Physicians (CHEST).
“We wanted to establish the safety, because long-acting agents are approved only for use in nonhospitalized patients. We established that it was safe and that it was comparably effective, but you could give 30% lower doses. Patients don’t have to be woken up to get the medication, and there’s a better chance that all the doses will be administered to these patients. So I think that it provides convenience with similar efficacy and safety,” said Dr. Dhand, a pulmonologist and professor of medicine at the University of Tennessee, Knoxville.
The researchers randomized 60 patients to receive nebulized albuterol (2.5 mg) and ipratropium (0.5 mg) every 6 hours (short-acting group) or nebulized formoterol (20 mcg) every 12 hours and revefenacin (175 mcg) every 24 hours (long-acting group). The mean age was 63.2 years, 58.3% were male, and 65% were current smokers.
The median decrease between day 1 and day 3 in the Modified Borg Dyspnea score was 4.0 in the long-acting group (P < .001), and 2.0 in the short-acting group, though the latter was not statistically significant (P = .134). Both groups had a decrease in supplemental oxygen requirement, with no difference between the two groups. There was also no difference in the number of respiratory visits for rescue therapy.
Respiratory therapists in the audience welcomed the new evidence. “As a respiratory therapist, I feel that we should move away from giving good short acting [therapies] ... the new guidelines state that we should move away from them, but I think that physicians in general have not gone that way. The way that we’re working, giving short acting every four hours – I don’t see that it’s a benefit to our patients,” said Sharon Armstead, who attended the session and was asked to comment on the study. She is a respiratory therapist at Ascension Health and an instructor at Concordia University, Austin, Texas. Ms. Armstead has asthma, and has first-hand experience as a patient when respiratory therapists are unable to attend to the patient every 4 hours.
She suggested that continued use of short-acting therapies may be due to inertia. “It’s easier [for a physician] to click a button on [a computer screen] than to actually slow down and write the order. If we need a rescue, then we’ll call for a rescue,” Ms. Armstead said.
She anticipates that long-acting therapies will ultimately lead to better outcomes because they will increase the time that respiratory therapists can spend with patients. “That’s what we really want to do. We want to spend time with our patients and stay there and watch our patients. But if you’re just telling us to [administer a therapy] every 4 hours, it’s not really giving the patient what they need.”
Specifically, there were concerns about cardiovascular safety, but the researchers found no between-group differences.
Asked for comment, session co-moderator Brittany Duchene, MD remarked: “It’s super interesting, but I worry about the cost. From a practical perspective, it’s challenging to get those drugs placed on an outpatient basis. They are very expensive, and they’re newer [drugs], but I think overall it’s good to give less,” said Dr. Duchene, a pulmonary critical care physician at Northeastern Vermont Regional Hospital, St. Johnsbury.
A potential concern raised by one audience member is that some patients are used to frequent treatment and may grow anxious with less frequent therapy. “I think we just need some reeducation that this is like a long-acting medicine. It also decreases the burden on our respiratory therapists, which is very good,” said Dr. Duchene.
The study was funded by Mylan/Theravance Biopharma. Dr. Dhand has received research support from Theravance, Mylan, and Viatris. He has received honoraria from Teva and UpToDate. Ms. Armstead and Dr. Duchene have no relevant financial disclosures.
AT CHEST 2023
Head, neck cancer radiotherapy regimen saves time when resources limited
SAN DIEGO – In low- and middle-income countries with high incidence and mortality from head and neck cancer, resources remain limited. Patients often can’t travel far for treatment or afford to stay near a treatment center for the length of time required for conventionally fractionated radiotherapy.
in these settings.
The phase 3 randomized HYPNO trial, conducted in 10 low- and middle-income countries, revealed that the hypofractionated regimen shortened total treatment time by a median of 11.5 days and was noninferior to conventional fractionation for tumor control and safety.
The primary trial results were presented by Søren Bentzen, PhD, DMSc, at the annual meeting of the American Society for Radiation Oncology.
“It was Usain Bolt who said, ‘I train for 4 years to run 9 seconds,’ and that was the feeling that I had when we did the noninferiority test,” said Dr. Bentzen, from the University of Maryland School of Medicine in Baltimore. “We had not looked at the data while the data were being accumulated, and guess what? It actually turned out that we had noninferiority with respect to both locoregional control and the late effects.”
In the HYPNO trial, Dr. Bentzen and colleagues wanted to determine whether a streamlined approach to the treatment of patients in low- and middle-income countries could improve access to care and still achieve strong outcomes.
The investigators used mathematical modeling to devise a strategy to reduce the number of fractions and put this hypothesis to the test in a pragmatic trial.
