User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Employment and buyout agreements
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.

Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.
Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
. The most common question was, “Do I really need to go to the trouble and expense of negotiating them?” If you have more than one physician in your group, you absolutely do need written contracts for a variety of reasons, but mostly to avoid conflicts later on. The proverbial “handshake agreement” is worthless in a major business dispute; everyone loses in such situations except the lawyers and accountants.
Mergers and buy-ins were covered at some length in my two previous columns. If the arrangement is to be one of employer and employees rather than a merger of equal partners, you will need an employment agreement to cover duties, requirements, expectations, and benefits. They define how each practitioner/employee will be paid, along with paid time off, health insurance, expense allowances, and malpractice coverage, among other basics. The more that is spelled out in the employment agreement, the fewer disagreements you are likely to have down the road.
Many employment contracts include a “termination without cause” clause, which benefits both the practice and the practitioners. It allows a practice to terminate a new associate if it feels a mistake has been made, even if he or she has done nothing wrong. On the other hand, the newcomer has the option to terminate if a better offer arises, their spouse hates the area, or for any other reason.
Buyouts should be addressed in advance as well. Several recent correspondents told me they didn’t see the necessity of writing a buyout agreement, because they plan to eventually sell their practice, rendering any buyout conditions moot. But what happens if an associate dies, becomes permanently disabled, or abruptly decides to leave the practice? If you haven’t prepared for such eventualities, you could find yourself receiving a demand from your ex-partner (or surviving spouse) for immediate payment of that partner’s portion of the practice’s value. And your valuation of the practice is likely to be severely at odds with the other party’s. Meanwhile, remaining partners must cover all the practice’s expenses and deal with an increased patient load.
A buyout agreement avoids these problems by planning for such eventualities in advance. You must agree on how a buyout amount will be valued. As I’ve said in previous columns, I strongly advise using a formula, not a fixed amount. If a buyout is based on 15- or 20-year-old reimbursements, the buyout will have no relationship to what the partners are currently being paid. Likewise, any buyout calculated at “appraised value” is a problem, because the buyout amount remains a mystery until an appraisal is performed. If the appraised value ends up being too high, the remaining owners may refuse to pay it. Have an actuary create a formula, so that a buyout figure can be calculated at any time. This area, especially, is where you need experienced, competent legal advice.
To avoid surprises, any buyout should require ample notice (6-12 months is common) to allow time to rearrange finances and recruit a new provider. Vesting schedules, similar to those used in retirement plans, are also popular. If a partner leaves before a prescribed time period has elapsed – say, 20 years – the buyout is proportionally reduced.
Buyouts can also be useful when dealing with noncompete agreements, which are notoriously difficult (and expensive) to enforce. One solution is a buyout penalty; a departing partner can compete with his or her former practice, but at the cost of a substantially reduced buyout. This permits competition, but discourages it, and compensates the targeted practice.
Buyouts are also a potential solution to some buy-in issues. A new associate entering an established practice may not be able to contribute assets equal to existing partners’ stakes and may lack the cash necessary to make up the difference. One alternative is to agree that any inequalities will be compensated at the other end in buyout value. Those partners contributing more assets will receive larger buyouts than those contributing less.
As I’ve said many times, these are not negotiations to undertake on your own. Enlist the aid of a consultant or attorney (or both) with ample medical practice experience.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Biomarkers may help to predict persistent oligoarticular JIA
Ongoing research in patients with oligoarticular juvenile idiopathic arthritis (JIA) so far suggests that a set of biomarkers in synovial fluid may help to predict which patients may be more likely to stay with persistent oligoarticular disease rather than progress to polyarticular disease, according to new research presented at the annual scientific meeting of the Childhood Arthritis and Rheumatology Research Alliance, held virtually this year. Identifying biomarkers in synovial fluid or possibly serum could aid families and physicians in being more proactive in treatment protocols, said AnneMarie C. Brescia, MD, of Nemours Children’s Hospital in Wilmington, Del.
“JIA carries the risk of permanent joint damage and disability, which can result when joint involvement evolves from oligoarticular into a polyarticular course, termed extended oligoarticular disease,” Dr. Brescia told attendees. “Since disease progression increases the risk for disability, early prediction of this course is essential.”
This group – those whose oligoarticular disease will begin recruiting joints and ultimately become extended oligoarticular JIA – is “very important because they have been shown to have worse health-related quality of life and greater risk of needing a joint replacement than even polyarticular [JIA],” Dr. Brescia said. “So, our lab has really focused on trying to predict who will fall in this group.”
Melissa Oliver, MD, assistant professor of clinical pediatrics in the division of pediatric rheumatology at Indiana University in Indianapolis, was not involved in the study but agreed that having highly sensitive and specific biomarkers could be particularly helpful in clinical care.
“Biomarkers can help guide treatment decisions and help physicians and their patients share the decision-making about next choices and when to change,” Dr. Oliver told this news organization. “If a provider and parent know that their child has these markers in their serum or synovial fluid that may predict extension of their disease, then they may be more aggressive upfront with therapy.”
The study aimed to determine whether differential levels of synovial fluid proteins could be used to predict whether JIA would evolve into an extended course before it became clinically evident. Although early aggressive treatment is common with rheumatoid arthritis and can lead to remission, JIA treatment paradigms tend to be more reactive, Dr. Brescia said.
“It would be better to switch to proactive, that if we’re able to predict that this patient may have a more difficult course with extension to polyarticular, we could be prepared, we could inform the parents, and it would just help us have a more proactive approach,” she said.
The researchers used antibody arrays to detect the following inflammatory mediators in blinded samples: CD14, interleukin (IL)-1-alpha, IL-3, IL-5, IL-6, vascular endothelial growth factor (VEGF), and angiogenin. They analyzed 37 samples with persistent disease and 32 samples from disease that had not yet extended but would become extended in that patient. The samples came from patients who were taking no medicines or only NSAIDs. The researchers assessed the sensitivity and specificity of each biomarker. Sensitivity referred the biomarker’s ability to correctly indicate that the sample would extend, and specificity referred to the biomarker’s accuracy in determining that the disease in the sample would remain persistent.
Combining samples from cohorts at Nemours Children’s Health (14 persistent and 7 extended-to-be) and Cincinnati Children’s Hospital (23 persistent and 25 extended-to-be) yielded the following results: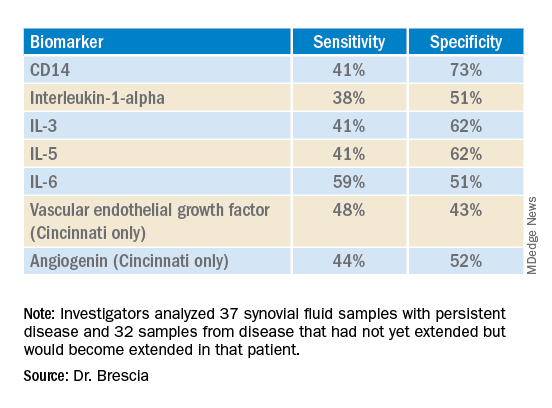
The findings revealed that the selected biomarkers were more accurate at predicting whose disease would remain persistent than predicting those that would extend, Dr. Brescia said. CD14 was the most specific biomarker, and IL-6 was the most sensitive biomarker in both groups.
When the researchers translated the findings from ELISA to the Luminex platform, positive results in synovial fluid for all these biomarkers were also positive in serum samples. Although the differences between persistent and extended-to-be samples did not reach statistical significance using Luminex, the pattern was the same for each biomarker.
“Luminex is more sensitive than ELISA. We believe that conducting an LDA [linear discriminant analysis] using these Luminex measurements will allow us to determine new cutoffs or new protein levels that are appropriate for Luminex to predict who will extend,” Dr. Brescia said. “It’s also our goal to develop a serum panel because ... being able to detect these markers in serum would expand the applicability of these markers to more patients.”
Dr. Brescia then described the group’s work in defining clinically relevant subpopulations of patients based on fibroblast-like synoviocytes (FLS) cells in the synovial intimal lining that produce inflammatory cytokines.
“Our compelling, single-cell, RNA sequencing preliminary data revealing multiple subpopulations within the total FLS population supports our hypothesis that distinct FLS subpopulations correlate with clinical outcome,” said Dr. Brescia. They looked at the percentage of chondrocyte-like, fibroblast-like, and smooth muscle-like subpopulations in samples from patients with oligoarticular JIA, extended-to-be JIA, and polyarticular JIA. Chondrocytes occurred in the largest proportion, and polyarticular JIA FLS had the largest percentage of chondrocytes, compared with the other two subpopulation groups.
“This is a work in progress,” Dr. Brescia said, “so hopefully you’ll hear about it next year.” In response to an attendee’s question, she said she believes identifying reliable biomarkers will eventually lead to refining treatment paradigms.
“I think it will at least change the guidance we can provide parents about making next choices and how quickly to accelerate to those next choices,” Dr. Brescia said. For example, if a child’s serum or synovial fluid has markers that show a very high likelihood of extension, the parent may decide to proceed to the next level medication sooner. “I do think it will push both parents and doctors to be a little more proactive instead of reactive when the poor patient comes back with 13 joints involved when they had just been an oligo for years.”
Dr. Oliver noted the promise of CD14 and IL-6 in potentially predicting which patients’ disease will stay persistent but cautioned that it’s still early in evaluating these biomarkers, especially with the limited patient samples in this study.
“I think these results are promising, and it’s great that there are groups out there working on this,” Dr. Oliver said. “Once we have a reliable, highly sensitive and specific biomarker, that will definitely help providers, parents, and patients be more informed.”
The research was supported by the Open Net Foundation, the Arthritis Foundation, Delaware Community Foundation, the Delaware Clinical and Translational Research (DE-CTR) ACCEL Program, the Nancy Taylor Foundation for Chronic Diseases, and CARRA. Dr. Brescia and Dr. Oliver have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Ongoing research in patients with oligoarticular juvenile idiopathic arthritis (JIA) so far suggests that a set of biomarkers in synovial fluid may help to predict which patients may be more likely to stay with persistent oligoarticular disease rather than progress to polyarticular disease, according to new research presented at the annual scientific meeting of the Childhood Arthritis and Rheumatology Research Alliance, held virtually this year. Identifying biomarkers in synovial fluid or possibly serum could aid families and physicians in being more proactive in treatment protocols, said AnneMarie C. Brescia, MD, of Nemours Children’s Hospital in Wilmington, Del.
“JIA carries the risk of permanent joint damage and disability, which can result when joint involvement evolves from oligoarticular into a polyarticular course, termed extended oligoarticular disease,” Dr. Brescia told attendees. “Since disease progression increases the risk for disability, early prediction of this course is essential.”
This group – those whose oligoarticular disease will begin recruiting joints and ultimately become extended oligoarticular JIA – is “very important because they have been shown to have worse health-related quality of life and greater risk of needing a joint replacement than even polyarticular [JIA],” Dr. Brescia said. “So, our lab has really focused on trying to predict who will fall in this group.”
Melissa Oliver, MD, assistant professor of clinical pediatrics in the division of pediatric rheumatology at Indiana University in Indianapolis, was not involved in the study but agreed that having highly sensitive and specific biomarkers could be particularly helpful in clinical care.
“Biomarkers can help guide treatment decisions and help physicians and their patients share the decision-making about next choices and when to change,” Dr. Oliver told this news organization. “If a provider and parent know that their child has these markers in their serum or synovial fluid that may predict extension of their disease, then they may be more aggressive upfront with therapy.”
The study aimed to determine whether differential levels of synovial fluid proteins could be used to predict whether JIA would evolve into an extended course before it became clinically evident. Although early aggressive treatment is common with rheumatoid arthritis and can lead to remission, JIA treatment paradigms tend to be more reactive, Dr. Brescia said.
“It would be better to switch to proactive, that if we’re able to predict that this patient may have a more difficult course with extension to polyarticular, we could be prepared, we could inform the parents, and it would just help us have a more proactive approach,” she said.
The researchers used antibody arrays to detect the following inflammatory mediators in blinded samples: CD14, interleukin (IL)-1-alpha, IL-3, IL-5, IL-6, vascular endothelial growth factor (VEGF), and angiogenin. They analyzed 37 samples with persistent disease and 32 samples from disease that had not yet extended but would become extended in that patient. The samples came from patients who were taking no medicines or only NSAIDs. The researchers assessed the sensitivity and specificity of each biomarker. Sensitivity referred the biomarker’s ability to correctly indicate that the sample would extend, and specificity referred to the biomarker’s accuracy in determining that the disease in the sample would remain persistent.
Combining samples from cohorts at Nemours Children’s Health (14 persistent and 7 extended-to-be) and Cincinnati Children’s Hospital (23 persistent and 25 extended-to-be) yielded the following results:
The findings revealed that the selected biomarkers were more accurate at predicting whose disease would remain persistent than predicting those that would extend, Dr. Brescia said. CD14 was the most specific biomarker, and IL-6 was the most sensitive biomarker in both groups.
When the researchers translated the findings from ELISA to the Luminex platform, positive results in synovial fluid for all these biomarkers were also positive in serum samples. Although the differences between persistent and extended-to-be samples did not reach statistical significance using Luminex, the pattern was the same for each biomarker.
“Luminex is more sensitive than ELISA. We believe that conducting an LDA [linear discriminant analysis] using these Luminex measurements will allow us to determine new cutoffs or new protein levels that are appropriate for Luminex to predict who will extend,” Dr. Brescia said. “It’s also our goal to develop a serum panel because ... being able to detect these markers in serum would expand the applicability of these markers to more patients.”
Dr. Brescia then described the group’s work in defining clinically relevant subpopulations of patients based on fibroblast-like synoviocytes (FLS) cells in the synovial intimal lining that produce inflammatory cytokines.
“Our compelling, single-cell, RNA sequencing preliminary data revealing multiple subpopulations within the total FLS population supports our hypothesis that distinct FLS subpopulations correlate with clinical outcome,” said Dr. Brescia. They looked at the percentage of chondrocyte-like, fibroblast-like, and smooth muscle-like subpopulations in samples from patients with oligoarticular JIA, extended-to-be JIA, and polyarticular JIA. Chondrocytes occurred in the largest proportion, and polyarticular JIA FLS had the largest percentage of chondrocytes, compared with the other two subpopulation groups.
“This is a work in progress,” Dr. Brescia said, “so hopefully you’ll hear about it next year.” In response to an attendee’s question, she said she believes identifying reliable biomarkers will eventually lead to refining treatment paradigms.
“I think it will at least change the guidance we can provide parents about making next choices and how quickly to accelerate to those next choices,” Dr. Brescia said. For example, if a child’s serum or synovial fluid has markers that show a very high likelihood of extension, the parent may decide to proceed to the next level medication sooner. “I do think it will push both parents and doctors to be a little more proactive instead of reactive when the poor patient comes back with 13 joints involved when they had just been an oligo for years.”
Dr. Oliver noted the promise of CD14 and IL-6 in potentially predicting which patients’ disease will stay persistent but cautioned that it’s still early in evaluating these biomarkers, especially with the limited patient samples in this study.
“I think these results are promising, and it’s great that there are groups out there working on this,” Dr. Oliver said. “Once we have a reliable, highly sensitive and specific biomarker, that will definitely help providers, parents, and patients be more informed.”
The research was supported by the Open Net Foundation, the Arthritis Foundation, Delaware Community Foundation, the Delaware Clinical and Translational Research (DE-CTR) ACCEL Program, the Nancy Taylor Foundation for Chronic Diseases, and CARRA. Dr. Brescia and Dr. Oliver have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Ongoing research in patients with oligoarticular juvenile idiopathic arthritis (JIA) so far suggests that a set of biomarkers in synovial fluid may help to predict which patients may be more likely to stay with persistent oligoarticular disease rather than progress to polyarticular disease, according to new research presented at the annual scientific meeting of the Childhood Arthritis and Rheumatology Research Alliance, held virtually this year. Identifying biomarkers in synovial fluid or possibly serum could aid families and physicians in being more proactive in treatment protocols, said AnneMarie C. Brescia, MD, of Nemours Children’s Hospital in Wilmington, Del.
“JIA carries the risk of permanent joint damage and disability, which can result when joint involvement evolves from oligoarticular into a polyarticular course, termed extended oligoarticular disease,” Dr. Brescia told attendees. “Since disease progression increases the risk for disability, early prediction of this course is essential.”
This group – those whose oligoarticular disease will begin recruiting joints and ultimately become extended oligoarticular JIA – is “very important because they have been shown to have worse health-related quality of life and greater risk of needing a joint replacement than even polyarticular [JIA],” Dr. Brescia said. “So, our lab has really focused on trying to predict who will fall in this group.”
Melissa Oliver, MD, assistant professor of clinical pediatrics in the division of pediatric rheumatology at Indiana University in Indianapolis, was not involved in the study but agreed that having highly sensitive and specific biomarkers could be particularly helpful in clinical care.
“Biomarkers can help guide treatment decisions and help physicians and their patients share the decision-making about next choices and when to change,” Dr. Oliver told this news organization. “If a provider and parent know that their child has these markers in their serum or synovial fluid that may predict extension of their disease, then they may be more aggressive upfront with therapy.”
The study aimed to determine whether differential levels of synovial fluid proteins could be used to predict whether JIA would evolve into an extended course before it became clinically evident. Although early aggressive treatment is common with rheumatoid arthritis and can lead to remission, JIA treatment paradigms tend to be more reactive, Dr. Brescia said.
“It would be better to switch to proactive, that if we’re able to predict that this patient may have a more difficult course with extension to polyarticular, we could be prepared, we could inform the parents, and it would just help us have a more proactive approach,” she said.
The researchers used antibody arrays to detect the following inflammatory mediators in blinded samples: CD14, interleukin (IL)-1-alpha, IL-3, IL-5, IL-6, vascular endothelial growth factor (VEGF), and angiogenin. They analyzed 37 samples with persistent disease and 32 samples from disease that had not yet extended but would become extended in that patient. The samples came from patients who were taking no medicines or only NSAIDs. The researchers assessed the sensitivity and specificity of each biomarker. Sensitivity referred the biomarker’s ability to correctly indicate that the sample would extend, and specificity referred to the biomarker’s accuracy in determining that the disease in the sample would remain persistent.
Combining samples from cohorts at Nemours Children’s Health (14 persistent and 7 extended-to-be) and Cincinnati Children’s Hospital (23 persistent and 25 extended-to-be) yielded the following results:
The findings revealed that the selected biomarkers were more accurate at predicting whose disease would remain persistent than predicting those that would extend, Dr. Brescia said. CD14 was the most specific biomarker, and IL-6 was the most sensitive biomarker in both groups.
When the researchers translated the findings from ELISA to the Luminex platform, positive results in synovial fluid for all these biomarkers were also positive in serum samples. Although the differences between persistent and extended-to-be samples did not reach statistical significance using Luminex, the pattern was the same for each biomarker.
“Luminex is more sensitive than ELISA. We believe that conducting an LDA [linear discriminant analysis] using these Luminex measurements will allow us to determine new cutoffs or new protein levels that are appropriate for Luminex to predict who will extend,” Dr. Brescia said. “It’s also our goal to develop a serum panel because ... being able to detect these markers in serum would expand the applicability of these markers to more patients.”
Dr. Brescia then described the group’s work in defining clinically relevant subpopulations of patients based on fibroblast-like synoviocytes (FLS) cells in the synovial intimal lining that produce inflammatory cytokines.
“Our compelling, single-cell, RNA sequencing preliminary data revealing multiple subpopulations within the total FLS population supports our hypothesis that distinct FLS subpopulations correlate with clinical outcome,” said Dr. Brescia. They looked at the percentage of chondrocyte-like, fibroblast-like, and smooth muscle-like subpopulations in samples from patients with oligoarticular JIA, extended-to-be JIA, and polyarticular JIA. Chondrocytes occurred in the largest proportion, and polyarticular JIA FLS had the largest percentage of chondrocytes, compared with the other two subpopulation groups.
“This is a work in progress,” Dr. Brescia said, “so hopefully you’ll hear about it next year.” In response to an attendee’s question, she said she believes identifying reliable biomarkers will eventually lead to refining treatment paradigms.
“I think it will at least change the guidance we can provide parents about making next choices and how quickly to accelerate to those next choices,” Dr. Brescia said. For example, if a child’s serum or synovial fluid has markers that show a very high likelihood of extension, the parent may decide to proceed to the next level medication sooner. “I do think it will push both parents and doctors to be a little more proactive instead of reactive when the poor patient comes back with 13 joints involved when they had just been an oligo for years.”
Dr. Oliver noted the promise of CD14 and IL-6 in potentially predicting which patients’ disease will stay persistent but cautioned that it’s still early in evaluating these biomarkers, especially with the limited patient samples in this study.
“I think these results are promising, and it’s great that there are groups out there working on this,” Dr. Oliver said. “Once we have a reliable, highly sensitive and specific biomarker, that will definitely help providers, parents, and patients be more informed.”
The research was supported by the Open Net Foundation, the Arthritis Foundation, Delaware Community Foundation, the Delaware Clinical and Translational Research (DE-CTR) ACCEL Program, the Nancy Taylor Foundation for Chronic Diseases, and CARRA. Dr. Brescia and Dr. Oliver have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CARRA 2022
Updated pediatric uveitis recommendations advise on expanded treatment options
Glucocorticoids should be bridging therapies in the treatment of juvenile idiopathic arthritis–associated uveitis (JIAU) and idiopathic chronic anterior uveitis (CAU), according to recently released recommendations from the Multinational Interdisciplinary Working Group for Uveitis in Childhood (MIWGUC).
The recommendations cover literature from December 2014 to June 2020 and represent an update of previously published treatment guidelines from 2018. The MIWGUC work group that formulated the new recommendations consisted of eight pediatric rheumatologists and eight ophthalmologists with expertise in pediatric uveitis.

One major shift from the previous guidelines is the lack of distinction between JIAU and CAU, said lead author Ivan Foeldvari, MD, head of the Hamburg (Germany) Center for Pediatric and Adolescent Rheumatology.
“We are considering these two conditions equivalent regarding the ophthalmological presentation,” Dr. Foeldvari said in an interview.
These guidelines have also expanded possible treatment options for these conditions in light of data from clinical trials that have pointed to new options, Dr. Foeldvari noted.
The guidelines also present new options, compared with the 2019 American College of Rheumatology/Arthritis Foundation JIA-associated uveitis guideline. The data cutoff for that guideline was 2014. “Many key papers were published since 2014,” Dr. Foeldvari said.
Another major change is in the escalation of therapy, he noted.
“We view glucocorticoids as a bridging agent, which is very important to emphasize,” Dr. Foeldvari said. “We do not want oral glucocorticoids used as a monotherapy. If you consider a child who has severe uveitis and you want to give an oral glucocorticoid treatment, then it should be considered only for bridging. We suggest to start a DMARD [disease-modifying antirheumatic drug].”
The specific recommendation is that methotrexate be the first DMARD that clinicians choose after using glucocorticoids as a bridging therapy; adalimumab is recommended as the next treatment choice for patients who do not respond to methotrexate.
The working group also calls for limited use of topical glucocorticoids in the affected eye, he said.
“We recommend no more than two or three drops long term in the eye, because there are studies that show continuous local therapy is the main reason that children may develop blindness,” Dr. Foeldvari said. “With respect to oral corticosteroids, they have a lot of systemic effects. Those effects include a high risk of infection, weight gain, and growth disturbance.”

The new recommendations can guide treatment decisions for rheumatologists and ophthalmologists alike, according to Daniel J. Lovell, MD, MPH, the Joseph E. Levinson Endowed Chair of Pediatric Rheumatology and professor of pediatrics at the University of Cincinnati and Cincinnati Children’s Hospital Medical Center. He was one of the authors of the 2019 ACR/Arthritis Foundation guideline.
“We [rheumatologists] comanage these patients with ophthalmologists,” Dr. Lovell said in an interview. “Ophthalmologists are oftentimes not as experienced in using biologics or methotrexate in terms of monitoring for safety and dosing.”
Dr. Lovell pointed out that the key message from this set of recommendations is to curb the use of topical steroids.
“Topical steroids should be used sparingly and as monotherapy for a very short period of time,” Dr. Lovell said. “Any guidelines agree that if eye inflammation is still present at 3 months, we need to move beyond topical steroid monotherapy.”
These new recommendations from MIWGUC are fairly consistent with the 2019 ACR/Arthritis Foundation guideline, he noted.
“The differences are very minor,” Dr. Lovell said. “In both instances, systemic corticosteroids should be bridging therapy. If you have a patient who needs systemic corticosteroids in addition to topical at the same time, you should be talking about adding other anti-inflammatory treatments, such as traditional and/or biologic DMARDs. Both MIWGUC and the ACR guidelines agree on that.”
The 2019 ACR/Arthritis Foundation guideline did not mention rituximab as an option, nor Janus kinase (JAK) inhibitors, Dr. Lovell said, noting there was no literature on JAK inhibitors as a possible option for JIAU when the guideline was being formulated.
Both sets of guidelines point out that there is a dearth of literature with respect to determining the safe dose of maintenance topical corticosteroids, Dr. Lovell said.
“The ACR 2019 guidelines state you should add systemic therapy if there is persistent eye inflammation despite use of up to two drops per day of topical corticosteroids, while the European [MIWGUC] guideline states you can allow up to three drops,” he said. “In both instances, they are quoting the same two sources. Both guidelines indicate that the literature is very scant as to defining a true, safe dose of topical ocular corticosteroids. They differ by one drop allowed per day. In both instances, in the presence of active uveitis, at 3 months on topical steroid monotherapy, both [guidelines] strongly recommend adding systemic therapy.”