Patients from Uruguay, Brazil, Argentina, Cuba, South Africa, India, Pakistan, Thailand, Indonesia, and the Philippines were enrolled. After stratification by performance status, tumor subsite, institution, and previous treatment with chemotherapy, the 792 patients in the trial were randomly assigned in a 1:1 ratio to receive either 66 Gy in 33 fractions 6 days each week over 5.5 weeks, or 55 Gy in 20 fractions 5 days per week over 4 weeks. In both groups, weekly cisplatin was optional.
Compliance with the regimens was high in both arms, with 95% of patients assigned to conventional fractionation and 99% assigned to hypofractionation receiving the total planned doses.
At 3 years’ follow-up, the rates of locoregional control were 50.7% in the hypofractionation arm and 51.2% in the conventional fractionation arm (P = .40). No significant differences between the groups have emerged over 5 years, Dr. Bentzen said.
Rates of late toxicities of grade 3 or greater at 3 years’ follow-up were similar between the groups, at 18.8% in the hypofractionation arm and 20.2% in the conventional fractionation arm (P = .68).
Three-year overall survival rates also did not differ between the groups – 54.1% in the hypofractionation arm vs. 55.5% in the conventional arm (P = .62) – nor did rates of progression-free survival – 44.0% vs. 45.3%.
“Head and neck cancer caused by factors other than the human papillomavirus (HPV) remains a significant burden especially in lower- and middle-income countries,” Dr. Bentzen said in a press release. “This is a trial that directly informs how you can effectively deliver radiation therapy to patients in a resource-scarce environment.”
Beth Beadle, MD, PhD, the invited discussant at a media briefing where Dr. Bentzen summarized the findings, said, “I think this trial is going to change practice in low- and middle-income countries and will improve access to care.”
Although the approach used in the HYPNO trial will likely allow more patients to receive treatment and will save lives in countries with limited resources, the strategy likely won’t apply to U.S. practice, noted Dr. Beadle, a professor of radiation oncology at Stanford University, California.
“The one thing I do caution, and that Dr. Bentzen brought up, is that this is a very different population than the one that we see in the United States now,” Dr. Beadle said. “In fact, it’s very challenging to find a similar patient population to even serve as a comparison in the modern era and modern techniques.”
The HYPNO trial was sponsored by the International Atomic Energy Agency. Dr. Bentzen and Dr. Beadle have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – In low- and middle-income countries with high incidence and mortality from head and neck cancer, resources remain limited. Patients often can’t travel far for treatment or afford to stay near a treatment center for the length of time required for conventionally fractionated radiotherapy.
in these settings.
The phase 3 randomized HYPNO trial, conducted in 10 low- and middle-income countries, revealed that the hypofractionated regimen shortened total treatment time by a median of 11.5 days and was noninferior to conventional fractionation for tumor control and safety.
The primary trial results were presented by Søren Bentzen, PhD, DMSc, at the annual meeting of the American Society for Radiation Oncology.
“It was Usain Bolt who said, ‘I train for 4 years to run 9 seconds,’ and that was the feeling that I had when we did the noninferiority test,” said Dr. Bentzen, from the University of Maryland School of Medicine in Baltimore. “We had not looked at the data while the data were being accumulated, and guess what? It actually turned out that we had noninferiority with respect to both locoregional control and the late effects.”
In the HYPNO trial, Dr. Bentzen and colleagues wanted to determine whether a streamlined approach to the treatment of patients in low- and middle-income countries could improve access to care and still achieve strong outcomes.
The investigators used mathematical modeling to devise a strategy to reduce the number of fractions and put this hypothesis to the test in a pragmatic trial.
Patients from Uruguay, Brazil, Argentina, Cuba, South Africa, India, Pakistan, Thailand, Indonesia, and the Philippines were enrolled. After stratification by performance status, tumor subsite, institution, and previous treatment with chemotherapy, the 792 patients in the trial were randomly assigned in a 1:1 ratio to receive either 66 Gy in 33 fractions 6 days each week over 5.5 weeks, or 55 Gy in 20 fractions 5 days per week over 4 weeks. In both groups, weekly cisplatin was optional.
Compliance with the regimens was high in both arms, with 95% of patients assigned to conventional fractionation and 99% assigned to hypofractionation receiving the total planned doses.
At 3 years’ follow-up, the rates of locoregional control were 50.7% in the hypofractionation arm and 51.2% in the conventional fractionation arm (P = .40). No significant differences between the groups have emerged over 5 years, Dr. Bentzen said.
Rates of late toxicities of grade 3 or greater at 3 years’ follow-up were similar between the groups, at 18.8% in the hypofractionation arm and 20.2% in the conventional fractionation arm (P = .68).
Three-year overall survival rates also did not differ between the groups – 54.1% in the hypofractionation arm vs. 55.5% in the conventional arm (P = .62) – nor did rates of progression-free survival – 44.0% vs. 45.3%.