Marinka Twilt, MD, MSCE, PhD, associate professor in the department of pediatrics at the University of Calgary (Alta.), noted in an interview that these latest recommendations from MIWGUC have included consensus views on what to do if certain medications fail to lead to remission, which is not addressed in the 2019 ACR/Arthritis Foundation guideline.
“The new manuscript provides consensus on the use of abatacept, JAK inhibitors, and rituximab if patients are refractory to adalimumab and tocilizumab, which is not discussed in the 2019 recommendations,” Dr. Twilt said.
She also pointed out that these recommendations suggest adalimumab as treatment before infliximab, whereas the 2019 guideline did not recommend using one or the other first.
In compiling the recommendations, the authors received no outside financial support. Dr. Foeldvari is a member of advisory boards for Lilly, Pfizer, Novartis, and Medac. Dr. Lovell and Dr. Twilt disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Glucocorticoids should be bridging therapies in the treatment of juvenile idiopathic arthritis–associated uveitis (JIAU) and idiopathic chronic anterior uveitis (CAU), according to recently released recommendations from the Multinational Interdisciplinary Working Group for Uveitis in Childhood (MIWGUC).
The recommendations cover literature from December 2014 to June 2020 and represent an update of previously published treatment guidelines from 2018. The MIWGUC work group that formulated the new recommendations consisted of eight pediatric rheumatologists and eight ophthalmologists with expertise in pediatric uveitis.
One major shift from the previous guidelines is the lack of distinction between JIAU and CAU, said lead author Ivan Foeldvari, MD, head of the Hamburg (Germany) Center for Pediatric and Adolescent Rheumatology.
“We are considering these two conditions equivalent regarding the ophthalmological presentation,” Dr. Foeldvari said in an interview.
These guidelines have also expanded possible treatment options for these conditions in light of data from clinical trials that have pointed to new options, Dr. Foeldvari noted.
The guidelines also present new options, compared with the 2019 American College of Rheumatology/Arthritis Foundation JIA-associated uveitis guideline. The data cutoff for that guideline was 2014. “Many key papers were published since 2014,” Dr. Foeldvari said.
Another major change is in the escalation of therapy, he noted.
“We view glucocorticoids as a bridging agent, which is very important to emphasize,” Dr. Foeldvari said. “We do not want oral glucocorticoids used as a monotherapy. If you consider a child who has severe uveitis and you want to give an oral glucocorticoid treatment, then it should be considered only for bridging. We suggest to start a DMARD [disease-modifying antirheumatic drug].”
The specific recommendation is that methotrexate be the first DMARD that clinicians choose after using glucocorticoids as a bridging therapy; adalimumab is recommended as the next treatment choice for patients who do not respond to methotrexate.
The working group also calls for limited use of topical glucocorticoids in the affected eye, he said.
“We recommend no more than two or three drops long term in the eye, because there are studies that show continuous local therapy is the main reason that children may develop blindness,” Dr. Foeldvari said. “With respect to oral corticosteroids, they have a lot of systemic effects. Those effects include a high risk of infection, weight gain, and growth disturbance.”
The new recommendations can guide treatment decisions for rheumatologists and ophthalmologists alike, according to Daniel J. Lovell, MD, MPH, the Joseph E. Levinson Endowed Chair of Pediatric Rheumatology and professor of pediatrics at the University of Cincinnati and Cincinnati Children’s Hospital Medical Center. He was one of the authors of the 2019 ACR/Arthritis Foundation guideline.
“We [rheumatologists] comanage these patients with ophthalmologists,” Dr. Lovell said in an interview. “Ophthalmologists are oftentimes not as experienced in using biologics or methotrexate in terms of monitoring for safety and dosing.”
Dr. Lovell pointed out that the key message from this set of recommendations is to curb the use of topical steroids.
“Topical steroids should be used sparingly and as monotherapy for a very short period of time,” Dr. Lovell said. “Any guidelines agree that if eye inflammation is still present at 3 months, we need to move beyond topical steroid monotherapy.”
These new recommendations from MIWGUC are fairly consistent with the 2019 ACR/Arthritis Foundation guideline, he noted.
“The differences are very minor,” Dr. Lovell said. “In both instances, systemic corticosteroids should be bridging therapy. If you have a patient who needs systemic corticosteroids in addition to topical at the same time, you should be talking about adding other anti-inflammatory treatments, such as traditional and/or biologic DMARDs. Both MIWGUC and the ACR guidelines agree on that.”
The 2019 ACR/Arthritis Foundation guideline did not mention rituximab as an option, nor Janus kinase (JAK) inhibitors, Dr. Lovell said, noting there was no literature on JAK inhibitors as a possible option for JIAU when the guideline was being formulated.
Both sets of guidelines point out that there is a dearth of literature with respect to determining the safe dose of maintenance topical corticosteroids, Dr. Lovell said.
“The ACR 2019 guidelines state you should add systemic therapy if there is persistent eye inflammation despite use of up to two drops per day of topical corticosteroids, while the European [MIWGUC] guideline states you can allow up to three drops,” he said. “In both instances, they are quoting the same two sources. Both guidelines indicate that the literature is very scant as to defining a true, safe dose of topical ocular corticosteroids. They differ by one drop allowed per day. In both instances, in the presence of active uveitis, at 3 months on topical steroid monotherapy, both [guidelines] strongly recommend adding systemic therapy.”
Marinka Twilt, MD, MSCE, PhD, associate professor in the department of pediatrics at the University of Calgary (Alta.), noted in an interview that these latest recommendations from MIWGUC have included consensus views on what to do if certain medications fail to lead to remission, which is not addressed in the 2019 ACR/Arthritis Foundation guideline.
“The new manuscript provides consensus on the use of abatacept, JAK inhibitors, and rituximab if patients are refractory to adalimumab and tocilizumab, which is not discussed in the 2019 recommendations,” Dr. Twilt said.
She also pointed out that these recommendations suggest adalimumab as treatment before infliximab, whereas the 2019 guideline did not recommend using one or the other first.
In compiling the recommendations, the authors received no outside financial support. Dr. Foeldvari is a member of advisory boards for Lilly, Pfizer, Novartis, and Medac. Dr. Lovell and Dr. Twilt disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Glucocorticoids should be bridging therapies in the treatment of juvenile idiopathic arthritis–associated uveitis (JIAU) and idiopathic chronic anterior uveitis (CAU), according to recently released recommendations from the Multinational Interdisciplinary Working Group for Uveitis in Childhood (MIWGUC).
The recommendations cover literature from December 2014 to June 2020 and represent an update of previously published treatment guidelines from 2018. The MIWGUC work group that formulated the new recommendations consisted of eight pediatric rheumatologists and eight ophthalmologists with expertise in pediatric uveitis.
One major shift from the previous guidelines is the lack of distinction between JIAU and CAU, said lead author Ivan Foeldvari, MD, head of the Hamburg (Germany) Center for Pediatric and Adolescent Rheumatology.
“We are considering these two conditions equivalent regarding the ophthalmological presentation,” Dr. Foeldvari said in an interview.
These guidelines have also expanded possible treatment options for these conditions in light of data from clinical trials that have pointed to new options, Dr. Foeldvari noted.
The guidelines also present new options, compared with the 2019 American College of Rheumatology/Arthritis Foundation JIA-associated uveitis guideline. The data cutoff for that guideline was 2014. “Many key papers were published since 2014,” Dr. Foeldvari said.
Another major change is in the escalation of therapy, he noted.
“We view glucocorticoids as a bridging agent, which is very important to emphasize,” Dr. Foeldvari said. “We do not want oral glucocorticoids used as a monotherapy. If you consider a child who has severe uveitis and you want to give an oral glucocorticoid treatment, then it should be considered only for bridging. We suggest to start a DMARD [disease-modifying antirheumatic drug].”
The specific recommendation is that methotrexate be the first DMARD that clinicians choose after using glucocorticoids as a bridging therapy; adalimumab is recommended as the next treatment choice for patients who do not respond to methotrexate.
The working group also calls for limited use of topical glucocorticoids in the affected eye, he said.
“We recommend no more than two or three drops long term in the eye, because there are studies that show continuous local therapy is the main reason that children may develop blindness,” Dr. Foeldvari said. “With respect to oral corticosteroids, they have a lot of systemic effects. Those effects include a high risk of infection, weight gain, and growth disturbance.”
The new recommendations can guide treatment decisions for rheumatologists and ophthalmologists alike, according to Daniel J. Lovell, MD, MPH, the Joseph E. Levinson Endowed Chair of Pediatric Rheumatology and professor of pediatrics at the University of Cincinnati and Cincinnati Children’s Hospital Medical Center. He was one of the authors of the 2019 ACR/Arthritis Foundation guideline.
“We [rheumatologists] comanage these patients with ophthalmologists,” Dr. Lovell said in an interview. “Ophthalmologists are oftentimes not as experienced in using biologics or methotrexate in terms of monitoring for safety and dosing.”
Dr. Lovell pointed out that the key message from this set of recommendations is to curb the use of topical steroids.
“Topical steroids should be used sparingly and as monotherapy for a very short period of time,” Dr. Lovell said. “Any guidelines agree that if eye inflammation is still present at 3 months, we need to move beyond topical steroid monotherapy.”
These new recommendations from MIWGUC are fairly consistent with the 2019 ACR/Arthritis Foundation guideline, he noted.
“The differences are very minor,” Dr. Lovell said. “In both instances, systemic corticosteroids should be bridging therapy. If you have a patient who needs systemic corticosteroids in addition to topical at the same time, you should be talking about adding other anti-inflammatory treatments, such as traditional and/or biologic DMARDs. Both MIWGUC and the ACR guidelines agree on that.”
The 2019 ACR/Arthritis Foundation guideline did not mention rituximab as an option, nor Janus kinase (JAK) inhibitors, Dr. Lovell said, noting there was no literature on JAK inhibitors as a possible option for JIAU when the guideline was being formulated.
Both sets of guidelines point out that there is a dearth of literature with respect to determining the safe dose of maintenance topical corticosteroids, Dr. Lovell said.
“The ACR 2019 guidelines state you should add systemic therapy if there is persistent eye inflammation despite use of up to two drops per day of topical corticosteroids, while the European [MIWGUC] guideline states you can allow up to three drops,” he said. “In both instances, they are quoting the same two sources. Both guidelines indicate that the literature is very scant as to defining a true, safe dose of topical ocular corticosteroids. They differ by one drop allowed per day. In both instances, in the presence of active uveitis, at 3 months on topical steroid monotherapy, both [guidelines] strongly recommend adding systemic therapy.”
Marinka Twilt, MD, MSCE, PhD, associate professor in the department of pediatrics at the University of Calgary (Alta.), noted in an interview that these latest recommendations from MIWGUC have included consensus views on what to do if certain medications fail to lead to remission, which is not addressed in the 2019 ACR/Arthritis Foundation guideline.
“The new manuscript provides consensus on the use of abatacept, JAK inhibitors, and rituximab if patients are refractory to adalimumab and tocilizumab, which is not discussed in the 2019 recommendations,” Dr. Twilt said.
She also pointed out that these recommendations suggest adalimumab as treatment before infliximab, whereas the 2019 guideline did not recommend using one or the other first.
In compiling the recommendations, the authors received no outside financial support. Dr. Foeldvari is a member of advisory boards for Lilly, Pfizer, Novartis, and Medac. Dr. Lovell and Dr. Twilt disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ARTHRITIS CARE RESEARCH
Microbiome’s new happy place: The beer gut
Your gut microbiome will thank you later
A healthy gut seems like the new catch-all to better overall health these days. Nutrition and diet culture has us drinking kombucha and ginger tea and coffee, but what if we told you that going to happy hour might also help?
In a recent double-blind study published in the Journal of Agricultural and Food Chemistry, 19 men were divided into two groups and asked to drink 11 ounces of alcoholic lager (5.2% by volume) or nonalcoholic lager with dinner for 4 weeks.
Beer? Yes. Beer.
We humans have trillions of microorganisms running rampant through our digestive tracts. When they’re happy, we have a lower chance of developing heart disease and diabetes. You know what else has millions of happy microorganisms from fermentation? Beer. It also has polyphenols that can help the body’s tissues fight cancers, as well as heart disease and inflammation. So beer is looking a little more healthy now, isn’t it?
In the study, the researchers found that both the alcoholic- and nonalcoholic-lager groups had a boost in bacterial diversity in the gut and higher fecal alkaline phosphatase levels, which showed improved intestinal health. They acknowledged, however, that the nonalcoholic route would be safer and healthier for overall health.
So add a lager to the list of gut-healthy foods that you should be consuming. It may give the phrase “beer gut” a whole new meaning.
We’ve lost our minds, but at least we know how fast they’re going
The phrase “quantum consciousness” sounds like something out of a particularly cheesy episode of Star Trek: “Oh no, Captain, the quantum consciousness has invaded our computer, and the only way to drive it out is to reverse the polarity of a focused tachyon beam.”
When it comes to understanding such basic existential issues as the origin of consciousness, however, quantum mechanics wasn’t off the table. The theory of the quantum origin of consciousness dates back to the 1990s (thanks in part to noted physician Roger Penrose), and goes something like this: There are microtubules within neurons in the brain that are small enough and isolated enough from the warm, wet, and chaotic brain environment where quantum effects can briefly come into play. We’re talking miniscule fractions of a second here, but still, long enough for quantum calculations to take place in the form of system wavefunction collapse, courtesy of gravity.
To plunge even deeper into the rabbit hole of quantum mechanics, the reason Schrödinger’s cat doesn’t occur in real life is wavefunction collapse; the more massive a quantum system is, the more likely it is to collapse into one state or another (alive or dead, in the cat’s case). The quantum origin of consciousness, or Orch OR theory, holds that human consciousness arises from electrical oscillations within the neuronal microtubules caused by the computations stemming from the collapse of small quantum systems.
That is an awful lot of overly simplified explanation, especially considering the study that just came out essentially disproved it. Oops. The research, published in Physics of Life Reviews, is pretty simple. The researchers went to a lab deep underground to avoid interference from cosmic rays, and sat around for months, observing a chunk of germanium for signs of spontaneous radiation, attributable to the same sort of wavefunction collapse that is supposedly occurring in our brains. They found nothing out of the ordinary, pretty definitively disproving most of Orch OR theory.
The researchers were unwilling to completely dismiss the idea (this is quantum mechanics, after all, uncertainty kind of goes with the territory), but it does seem like we’ll have to search elsewhere for sources of human consciousness. Personally, we’re big fans of the cymbal-playing monkey.
Missing links: A real fish story
Dear LOTME:
Ear’s a question that’s been keeping me up at night. Is the human middle ear the result of top-secret government experiments involving alien technology, Abraham Lincoln, and the Illuminati?
Restless in Roswell
Dear Restless:
The paleoanthropologic community has been sorting through this mystery for decades, and fossils discovered in China over the past 20 years finally provide a much less conspiratorially satisfying answer.

For some time now, experts in the field have believed that the bones of the human middle ear evolved from the spiracular gill of a fish. The spiracle is a small hole behind each eye that opens to the mouth in some fishes and was used to breathe air in the earliest, most primitive species. But how did we get from spiracle to ear?
The missing links come in the form of the cranial anatomy of Shuyu, a 438-million-year-old, fingernail-sized skull of a jawless fish, and the 419-million-year-old fossil of a completely preserved fish with gill filaments in the first branchial chamber.
“These fossils provided the first anatomical and fossil evidence for a vertebrate spiracle originating from fish gills,” senior author Gai Zhikun, PhD, of the Institute of Vertebrate Paleontology and Paleoanthropology, Beijing, said in a written statement.
In many ways, it seems, we are fish: “Many important structures of human beings can be traced back to our fish ancestors, such as our teeth, jaws, middle ears, etc,” added Zhu Min, PhD, also of the institute.
So, Restless, the next time you hear the soothing sounds of an angry mob storming the Capitol or you chew on a slab, slice, or chunk of mutant, laboratory-produced chicken in your favorite fast-food restaurant, be sure to thank Shuyu.
Can you lend me an ear?
If you thought locusts were only a nuisance, think again. They have their uses. If you take a locust’s ear and put it inside a robot, the robot will be able to hear and receive signals. Who knew?
Researchers from Tel Aviv University in Israel showed the robot’s hearing abilities by giving clap signals that told the robot what to do: One clap means go forward, two claps mean move back. What do you think the robot would do if it heard the clap break from Cha Cha Slide?
“Our task was to replace the robot’s electronic microphone with a dead insect’s ear, use the ear’s ability to detect the electrical signals from the environment, in this case vibrations in the air, and, using a special chip, convert the insect input to that of the robot,” Ben M. Maoz, PhD, said in a statement from the university.
And how does a dead locust ear work in a robot? Well, Dr. Maoz explained: “My laboratory has developed a special device – Ear-on-a-Chip – that allows the ear to be kept alive throughout the experiment by supplying oxygen and food to the organ while allowing the electrical signals to be taken out of the locust’s ear and amplified and transmitted to the robot.”
The research won’t stop at hearing, he said, as the other four senses also will be taken into consideration. This could help us sense dangers in the future, such as earthquakes or diseases. We said it before and we’ll say it again: We’re rooting for you, science!
Your gut microbiome will thank you later
A healthy gut seems like the new catch-all to better overall health these days. Nutrition and diet culture has us drinking kombucha and ginger tea and coffee, but what if we told you that going to happy hour might also help?
In a recent double-blind study published in the Journal of Agricultural and Food Chemistry, 19 men were divided into two groups and asked to drink 11 ounces of alcoholic lager (5.2% by volume) or nonalcoholic lager with dinner for 4 weeks.
Beer? Yes. Beer.
We humans have trillions of microorganisms running rampant through our digestive tracts. When they’re happy, we have a lower chance of developing heart disease and diabetes. You know what else has millions of happy microorganisms from fermentation? Beer. It also has polyphenols that can help the body’s tissues fight cancers, as well as heart disease and inflammation. So beer is looking a little more healthy now, isn’t it?
In the study, the researchers found that both the alcoholic- and nonalcoholic-lager groups had a boost in bacterial diversity in the gut and higher fecal alkaline phosphatase levels, which showed improved intestinal health. They acknowledged, however, that the nonalcoholic route would be safer and healthier for overall health.
So add a lager to the list of gut-healthy foods that you should be consuming. It may give the phrase “beer gut” a whole new meaning.
We’ve lost our minds, but at least we know how fast they’re going
The phrase “quantum consciousness” sounds like something out of a particularly cheesy episode of Star Trek: “Oh no, Captain, the quantum consciousness has invaded our computer, and the only way to drive it out is to reverse the polarity of a focused tachyon beam.”
When it comes to understanding such basic existential issues as the origin of consciousness, however, quantum mechanics wasn’t off the table. The theory of the quantum origin of consciousness dates back to the 1990s (thanks in part to noted physician Roger Penrose), and goes something like this: There are microtubules within neurons in the brain that are small enough and isolated enough from the warm, wet, and chaotic brain environment where quantum effects can briefly come into play. We’re talking miniscule fractions of a second here, but still, long enough for quantum calculations to take place in the form of system wavefunction collapse, courtesy of gravity.
To plunge even deeper into the rabbit hole of quantum mechanics, the reason Schrödinger’s cat doesn’t occur in real life is wavefunction collapse; the more massive a quantum system is, the more likely it is to collapse into one state or another (alive or dead, in the cat’s case). The quantum origin of consciousness, or Orch OR theory, holds that human consciousness arises from electrical oscillations within the neuronal microtubules caused by the computations stemming from the collapse of small quantum systems.
That is an awful lot of overly simplified explanation, especially considering the study that just came out essentially disproved it. Oops. The research, published in Physics of Life Reviews, is pretty simple. The researchers went to a lab deep underground to avoid interference from cosmic rays, and sat around for months, observing a chunk of germanium for signs of spontaneous radiation, attributable to the same sort of wavefunction collapse that is supposedly occurring in our brains. They found nothing out of the ordinary, pretty definitively disproving most of Orch OR theory.
The researchers were unwilling to completely dismiss the idea (this is quantum mechanics, after all, uncertainty kind of goes with the territory), but it does seem like we’ll have to search elsewhere for sources of human consciousness. Personally, we’re big fans of the cymbal-playing monkey.
Missing links: A real fish story
Dear LOTME:
Ear’s a question that’s been keeping me up at night. Is the human middle ear the result of top-secret government experiments involving alien technology, Abraham Lincoln, and the Illuminati?
Restless in Roswell
Dear Restless:
The paleoanthropologic community has been sorting through this mystery for decades, and fossils discovered in China over the past 20 years finally provide a much less conspiratorially satisfying answer.
For some time now, experts in the field have believed that the bones of the human middle ear evolved from the spiracular gill of a fish. The spiracle is a small hole behind each eye that opens to the mouth in some fishes and was used to breathe air in the earliest, most primitive species. But how did we get from spiracle to ear?
The missing links come in the form of the cranial anatomy of Shuyu, a 438-million-year-old, fingernail-sized skull of a jawless fish, and the 419-million-year-old fossil of a completely preserved fish with gill filaments in the first branchial chamber.
“These fossils provided the first anatomical and fossil evidence for a vertebrate spiracle originating from fish gills,” senior author Gai Zhikun, PhD, of the Institute of Vertebrate Paleontology and Paleoanthropology, Beijing, said in a written statement.
In many ways, it seems, we are fish: “Many important structures of human beings can be traced back to our fish ancestors, such as our teeth, jaws, middle ears, etc,” added Zhu Min, PhD, also of the institute.
So, Restless, the next time you hear the soothing sounds of an angry mob storming the Capitol or you chew on a slab, slice, or chunk of mutant, laboratory-produced chicken in your favorite fast-food restaurant, be sure to thank Shuyu.
Can you lend me an ear?
If you thought locusts were only a nuisance, think again. They have their uses. If you take a locust’s ear and put it inside a robot, the robot will be able to hear and receive signals. Who knew?
Researchers from Tel Aviv University in Israel showed the robot’s hearing abilities by giving clap signals that told the robot what to do: One clap means go forward, two claps mean move back. What do you think the robot would do if it heard the clap break from Cha Cha Slide?
“Our task was to replace the robot’s electronic microphone with a dead insect’s ear, use the ear’s ability to detect the electrical signals from the environment, in this case vibrations in the air, and, using a special chip, convert the insect input to that of the robot,” Ben M. Maoz, PhD, said in a statement from the university.
And how does a dead locust ear work in a robot? Well, Dr. Maoz explained: “My laboratory has developed a special device – Ear-on-a-Chip – that allows the ear to be kept alive throughout the experiment by supplying oxygen and food to the organ while allowing the electrical signals to be taken out of the locust’s ear and amplified and transmitted to the robot.”
The research won’t stop at hearing, he said, as the other four senses also will be taken into consideration. This could help us sense dangers in the future, such as earthquakes or diseases. We said it before and we’ll say it again: We’re rooting for you, science!
Your gut microbiome will thank you later
A healthy gut seems like the new catch-all to better overall health these days. Nutrition and diet culture has us drinking kombucha and ginger tea and coffee, but what if we told you that going to happy hour might also help?
In a recent double-blind study published in the Journal of Agricultural and Food Chemistry, 19 men were divided into two groups and asked to drink 11 ounces of alcoholic lager (5.2% by volume) or nonalcoholic lager with dinner for 4 weeks.
Beer? Yes. Beer.
We humans have trillions of microorganisms running rampant through our digestive tracts. When they’re happy, we have a lower chance of developing heart disease and diabetes. You know what else has millions of happy microorganisms from fermentation? Beer. It also has polyphenols that can help the body’s tissues fight cancers, as well as heart disease and inflammation. So beer is looking a little more healthy now, isn’t it?
In the study, the researchers found that both the alcoholic- and nonalcoholic-lager groups had a boost in bacterial diversity in the gut and higher fecal alkaline phosphatase levels, which showed improved intestinal health. They acknowledged, however, that the nonalcoholic route would be safer and healthier for overall health.
So add a lager to the list of gut-healthy foods that you should be consuming. It may give the phrase “beer gut” a whole new meaning.
We’ve lost our minds, but at least we know how fast they’re going
The phrase “quantum consciousness” sounds like something out of a particularly cheesy episode of Star Trek: “Oh no, Captain, the quantum consciousness has invaded our computer, and the only way to drive it out is to reverse the polarity of a focused tachyon beam.”
When it comes to understanding such basic existential issues as the origin of consciousness, however, quantum mechanics wasn’t off the table. The theory of the quantum origin of consciousness dates back to the 1990s (thanks in part to noted physician Roger Penrose), and goes something like this: There are microtubules within neurons in the brain that are small enough and isolated enough from the warm, wet, and chaotic brain environment where quantum effects can briefly come into play. We’re talking miniscule fractions of a second here, but still, long enough for quantum calculations to take place in the form of system wavefunction collapse, courtesy of gravity.
To plunge even deeper into the rabbit hole of quantum mechanics, the reason Schrödinger’s cat doesn’t occur in real life is wavefunction collapse; the more massive a quantum system is, the more likely it is to collapse into one state or another (alive or dead, in the cat’s case). The quantum origin of consciousness, or Orch OR theory, holds that human consciousness arises from electrical oscillations within the neuronal microtubules caused by the computations stemming from the collapse of small quantum systems.
That is an awful lot of overly simplified explanation, especially considering the study that just came out essentially disproved it. Oops. The research, published in Physics of Life Reviews, is pretty simple. The researchers went to a lab deep underground to avoid interference from cosmic rays, and sat around for months, observing a chunk of germanium for signs of spontaneous radiation, attributable to the same sort of wavefunction collapse that is supposedly occurring in our brains. They found nothing out of the ordinary, pretty definitively disproving most of Orch OR theory.
The researchers were unwilling to completely dismiss the idea (this is quantum mechanics, after all, uncertainty kind of goes with the territory), but it does seem like we’ll have to search elsewhere for sources of human consciousness. Personally, we’re big fans of the cymbal-playing monkey.