“Head and neck cancer caused by factors other than the human papillomavirus (HPV) remains a significant burden especially in lower- and middle-income countries,” Dr. Bentzen said in a press release. “This is a trial that directly informs how you can effectively deliver radiation therapy to patients in a resource-scarce environment.”
Beth Beadle, MD, PhD, the invited discussant at a media briefing where Dr. Bentzen summarized the findings, said, “I think this trial is going to change practice in low- and middle-income countries and will improve access to care.”
Although the approach used in the HYPNO trial will likely allow more patients to receive treatment and will save lives in countries with limited resources, the strategy likely won’t apply to U.S. practice, noted Dr. Beadle, a professor of radiation oncology at Stanford University, California.
“The one thing I do caution, and that Dr. Bentzen brought up, is that this is a very different population than the one that we see in the United States now,” Dr. Beadle said. “In fact, it’s very challenging to find a similar patient population to even serve as a comparison in the modern era and modern techniques.”
The HYPNO trial was sponsored by the International Atomic Energy Agency. Dr. Bentzen and Dr. Beadle have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – In low- and middle-income countries with high incidence and mortality from head and neck cancer, resources remain limited. Patients often can’t travel far for treatment or afford to stay near a treatment center for the length of time required for conventionally fractionated radiotherapy.
in these settings.
The phase 3 randomized HYPNO trial, conducted in 10 low- and middle-income countries, revealed that the hypofractionated regimen shortened total treatment time by a median of 11.5 days and was noninferior to conventional fractionation for tumor control and safety.
The primary trial results were presented by Søren Bentzen, PhD, DMSc, at the annual meeting of the American Society for Radiation Oncology.
“It was Usain Bolt who said, ‘I train for 4 years to run 9 seconds,’ and that was the feeling that I had when we did the noninferiority test,” said Dr. Bentzen, from the University of Maryland School of Medicine in Baltimore. “We had not looked at the data while the data were being accumulated, and guess what? It actually turned out that we had noninferiority with respect to both locoregional control and the late effects.”
In the HYPNO trial, Dr. Bentzen and colleagues wanted to determine whether a streamlined approach to the treatment of patients in low- and middle-income countries could improve access to care and still achieve strong outcomes.
The investigators used mathematical modeling to devise a strategy to reduce the number of fractions and put this hypothesis to the test in a pragmatic trial.
Patients from Uruguay, Brazil, Argentina, Cuba, South Africa, India, Pakistan, Thailand, Indonesia, and the Philippines were enrolled. After stratification by performance status, tumor subsite, institution, and previous treatment with chemotherapy, the 792 patients in the trial were randomly assigned in a 1:1 ratio to receive either 66 Gy in 33 fractions 6 days each week over 5.5 weeks, or 55 Gy in 20 fractions 5 days per week over 4 weeks. In both groups, weekly cisplatin was optional.
Compliance with the regimens was high in both arms, with 95% of patients assigned to conventional fractionation and 99% assigned to hypofractionation receiving the total planned doses.
At 3 years’ follow-up, the rates of locoregional control were 50.7% in the hypofractionation arm and 51.2% in the conventional fractionation arm (P = .40). No significant differences between the groups have emerged over 5 years, Dr. Bentzen said.
Rates of late toxicities of grade 3 or greater at 3 years’ follow-up were similar between the groups, at 18.8% in the hypofractionation arm and 20.2% in the conventional fractionation arm (P = .68).
Three-year overall survival rates also did not differ between the groups – 54.1% in the hypofractionation arm vs. 55.5% in the conventional arm (P = .62) – nor did rates of progression-free survival – 44.0% vs. 45.3%.
“Head and neck cancer caused by factors other than the human papillomavirus (HPV) remains a significant burden especially in lower- and middle-income countries,” Dr. Bentzen said in a press release. “This is a trial that directly informs how you can effectively deliver radiation therapy to patients in a resource-scarce environment.”
Beth Beadle, MD, PhD, the invited discussant at a media briefing where Dr. Bentzen summarized the findings, said, “I think this trial is going to change practice in low- and middle-income countries and will improve access to care.”
Although the approach used in the HYPNO trial will likely allow more patients to receive treatment and will save lives in countries with limited resources, the strategy likely won’t apply to U.S. practice, noted Dr. Beadle, a professor of radiation oncology at Stanford University, California.
“The one thing I do caution, and that Dr. Bentzen brought up, is that this is a very different population than the one that we see in the United States now,” Dr. Beadle said. “In fact, it’s very challenging to find a similar patient population to even serve as a comparison in the modern era and modern techniques.”
The HYPNO trial was sponsored by the International Atomic Energy Agency. Dr. Bentzen and Dr. Beadle have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ASTRO 2023