Missing links: A real fish story
Dear LOTME:
Ear’s a question that’s been keeping me up at night. Is the human middle ear the result of top-secret government experiments involving alien technology, Abraham Lincoln, and the Illuminati?
Restless in Roswell
Dear Restless:
The paleoanthropologic community has been sorting through this mystery for decades, and fossils discovered in China over the past 20 years finally provide a much less conspiratorially satisfying answer.
For some time now, experts in the field have believed that the bones of the human middle ear evolved from the spiracular gill of a fish. The spiracle is a small hole behind each eye that opens to the mouth in some fishes and was used to breathe air in the earliest, most primitive species. But how did we get from spiracle to ear?
The missing links come in the form of the cranial anatomy of Shuyu, a 438-million-year-old, fingernail-sized skull of a jawless fish, and the 419-million-year-old fossil of a completely preserved fish with gill filaments in the first branchial chamber.
“These fossils provided the first anatomical and fossil evidence for a vertebrate spiracle originating from fish gills,” senior author Gai Zhikun, PhD, of the Institute of Vertebrate Paleontology and Paleoanthropology, Beijing, said in a written statement.
In many ways, it seems, we are fish: “Many important structures of human beings can be traced back to our fish ancestors, such as our teeth, jaws, middle ears, etc,” added Zhu Min, PhD, also of the institute.
So, Restless, the next time you hear the soothing sounds of an angry mob storming the Capitol or you chew on a slab, slice, or chunk of mutant, laboratory-produced chicken in your favorite fast-food restaurant, be sure to thank Shuyu.
Can you lend me an ear?
If you thought locusts were only a nuisance, think again. They have their uses. If you take a locust’s ear and put it inside a robot, the robot will be able to hear and receive signals. Who knew?
Researchers from Tel Aviv University in Israel showed the robot’s hearing abilities by giving clap signals that told the robot what to do: One clap means go forward, two claps mean move back. What do you think the robot would do if it heard the clap break from Cha Cha Slide?
“Our task was to replace the robot’s electronic microphone with a dead insect’s ear, use the ear’s ability to detect the electrical signals from the environment, in this case vibrations in the air, and, using a special chip, convert the insect input to that of the robot,” Ben M. Maoz, PhD, said in a statement from the university.
And how does a dead locust ear work in a robot? Well, Dr. Maoz explained: “My laboratory has developed a special device – Ear-on-a-Chip – that allows the ear to be kept alive throughout the experiment by supplying oxygen and food to the organ while allowing the electrical signals to be taken out of the locust’s ear and amplified and transmitted to the robot.”
The research won’t stop at hearing, he said, as the other four senses also will be taken into consideration. This could help us sense dangers in the future, such as earthquakes or diseases. We said it before and we’ll say it again: We’re rooting for you, science!
Bimekizumab calms psoriatic arthritis in phase 3 ‘BE’ trials
COPENHAGEN – For patients with active psoriatic arthritis for whom tumor necrosis factor (TNF) inhibitors failed to produce an adequate response, use of the dual interleukin-17 (IL-17) inhibitor bimekizumab (Bimzelx) was associated with significant improvement in joint, skin, and health-related quality-of-life parameters, compared with placebo, reported investigators in the phase 3, double-blind, randomized BE COMPLETE trial.
The primary endpoint, which was the percentage of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks, was achieved in 43.4% of patients assigned to receive bimekizumab 160 mg every 4 weeks, compared with 6.8% among patients who received placebo, reported Joseph F. Merola, MD, a dermatologist and rheumatologist at Brigham and Women’s Hospital in Boston.

“The high-level and exciting take-home [message is] that BE COMPLETE did meet all primary and all ranked secondary endpoints at week 16,” he said at the annual European Congress of Rheumatology.
Also at the congress, Iain McInnes, MD, PhD, of the Institute of Infection, Immunity, and Inflammation at the University of Glasgow, Scotland, presented data from a second phase 3, double-blind, randomized trial called BE OPTIMAL that showed similar benefits for patients with psoriatic arthritis who had not previously received biologic disease-modifying antirheumatic drugs.

“This is a new mode of action, inhibiting two cytokines simultaneously,” he said in a late-breaking oral abstract session.
As previously reported by this news organization, use of bimekizumab led to rapid reductions in signs and symptoms of radiographic axial spondyloarthritis in the phase 3 trial called BE MOBILE 2.
Bimekizumab is a monoclonal immunoglobulin G1 antibody that selectively inhibits IL-17A and IL-17F. It is approved in the European Union for treating adults with moderate to severe plaque psoriasis.
BE COMPLETE efficacy
Inclusion criteria comprised adult-onset psoriatic arthritis meeting Classification Criteria for Psoriatic Arthritis (CASPAR) for at least 6 months; tender and swollen joint counts of at least 3/68; one or more active psoriatic lesions; and/or a documented history of psoriasis characterized by intolerance to one or two TNF inhibitors or failure of TNF inhibitors. Patients were randomly assigned in a 2:1 ratio to receive either bimekizumab 160 mg every 4 weeks (n = 267) or placebo (n = 133) for 16 weeks.
Some participants are being followed in the extension BE VITAL study, which will evaluate response to treatment and long-term safety. Patients who do enroll in the extension study will be followed for safety for a period of 20 weeks after the last dose.
As noted before, the trial met its primary endpoint of a significant improvement over placebo in ACR50 (hazard ratio, 11.1; P < .001).
In addition, the trial met all ranked secondary endpoints, including the Health Assessment Questionnaire–Disability Index change from baseline, 90% improvement in the Psoriasis Area and Severity Index (PASI90), Short-Form 36-Item Health Survey, and minimal disease activity (P < .001 for all comparisons).
Improvement with bimekizumab was rapid; curves began to separate from placebo by week 4, Dr. Merola said.
BE OPTIMAL efficacy
In this study, which had the same eligibility criteria as BE COMPLETE, patients were randomly assigned in a 2:3:1 ratio to receive 16 weeks of treatment with either placebo, bimekizumab 160 mg every 4 weeks, or adalimumab 40 mg every 2 weeks as a reference treatment.
This trial also met its primary and ranked secondary endpoints, which were similar to those of BE COMPLETE but also included measures of pooled resolution of enthesitis and dactylitis and change from baseline in van der Heijde modified total Sharp score (P < .001 for all comparisons).
In all, 43.9% of patients who received bimekizumab and 45.7% who received adalimumab achieved ACR50 at week 16, compared with 10% of patients who received placebo. The difference between the placebo and bimekizumab groups was significant (P < .001).
Safety
More patients who received the two active agents in this trial had treatment-emergent adverse events (TEAEs) in comparison with those in the placebo arm, but the incidence of serious TEAEs was less than 2% in each arm.
The most frequent events were nasopharyngitis, upper respiratory tract infection, headache, diarrhea, and hypertension.
Patients tolerated bimekizumab well, and there were no unexpected safety signals, Dr. McInnes said.
Clues to efficacy
In the question-and-answer session following Dr. McInnes’ presentation, Ronald Van Vollenhoven, MD, of the University of Amsterdam, said, “I have a question that is sort of generic in studies of psoriatic arthritis, so it does not only apply to this study, but the skin responses seem to be excellent – PASI90 sounds wonderful – but given that this is the case, is it reasonable to claim that the study is double-blinded in respect to the joints?”
Dr. McInnes replied that while he has considered this conundrum for many years in trials of drugs for psoriatic arthritis, “it doesn’t seem to be a major determinant of the outcome.”
The studies were supported by UCB Pharma. Dr. Merola and Dr. McInnes have consulted for UCB and other pharmaceutical companies that market drugs for psoriatic arthritis and psoriasis. Dr. Van Vollenhoven has received research support, has consulted for, and has spoken on behalf of UCB and other pharmaceutical companies.
A version of this article first appeared on Medscape.com.
COPENHAGEN – For patients with active psoriatic arthritis for whom tumor necrosis factor (TNF) inhibitors failed to produce an adequate response, use of the dual interleukin-17 (IL-17) inhibitor bimekizumab (Bimzelx) was associated with significant improvement in joint, skin, and health-related quality-of-life parameters, compared with placebo, reported investigators in the phase 3, double-blind, randomized BE COMPLETE trial.
The primary endpoint, which was the percentage of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks, was achieved in 43.4% of patients assigned to receive bimekizumab 160 mg every 4 weeks, compared with 6.8% among patients who received placebo, reported Joseph F. Merola, MD, a dermatologist and rheumatologist at Brigham and Women’s Hospital in Boston.
“The high-level and exciting take-home [message is] that BE COMPLETE did meet all primary and all ranked secondary endpoints at week 16,” he said at the annual European Congress of Rheumatology.
Also at the congress, Iain McInnes, MD, PhD, of the Institute of Infection, Immunity, and Inflammation at the University of Glasgow, Scotland, presented data from a second phase 3, double-blind, randomized trial called BE OPTIMAL that showed similar benefits for patients with psoriatic arthritis who had not previously received biologic disease-modifying antirheumatic drugs.
“This is a new mode of action, inhibiting two cytokines simultaneously,” he said in a late-breaking oral abstract session.
As previously reported by this news organization, use of bimekizumab led to rapid reductions in signs and symptoms of radiographic axial spondyloarthritis in the phase 3 trial called BE MOBILE 2.
Bimekizumab is a monoclonal immunoglobulin G1 antibody that selectively inhibits IL-17A and IL-17F. It is approved in the European Union for treating adults with moderate to severe plaque psoriasis.
BE COMPLETE efficacy
Inclusion criteria comprised adult-onset psoriatic arthritis meeting Classification Criteria for Psoriatic Arthritis (CASPAR) for at least 6 months; tender and swollen joint counts of at least 3/68; one or more active psoriatic lesions; and/or a documented history of psoriasis characterized by intolerance to one or two TNF inhibitors or failure of TNF inhibitors. Patients were randomly assigned in a 2:1 ratio to receive either bimekizumab 160 mg every 4 weeks (n = 267) or placebo (n = 133) for 16 weeks.
Some participants are being followed in the extension BE VITAL study, which will evaluate response to treatment and long-term safety. Patients who do enroll in the extension study will be followed for safety for a period of 20 weeks after the last dose.
As noted before, the trial met its primary endpoint of a significant improvement over placebo in ACR50 (hazard ratio, 11.1; P < .001).
In addition, the trial met all ranked secondary endpoints, including the Health Assessment Questionnaire–Disability Index change from baseline, 90% improvement in the Psoriasis Area and Severity Index (PASI90), Short-Form 36-Item Health Survey, and minimal disease activity (P < .001 for all comparisons).
Improvement with bimekizumab was rapid; curves began to separate from placebo by week 4, Dr. Merola said.
BE OPTIMAL efficacy
In this study, which had the same eligibility criteria as BE COMPLETE, patients were randomly assigned in a 2:3:1 ratio to receive 16 weeks of treatment with either placebo, bimekizumab 160 mg every 4 weeks, or adalimumab 40 mg every 2 weeks as a reference treatment.
This trial also met its primary and ranked secondary endpoints, which were similar to those of BE COMPLETE but also included measures of pooled resolution of enthesitis and dactylitis and change from baseline in van der Heijde modified total Sharp score (P < .001 for all comparisons).
In all, 43.9% of patients who received bimekizumab and 45.7% who received adalimumab achieved ACR50 at week 16, compared with 10% of patients who received placebo. The difference between the placebo and bimekizumab groups was significant (P < .001).
Safety
More patients who received the two active agents in this trial had treatment-emergent adverse events (TEAEs) in comparison with those in the placebo arm, but the incidence of serious TEAEs was less than 2% in each arm.
The most frequent events were nasopharyngitis, upper respiratory tract infection, headache, diarrhea, and hypertension.
Patients tolerated bimekizumab well, and there were no unexpected safety signals, Dr. McInnes said.
Clues to efficacy
In the question-and-answer session following Dr. McInnes’ presentation, Ronald Van Vollenhoven, MD, of the University of Amsterdam, said, “I have a question that is sort of generic in studies of psoriatic arthritis, so it does not only apply to this study, but the skin responses seem to be excellent – PASI90 sounds wonderful – but given that this is the case, is it reasonable to claim that the study is double-blinded in respect to the joints?”
Dr. McInnes replied that while he has considered this conundrum for many years in trials of drugs for psoriatic arthritis, “it doesn’t seem to be a major determinant of the outcome.”
The studies were supported by UCB Pharma. Dr. Merola and Dr. McInnes have consulted for UCB and other pharmaceutical companies that market drugs for psoriatic arthritis and psoriasis. Dr. Van Vollenhoven has received research support, has consulted for, and has spoken on behalf of UCB and other pharmaceutical companies.
A version of this article first appeared on Medscape.com.
COPENHAGEN – For patients with active psoriatic arthritis for whom tumor necrosis factor (TNF) inhibitors failed to produce an adequate response, use of the dual interleukin-17 (IL-17) inhibitor bimekizumab (Bimzelx) was associated with significant improvement in joint, skin, and health-related quality-of-life parameters, compared with placebo, reported investigators in the phase 3, double-blind, randomized BE COMPLETE trial.
The primary endpoint, which was the percentage of patients who had 50% improvement in American College of Rheumatology response criteria (ACR50) at 16 weeks, was achieved in 43.4% of patients assigned to receive bimekizumab 160 mg every 4 weeks, compared with 6.8% among patients who received placebo, reported Joseph F. Merola, MD, a dermatologist and rheumatologist at Brigham and Women’s Hospital in Boston.
“The high-level and exciting take-home [message is] that BE COMPLETE did meet all primary and all ranked secondary endpoints at week 16,” he said at the annual European Congress of Rheumatology.
Also at the congress, Iain McInnes, MD, PhD, of the Institute of Infection, Immunity, and Inflammation at the University of Glasgow, Scotland, presented data from a second phase 3, double-blind, randomized trial called BE OPTIMAL that showed similar benefits for patients with psoriatic arthritis who had not previously received biologic disease-modifying antirheumatic drugs.
“This is a new mode of action, inhibiting two cytokines simultaneously,” he said in a late-breaking oral abstract session.
As previously reported by this news organization, use of bimekizumab led to rapid reductions in signs and symptoms of radiographic axial spondyloarthritis in the phase 3 trial called BE MOBILE 2.
Bimekizumab is a monoclonal immunoglobulin G1 antibody that selectively inhibits IL-17A and IL-17F. It is approved in the European Union for treating adults with moderate to severe plaque psoriasis.
BE COMPLETE efficacy
Inclusion criteria comprised adult-onset psoriatic arthritis meeting Classification Criteria for Psoriatic Arthritis (CASPAR) for at least 6 months; tender and swollen joint counts of at least 3/68; one or more active psoriatic lesions; and/or a documented history of psoriasis characterized by intolerance to one or two TNF inhibitors or failure of TNF inhibitors. Patients were randomly assigned in a 2:1 ratio to receive either bimekizumab 160 mg every 4 weeks (n = 267) or placebo (n = 133) for 16 weeks.
Some participants are being followed in the extension BE VITAL study, which will evaluate response to treatment and long-term safety. Patients who do enroll in the extension study will be followed for safety for a period of 20 weeks after the last dose.
As noted before, the trial met its primary endpoint of a significant improvement over placebo in ACR50 (hazard ratio, 11.1; P < .001).
In addition, the trial met all ranked secondary endpoints, including the Health Assessment Questionnaire–Disability Index change from baseline, 90% improvement in the Psoriasis Area and Severity Index (PASI90), Short-Form 36-Item Health Survey, and minimal disease activity (P < .001 for all comparisons).
Improvement with bimekizumab was rapid; curves began to separate from placebo by week 4, Dr. Merola said.
BE OPTIMAL efficacy
In this study, which had the same eligibility criteria as BE COMPLETE, patients were randomly assigned in a 2:3:1 ratio to receive 16 weeks of treatment with either placebo, bimekizumab 160 mg every 4 weeks, or adalimumab 40 mg every 2 weeks as a reference treatment.
This trial also met its primary and ranked secondary endpoints, which were similar to those of BE COMPLETE but also included measures of pooled resolution of enthesitis and dactylitis and change from baseline in van der Heijde modified total Sharp score (P < .001 for all comparisons).
In all, 43.9% of patients who received bimekizumab and 45.7% who received adalimumab achieved ACR50 at week 16, compared with 10% of patients who received placebo. The difference between the placebo and bimekizumab groups was significant (P < .001).
Safety
More patients who received the two active agents in this trial had treatment-emergent adverse events (TEAEs) in comparison with those in the placebo arm, but the incidence of serious TEAEs was less than 2% in each arm.
The most frequent events were nasopharyngitis, upper respiratory tract infection, headache, diarrhea, and hypertension.
Patients tolerated bimekizumab well, and there were no unexpected safety signals, Dr. McInnes said.
Clues to efficacy
In the question-and-answer session following Dr. McInnes’ presentation, Ronald Van Vollenhoven, MD, of the University of Amsterdam, said, “I have a question that is sort of generic in studies of psoriatic arthritis, so it does not only apply to this study, but the skin responses seem to be excellent – PASI90 sounds wonderful – but given that this is the case, is it reasonable to claim that the study is double-blinded in respect to the joints?”
Dr. McInnes replied that while he has considered this conundrum for many years in trials of drugs for psoriatic arthritis, “it doesn’t seem to be a major determinant of the outcome.”
The studies were supported by UCB Pharma. Dr. Merola and Dr. McInnes have consulted for UCB and other pharmaceutical companies that market drugs for psoriatic arthritis and psoriasis. Dr. Van Vollenhoven has received research support, has consulted for, and has spoken on behalf of UCB and other pharmaceutical companies.
A version of this article first appeared on Medscape.com.
AT THE EULAR 2022 CONGRESS
FTC decision to investigate pharmacy benefit managers applauded by rheumatologists
The Federal Trade Commission’s announcement June 7 of a plan to investigate the business practices of pharmacy benefit managers (PBMs) was welcome news to rheumatologists. Widespread concern about the cost of prescription drugs and an additional 24,000 comments from the public prompted the agency’s decision to examine PBMs, which act as intermediaries between insurers, manufacturers, and pharmacies.
PBMs negotiate drug prices and rebates with manufacturers, reimburse pharmacies for drug costs, and create insurers’ drug formularies. But it’s widely held that instead of managing and leveling costs, PBMs have ratcheted up prices at multiple junctures to gain more profit.
The FTC’s investigation will focus on the six largest PBMs: CVS Caremark, Express Scripts, OptumRx, Humana, Prime Therapeutics, and MedImpact Healthcare Systems. CVS Caremark is owned by CVS, Express Scripts is owned by Cigna, and OptumRx is owned by UnitedHealth. The companies will have 90 days to respond to the commission’s official request for information.
Some of the information the FTC plans to ask about includes how the companies may be pushing patients toward using PBM-owned pharmacies and how rebates affect insurers’ formularies and the cost of drugs for patients.
The purchase or establishment of PBMs by the largest insurance companies – known as vertical integration – makes it nearly impossible for outsiders to determine what’s really causing price increases for prescription drugs. “The black box of secretive contracts and monies changing hands between manufacturers and PBMs has grown quite large since the Department of Justice and the FTC allowed the big three PBMs to be part of the three largest health insurance companies,” Madelaine A. Feldman, MD, a rheumatologist at the Rheumatology Group, New Orleans, and president of the Coalition of State Rheumatology Organizations, told this news organization.

Dr. Feldman and fellow rheumatologists at the American College of Rheumatology are happy that the FTC has decided to pursue this investigation. They note that rheumatologists have been calling for action for years and are eager to see change.
This probe aims to determine not only how the PBM industry affects pharmacists but also how their practices create ripple effects across the prescription drug industry, said Dr. Feldman. “I was very happy to see that they will be investigating how rebates and other manufacturer price concessions affect formulary construction and utilization management tools, ultimately increasing drug prices and patient cost share.”
A version of this article first appeared on Medscape.com.
The Federal Trade Commission’s announcement June 7 of a plan to investigate the business practices of pharmacy benefit managers (PBMs) was welcome news to rheumatologists. Widespread concern about the cost of prescription drugs and an additional 24,000 comments from the public prompted the agency’s decision to examine PBMs, which act as intermediaries between insurers, manufacturers, and pharmacies.
PBMs negotiate drug prices and rebates with manufacturers, reimburse pharmacies for drug costs, and create insurers’ drug formularies. But it’s widely held that instead of managing and leveling costs, PBMs have ratcheted up prices at multiple junctures to gain more profit.
The FTC’s investigation will focus on the six largest PBMs: CVS Caremark, Express Scripts, OptumRx, Humana, Prime Therapeutics, and MedImpact Healthcare Systems. CVS Caremark is owned by CVS, Express Scripts is owned by Cigna, and OptumRx is owned by UnitedHealth. The companies will have 90 days to respond to the commission’s official request for information.
Some of the information the FTC plans to ask about includes how the companies may be pushing patients toward using PBM-owned pharmacies and how rebates affect insurers’ formularies and the cost of drugs for patients.
The purchase or establishment of PBMs by the largest insurance companies – known as vertical integration – makes it nearly impossible for outsiders to determine what’s really causing price increases for prescription drugs. “The black box of secretive contracts and monies changing hands between manufacturers and PBMs has grown quite large since the Department of Justice and the FTC allowed the big three PBMs to be part of the three largest health insurance companies,” Madelaine A. Feldman, MD, a rheumatologist at the Rheumatology Group, New Orleans, and president of the Coalition of State Rheumatology Organizations, told this news organization.
Dr. Feldman and fellow rheumatologists at the American College of Rheumatology are happy that the FTC has decided to pursue this investigation. They note that rheumatologists have been calling for action for years and are eager to see change.
This probe aims to determine not only how the PBM industry affects pharmacists but also how their practices create ripple effects across the prescription drug industry, said Dr. Feldman. “I was very happy to see that they will be investigating how rebates and other manufacturer price concessions affect formulary construction and utilization management tools, ultimately increasing drug prices and patient cost share.”
A version of this article first appeared on Medscape.com.
The Federal Trade Commission’s announcement June 7 of a plan to investigate the business practices of pharmacy benefit managers (PBMs) was welcome news to rheumatologists. Widespread concern about the cost of prescription drugs and an additional 24,000 comments from the public prompted the agency’s decision to examine PBMs, which act as intermediaries between insurers, manufacturers, and pharmacies.
PBMs negotiate drug prices and rebates with manufacturers, reimburse pharmacies for drug costs, and create insurers’ drug formularies. But it’s widely held that instead of managing and leveling costs, PBMs have ratcheted up prices at multiple junctures to gain more profit.
The FTC’s investigation will focus on the six largest PBMs: CVS Caremark, Express Scripts, OptumRx, Humana, Prime Therapeutics, and MedImpact Healthcare Systems. CVS Caremark is owned by CVS, Express Scripts is owned by Cigna, and OptumRx is owned by UnitedHealth. The companies will have 90 days to respond to the commission’s official request for information.
Some of the information the FTC plans to ask about includes how the companies may be pushing patients toward using PBM-owned pharmacies and how rebates affect insurers’ formularies and the cost of drugs for patients.
The purchase or establishment of PBMs by the largest insurance companies – known as vertical integration – makes it nearly impossible for outsiders to determine what’s really causing price increases for prescription drugs. “The black box of secretive contracts and monies changing hands between manufacturers and PBMs has grown quite large since the Department of Justice and the FTC allowed the big three PBMs to be part of the three largest health insurance companies,” Madelaine A. Feldman, MD, a rheumatologist at the Rheumatology Group, New Orleans, and president of the Coalition of State Rheumatology Organizations, told this news organization.
Dr. Feldman and fellow rheumatologists at the American College of Rheumatology are happy that the FTC has decided to pursue this investigation. They note that rheumatologists have been calling for action for years and are eager to see change.
This probe aims to determine not only how the PBM industry affects pharmacists but also how their practices create ripple effects across the prescription drug industry, said Dr. Feldman. “I was very happy to see that they will be investigating how rebates and other manufacturer price concessions affect formulary construction and utilization management tools, ultimately increasing drug prices and patient cost share.”
A version of this article first appeared on Medscape.com.
New onset-depression after RA diagnosis raises mortality risk ‘more than sixfold’
The development of depression after a rheumatoid arthritis diagnosis increased the risk for death “more than sixfold” when compared with having no depression at diagnosis, according to Danish researchers.
Cumulative mortality at 10 years was approximately 37% in patients with comorbid RA and depression versus around 13.5% of RA patients with no depression, Jens Kristian Pedersen, MD, PhD, of Odense (Denmark) University Hospital–Svendborg Hospital and the department of clinical research at the University of Southern Denmark, also in Odense, reported at the annual European Congress of Rheumatology.

“According to [antidepressant] exposure status, the cumulative mortality followed two clearly different paths,” Dr. Pedersen said. “The mortality curves separated early and already within the first and second year of follow-up.”
RA, depression, and mortality
Rates of depression in patients with RA are high, Dr. Pedersen said, and while it’s previously been reported that their coexistence can increase mortality, this is the first time that the link has been investigated in a population newly diagnosed with RA.
In this study, Dr. Pedersen and collaborators wanted to look at the association in incident RA and defined depression as the first filling of an antidepressant prescription.
“Although antidepressants are used for different indications, we have recently described that in RA the most frequent indication for filling antidepressants is depression,” he explained. Moreover, that research found that “the frequency of filling coincides with the occurrence of depressive disorder previously reported in the scientific literature.”
Data sourced from multiple Danish registers
To examine the mortality risk associated with newly diagnosed RA and new-onset depression, Dr. Pedersen described how five different Danish registers were used.
First, data from the DANBIO register were used to identify patients with incident RA living in Denmark over a 10-year period ending in December 2018. Although perhaps widely known as a biologics register, DANBIO is required by the Danish National Board of Health to collect information on all patients with RA, regardless of their treatment.
Next, the Danish National Prescription Register and Danish National Patient Register were consulted to obtain data on patients who had a first prescription for antidepressant treatment and information on those who developed a diagnosis of depression. Demographic, vital status, and socioeconomic data were collated from the Danish Civil Registration System and Statistics Denmark databases.
To be sure they were looking at incident cases of RA and new cases of depression, the researchers excluded anyone with an existing prescription of antidepressants or methotrexate, or who had a confirmed diagnosis of either disorder 3 years prior to the index date of Jan. 1, 2008.
This meant that, from a total population of 18,000 patients in the DANBIO database, there were just over 11,000 who could be included in the analyses.
Overall, the median age at RA diagnosis was 61 years, two-thirds were female, and two-thirds had seropositive disease.
New-onset depression in incident RA
“During follow-up, about 10% filled a prescription of antidepressants,” said Dr. Pedersen, adding that there were 671 deaths, representing around 57,000 person-years at risk.
“The majority died from natural causes,” he said, although the cause of death was unknown in 30% of cases.
Comparing those who did and did not have a prescription for antidepressants, there were some differences in the age at which death occurred, the percentage of females to males, the presence of other comorbidities, and levels of higher education and income. These were all adjusted for in the analyses.
Adjusted hazard rate ratios were calculated to look at the mortality risk in patients who had antidepressant exposure. The highest HRR for mortality with antidepressant use was seen in patients aged 55 years or younger at 6.66, with the next highest HRRs being for male gender (3.70) and seropositive RA (3.45).
But HRRs for seronegative RA, female gender, and age 55-70 years or older than 75 years were all still around 3.0.
Depression definition questioned
“My only concern is about the definition of depression in your analysis,” said a member of the audience at the congress.
“You used antidepressant use as a proxy of depression diagnosis, but it might be that most or many patients have taken [medication] like duloxetine for pain control, and you are just seeing higher disease activity and more aggressive RA.”
Dr. Pedersen responded: “After the EULAR 2022 submission deadline, we reanalyzed our data using two other measures of depression.
“First, we use treatment with antidepressants with a positive indication of depression, according to the prescribing physician, and secondly, we used first diagnosis with depression according to ICD-10 Code F32 – ‘depressive episode after discharge from hospital as an outpatient,’ ” he said.
“All definitions end up with a hazard rate ratio of about three. So, in my opinion, it doesn’t matter whether you focus on one measure of depression or the other.”
David Isenberg, MD, FRCP, professor of rheumatology at University College London, wanted to know more about the antecedent history of depression and whether people who had been depressed maybe a decade or 2 decades before, were more likely to get RA.
That calculation has not been done, Dr. Pedersen said, adding that the study also can’t account for people who may have had recurrent depression. Depression treatment guidelines often recommend nonpharmacologic intervention in the first instance, “so we do not necessarily get the right picture of recurrent depression if we look further back.”
Pointing out that the sixfold increase in mortality was impressive, another delegate asked about whether it was because of a higher disease activity or joint damage and if the mortality risk might be lower in patients who are in remission.
“We don’t know that yet,” Dr. Pedersen answered. “We haven’t done the calculations, but there is the issue of residual confounding if we don’t take all relevant covariates into account. So, we need to do that calculation as well.”
The study was supported by the Danish Rheumatism Association. Dr. Pedersen had no conflicts of interest to disclose.
The development of depression after a rheumatoid arthritis diagnosis increased the risk for death “more than sixfold” when compared with having no depression at diagnosis, according to Danish researchers.
Cumulative mortality at 10 years was approximately 37% in patients with comorbid RA and depression versus around 13.5% of RA patients with no depression, Jens Kristian Pedersen, MD, PhD, of Odense (Denmark) University Hospital–Svendborg Hospital and the department of clinical research at the University of Southern Denmark, also in Odense, reported at the annual European Congress of Rheumatology.
“According to [antidepressant] exposure status, the cumulative mortality followed two clearly different paths,” Dr. Pedersen said. “The mortality curves separated early and already within the first and second year of follow-up.”
RA, depression, and mortality
Rates of depression in patients with RA are high, Dr. Pedersen said, and while it’s previously been reported that their coexistence can increase mortality, this is the first time that the link has been investigated in a population newly diagnosed with RA.
In this study, Dr. Pedersen and collaborators wanted to look at the association in incident RA and defined depression as the first filling of an antidepressant prescription.
“Although antidepressants are used for different indications, we have recently described that in RA the most frequent indication for filling antidepressants is depression,” he explained. Moreover, that research found that “the frequency of filling coincides with the occurrence of depressive disorder previously reported in the scientific literature.”
Data sourced from multiple Danish registers
To examine the mortality risk associated with newly diagnosed RA and new-onset depression, Dr. Pedersen described how five different Danish registers were used.
First, data from the DANBIO register were used to identify patients with incident RA living in Denmark over a 10-year period ending in December 2018. Although perhaps widely known as a biologics register, DANBIO is required by the Danish National Board of Health to collect information on all patients with RA, regardless of their treatment.
Next, the Danish National Prescription Register and Danish National Patient Register were consulted to obtain data on patients who had a first prescription for antidepressant treatment and information on those who developed a diagnosis of depression. Demographic, vital status, and socioeconomic data were collated from the Danish Civil Registration System and Statistics Denmark databases.
To be sure they were looking at incident cases of RA and new cases of depression, the researchers excluded anyone with an existing prescription of antidepressants or methotrexate, or who had a confirmed diagnosis of either disorder 3 years prior to the index date of Jan. 1, 2008.
This meant that, from a total population of 18,000 patients in the DANBIO database, there were just over 11,000 who could be included in the analyses.
Overall, the median age at RA diagnosis was 61 years, two-thirds were female, and two-thirds had seropositive disease.
New-onset depression in incident RA
“During follow-up, about 10% filled a prescription of antidepressants,” said Dr. Pedersen, adding that there were 671 deaths, representing around 57,000 person-years at risk.
“The majority died from natural causes,” he said, although the cause of death was unknown in 30% of cases.
Comparing those who did and did not have a prescription for antidepressants, there were some differences in the age at which death occurred, the percentage of females to males, the presence of other comorbidities, and levels of higher education and income. These were all adjusted for in the analyses.
Adjusted hazard rate ratios were calculated to look at the mortality risk in patients who had antidepressant exposure. The highest HRR for mortality with antidepressant use was seen in patients aged 55 years or younger at 6.66, with the next highest HRRs being for male gender (3.70) and seropositive RA (3.45).
But HRRs for seronegative RA, female gender, and age 55-70 years or older than 75 years were all still around 3.0.
Depression definition questioned
“My only concern is about the definition of depression in your analysis,” said a member of the audience at the congress.
“You used antidepressant use as a proxy of depression diagnosis, but it might be that most or many patients have taken [medication] like duloxetine for pain control, and you are just seeing higher disease activity and more aggressive RA.”
Dr. Pedersen responded: “After the EULAR 2022 submission deadline, we reanalyzed our data using two other measures of depression.
“First, we use treatment with antidepressants with a positive indication of depression, according to the prescribing physician, and secondly, we used first diagnosis with depression according to ICD-10 Code F32 – ‘depressive episode after discharge from hospital as an outpatient,’ ” he said.
“All definitions end up with a hazard rate ratio of about three. So, in my opinion, it doesn’t matter whether you focus on one measure of depression or the other.”
David Isenberg, MD, FRCP, professor of rheumatology at University College London, wanted to know more about the antecedent history of depression and whether people who had been depressed maybe a decade or 2 decades before, were more likely to get RA.
That calculation has not been done, Dr. Pedersen said, adding that the study also can’t account for people who may have had recurrent depression. Depression treatment guidelines often recommend nonpharmacologic intervention in the first instance, “so we do not necessarily get the right picture of recurrent depression if we look further back.”
Pointing out that the sixfold increase in mortality was impressive, another delegate asked about whether it was because of a higher disease activity or joint damage and if the mortality risk might be lower in patients who are in remission.
“We don’t know that yet,” Dr. Pedersen answered. “We haven’t done the calculations, but there is the issue of residual confounding if we don’t take all relevant covariates into account. So, we need to do that calculation as well.”
The study was supported by the Danish Rheumatism Association. Dr. Pedersen had no conflicts of interest to disclose.
The development of depression after a rheumatoid arthritis diagnosis increased the risk for death “more than sixfold” when compared with having no depression at diagnosis, according to Danish researchers.
Cumulative mortality at 10 years was approximately 37% in patients with comorbid RA and depression versus around 13.5% of RA patients with no depression, Jens Kristian Pedersen, MD, PhD, of Odense (Denmark) University Hospital–Svendborg Hospital and the department of clinical research at the University of Southern Denmark, also in Odense, reported at the annual European Congress of Rheumatology.
“According to [antidepressant] exposure status, the cumulative mortality followed two clearly different paths,” Dr. Pedersen said. “The mortality curves separated early and already within the first and second year of follow-up.”
RA, depression, and mortality
Rates of depression in patients with RA are high, Dr. Pedersen said, and while it’s previously been reported that their coexistence can increase mortality, this is the first time that the link has been investigated in a population newly diagnosed with RA.
In this study, Dr. Pedersen and collaborators wanted to look at the association in incident RA and defined depression as the first filling of an antidepressant prescription.
“Although antidepressants are used for different indications, we have recently described that in RA the most frequent indication for filling antidepressants is depression,” he explained. Moreover, that research found that “the frequency of filling coincides with the occurrence of depressive disorder previously reported in the scientific literature.”
Data sourced from multiple Danish registers
To examine the mortality risk associated with newly diagnosed RA and new-onset depression, Dr. Pedersen described how five different Danish registers were used.
First, data from the DANBIO register were used to identify patients with incident RA living in Denmark over a 10-year period ending in December 2018. Although perhaps widely known as a biologics register, DANBIO is required by the Danish National Board of Health to collect information on all patients with RA, regardless of their treatment.
Next, the Danish National Prescription Register and Danish National Patient Register were consulted to obtain data on patients who had a first prescription for antidepressant treatment and information on those who developed a diagnosis of depression. Demographic, vital status, and socioeconomic data were collated from the Danish Civil Registration System and Statistics Denmark databases.
To be sure they were looking at incident cases of RA and new cases of depression, the researchers excluded anyone with an existing prescription of antidepressants or methotrexate, or who had a confirmed diagnosis of either disorder 3 years prior to the index date of Jan. 1, 2008.
This meant that, from a total population of 18,000 patients in the DANBIO database, there were just over 11,000 who could be included in the analyses.
Overall, the median age at RA diagnosis was 61 years, two-thirds were female, and two-thirds had seropositive disease.
New-onset depression in incident RA
“During follow-up, about 10% filled a prescription of antidepressants,” said Dr. Pedersen, adding that there were 671 deaths, representing around 57,000 person-years at risk.
“The majority died from natural causes,” he said, although the cause of death was unknown in 30% of cases.
Comparing those who did and did not have a prescription for antidepressants, there were some differences in the age at which death occurred, the percentage of females to males, the presence of other comorbidities, and levels of higher education and income. These were all adjusted for in the analyses.
Adjusted hazard rate ratios were calculated to look at the mortality risk in patients who had antidepressant exposure. The highest HRR for mortality with antidepressant use was seen in patients aged 55 years or younger at 6.66, with the next highest HRRs being for male gender (3.70) and seropositive RA (3.45).
But HRRs for seronegative RA, female gender, and age 55-70 years or older than 75 years were all still around 3.0.
Depression definition questioned
“My only concern is about the definition of depression in your analysis,” said a member of the audience at the congress.
“You used antidepressant use as a proxy of depression diagnosis, but it might be that most or many patients have taken [medication] like duloxetine for pain control, and you are just seeing higher disease activity and more aggressive RA.”
Dr. Pedersen responded: “After the EULAR 2022 submission deadline, we reanalyzed our data using two other measures of depression.
“First, we use treatment with antidepressants with a positive indication of depression, according to the prescribing physician, and secondly, we used first diagnosis with depression according to ICD-10 Code F32 – ‘depressive episode after discharge from hospital as an outpatient,’ ” he said.
“All definitions end up with a hazard rate ratio of about three. So, in my opinion, it doesn’t matter whether you focus on one measure of depression or the other.”
David Isenberg, MD, FRCP, professor of rheumatology at University College London, wanted to know more about the antecedent history of depression and whether people who had been depressed maybe a decade or 2 decades before, were more likely to get RA.
That calculation has not been done, Dr. Pedersen said, adding that the study also can’t account for people who may have had recurrent depression. Depression treatment guidelines often recommend nonpharmacologic intervention in the first instance, “so we do not necessarily get the right picture of recurrent depression if we look further back.”
Pointing out that the sixfold increase in mortality was impressive, another delegate asked about whether it was because of a higher disease activity or joint damage and if the mortality risk might be lower in patients who are in remission.
“We don’t know that yet,” Dr. Pedersen answered. “We haven’t done the calculations, but there is the issue of residual confounding if we don’t take all relevant covariates into account. So, we need to do that calculation as well.”
The study was supported by the Danish Rheumatism Association. Dr. Pedersen had no conflicts of interest to disclose.
FROM THE EULAR 2022 CONGRESS
Diagnostic axSpA MRI features differ in men and women
MRI criteria used to diagnose axial spondyloarthritis (axSpA) may require gender-specific revision, according to research conducted at Charité Universitätsmedizin Berlin.
Although established MRI markers were detected in both sexes, their prevalence was substantially different in some cases – ankylosis and fat metaplasia were more prevalent in male than female patients, for example, while sclerosis was far more common in females.

“There’s increasing evidence in the literature and awareness in clinical practice that there are some sex differences in the clinical presentation of axSpA,” said radiologist Sevtap Tugce Ulas, MD, at the annual European Congress of Rheumatology.
She presented the first results of a study examining the diagnostic performance of MRI findings for men and women. “Men have a high risk of structural damage, while women are more likely to be affected by peripheral manifestations with a higher risk for pain, stiffness, and fatigue.”
Joint biomechanics are different in men and women, she pointed out, which might explain some of the disparities. She observed that diagnostic delay – a known problem in axSpA – was “significantly longer” in female patients.
Dr. Ulas and colleagues conducted a post hoc analysis of participants in six prospective axSpA cohorts. From a total of more than 1,100 participants, the researchers identified 684 who had both a clinical diagnosis and complete imaging data available for evaluation. The study population included 379 men and women with and 305 men and women without axSpA.
The mean age overall in all groups was 37 years, with axSpA patients more likely than controls to have elevated C-reactive protein levels; levels were also higher in men with axSpA, compared with in women with axSpA.
Men with axSpA also were more likely than women to be HLA-B27 positive (91% vs. 79%), but there were similar mean Bath Ankylosing Spondylitis Disease Activity Index scores recorded (4.4 vs. 4.6) among the subjects with axSpA.
Two experienced radiologists, blinded to the clinical diagnosis, scored the MRI images independently of each other, looking for the presence of ankylosis; erosions; sclerosis; fat metaplasia; and bone marrow edema in the ventral, mid, and dorsal regions of the sacroiliac joints. Any disagreement between the two reviewers was assessed by a third, more experienced radiologist.
Clear differences in MRI markers
“If you look in detail, we found no major sex-specific differences for erosion and bone marrow edema,” Dr. Ulas reported.
The situation was quite different for other MRI parameters examined. Indeed, more men than women had evidence of ankylosis (24.3% vs. 7.4%) and fat metaplasia (58.8% vs. 42.6%). Conversely, women were more likely than men to have evidence of sclerosis (75.0% vs. 57.6%).
“To make the performance more easily comparable, we calculated a diagnostic odds ratio, which is simply positive likelihood ratio divided by negative likelihood ratio,” Dr. Ulas said.
Doing this showed that the presence of ankylosis had “an almost 10 times stronger performance in men,” with a DOR of 40.1 versus 4.7 for women.
“Interestingly, this was not only caused by low prevalence in females, but also by high rates of false positives,” she said.
DOR for the other parameters in men and women were 18.6 and 6.3 for fat metaplasia, 2.5 and 3.0 for sclerosis, 17.6 and 11.1 for joint erosion, and 2.5 and 3.7 for bone edema.
Overall, diagnostic accuracy was improved only when middle and dorsal lesions were considered.
‘Remarkably different’ results
“By definition, these patients have the same disease,” said Hendrik Schulze-Koops, MD, of Ludwig Maximilian University of Munich (Germany).

Yet these are “remarkably different” findings, Dr. Schulze-Koops said during a closing highlights session of the congress.
Current imaging practices don’t differentiate between the sexes but perhaps they might need to, he said, because these data suggest “female patients have a different MRI pattern from what we learn from the textbooks.
“[The investigators] say diagnostic performance of established imaging markers on MRI is significantly lower in female axSpA patients, and we should consider this when we are in the situation where we question the disease.”
Marta Mosca, MD, PhD, of the University of Pisa (Italy) and who cochaired the session in which Dr. Ulas had presented the findings commented: “I think is very interesting. We always talk about gender differences in treatment and in the assessment.”

However, Dr. Mosca asked if there were plans to study other patient cohorts, notably those not just referred by a rheumatologist, as that was “a big limitation.”
Dr. Ulas replied: “I think we need follow-up studies to investigate this problem, because we know that there are differences in the clinical presentation and also in the imaging, and this is an important point.”
Of course, there are other limitations, Dr. Ulas said, such as the sole use of conventional T1-weighted spin echo sequences. Although often routinely used in clinical practice, this imaging technique can lead to overestimation of structural damage. Moreover, “subtle differences might have been missed” in bone marrow edema because it wasn’t included in the semiquantitative scoring system used.
“Most importantly, the MRI images under investigation were also used in the diagnostic process, which carries the risk of circular reasoning,” Dr. Ulas said.
However, there are clearly some differences in imaging appearance between men and women, and “we show a significantly lower performance of many typical MRI findings in women,” Dr. Ulas said. “We hope that these findings might spark a critical discussion on the appropriateness of sex-blind classification criteria for axSpA, and hopefully, eventually lead to refined criteria for both sexes.”
Dr. Ulas had no conflicts of interest to disclose. Dr. Schulze-Koops and Dr. Mosca were not involved in the study and had no relevant disclosures.
MRI criteria used to diagnose axial spondyloarthritis (axSpA) may require gender-specific revision, according to research conducted at Charité Universitätsmedizin Berlin.
Although established MRI markers were detected in both sexes, their prevalence was substantially different in some cases – ankylosis and fat metaplasia were more prevalent in male than female patients, for example, while sclerosis was far more common in females.
“There’s increasing evidence in the literature and awareness in clinical practice that there are some sex differences in the clinical presentation of axSpA,” said radiologist Sevtap Tugce Ulas, MD, at the annual European Congress of Rheumatology.
She presented the first results of a study examining the diagnostic performance of MRI findings for men and women. “Men have a high risk of structural damage, while women are more likely to be affected by peripheral manifestations with a higher risk for pain, stiffness, and fatigue.”
Joint biomechanics are different in men and women, she pointed out, which might explain some of the disparities. She observed that diagnostic delay – a known problem in axSpA – was “significantly longer” in female patients.
Dr. Ulas and colleagues conducted a post hoc analysis of participants in six prospective axSpA cohorts. From a total of more than 1,100 participants, the researchers identified 684 who had both a clinical diagnosis and complete imaging data available for evaluation. The study population included 379 men and women with and 305 men and women without axSpA.
The mean age overall in all groups was 37 years, with axSpA patients more likely than controls to have elevated C-reactive protein levels; levels were also higher in men with axSpA, compared with in women with axSpA.
Men with axSpA also were more likely than women to be HLA-B27 positive (91% vs. 79%), but there were similar mean Bath Ankylosing Spondylitis Disease Activity Index scores recorded (4.4 vs. 4.6) among the subjects with axSpA.
Two experienced radiologists, blinded to the clinical diagnosis, scored the MRI images independently of each other, looking for the presence of ankylosis; erosions; sclerosis; fat metaplasia; and bone marrow edema in the ventral, mid, and dorsal regions of the sacroiliac joints. Any disagreement between the two reviewers was assessed by a third, more experienced radiologist.
Clear differences in MRI markers
“If you look in detail, we found no major sex-specific differences for erosion and bone marrow edema,” Dr. Ulas reported.
The situation was quite different for other MRI parameters examined. Indeed, more men than women had evidence of ankylosis (24.3% vs. 7.4%) and fat metaplasia (58.8% vs. 42.6%). Conversely, women were more likely than men to have evidence of sclerosis (75.0% vs. 57.6%).
“To make the performance more easily comparable, we calculated a diagnostic odds ratio, which is simply positive likelihood ratio divided by negative likelihood ratio,” Dr. Ulas said.
Doing this showed that the presence of ankylosis had “an almost 10 times stronger performance in men,” with a DOR of 40.1 versus 4.7 for women.
“Interestingly, this was not only caused by low prevalence in females, but also by high rates of false positives,” she said.
DOR for the other parameters in men and women were 18.6 and 6.3 for fat metaplasia, 2.5 and 3.0 for sclerosis, 17.6 and 11.1 for joint erosion, and 2.5 and 3.7 for bone edema.
Overall, diagnostic accuracy was improved only when middle and dorsal lesions were considered.
‘Remarkably different’ results
“By definition, these patients have the same disease,” said Hendrik Schulze-Koops, MD, of Ludwig Maximilian University of Munich (Germany).
Yet these are “remarkably different” findings, Dr. Schulze-Koops said during a closing highlights session of the congress.
Current imaging practices don’t differentiate between the sexes but perhaps they might need to, he said, because these data suggest “female patients have a different MRI pattern from what we learn from the textbooks.
“[The investigators] say diagnostic performance of established imaging markers on MRI is significantly lower in female axSpA patients, and we should consider this when we are in the situation where we question the disease.”
Marta Mosca, MD, PhD, of the University of Pisa (Italy) and who cochaired the session in which Dr. Ulas had presented the findings commented: “I think is very interesting. We always talk about gender differences in treatment and in the assessment.”
However, Dr. Mosca asked if there were plans to study other patient cohorts, notably those not just referred by a rheumatologist, as that was “a big limitation.”
Dr. Ulas replied: “I think we need follow-up studies to investigate this problem, because we know that there are differences in the clinical presentation and also in the imaging, and this is an important point.”
Of course, there are other limitations, Dr. Ulas said, such as the sole use of conventional T1-weighted spin echo sequences. Although often routinely used in clinical practice, this imaging technique can lead to overestimation of structural damage. Moreover, “subtle differences might have been missed” in bone marrow edema because it wasn’t included in the semiquantitative scoring system used.
“Most importantly, the MRI images under investigation were also used in the diagnostic process, which carries the risk of circular reasoning,” Dr. Ulas said.
However, there are clearly some differences in imaging appearance between men and women, and “we show a significantly lower performance of many typical MRI findings in women,” Dr. Ulas said. “We hope that these findings might spark a critical discussion on the appropriateness of sex-blind classification criteria for axSpA, and hopefully, eventually lead to refined criteria for both sexes.”
Dr. Ulas had no conflicts of interest to disclose. Dr. Schulze-Koops and Dr. Mosca were not involved in the study and had no relevant disclosures.
MRI criteria used to diagnose axial spondyloarthritis (axSpA) may require gender-specific revision, according to research conducted at Charité Universitätsmedizin Berlin.
Although established MRI markers were detected in both sexes, their prevalence was substantially different in some cases – ankylosis and fat metaplasia were more prevalent in male than female patients, for example, while sclerosis was far more common in females.
“There’s increasing evidence in the literature and awareness in clinical practice that there are some sex differences in the clinical presentation of axSpA,” said radiologist Sevtap Tugce Ulas, MD, at the annual European Congress of Rheumatology.
She presented the first results of a study examining the diagnostic performance of MRI findings for men and women. “Men have a high risk of structural damage, while women are more likely to be affected by peripheral manifestations with a higher risk for pain, stiffness, and fatigue.”
Joint biomechanics are different in men and women, she pointed out, which might explain some of the disparities. She observed that diagnostic delay – a known problem in axSpA – was “significantly longer” in female patients.
Dr. Ulas and colleagues conducted a post hoc analysis of participants in six prospective axSpA cohorts. From a total of more than 1,100 participants, the researchers identified 684 who had both a clinical diagnosis and complete imaging data available for evaluation. The study population included 379 men and women with and 305 men and women without axSpA.
The mean age overall in all groups was 37 years, with axSpA patients more likely than controls to have elevated C-reactive protein levels; levels were also higher in men with axSpA, compared with in women with axSpA.
Men with axSpA also were more likely than women to be HLA-B27 positive (91% vs. 79%), but there were similar mean Bath Ankylosing Spondylitis Disease Activity Index scores recorded (4.4 vs. 4.6) among the subjects with axSpA.
Two experienced radiologists, blinded to the clinical diagnosis, scored the MRI images independently of each other, looking for the presence of ankylosis; erosions; sclerosis; fat metaplasia; and bone marrow edema in the ventral, mid, and dorsal regions of the sacroiliac joints. Any disagreement between the two reviewers was assessed by a third, more experienced radiologist.
Clear differences in MRI markers
“If you look in detail, we found no major sex-specific differences for erosion and bone marrow edema,” Dr. Ulas reported.
The situation was quite different for other MRI parameters examined. Indeed, more men than women had evidence of ankylosis (24.3% vs. 7.4%) and fat metaplasia (58.8% vs. 42.6%). Conversely, women were more likely than men to have evidence of sclerosis (75.0% vs. 57.6%).
“To make the performance more easily comparable, we calculated a diagnostic odds ratio, which is simply positive likelihood ratio divided by negative likelihood ratio,” Dr. Ulas said.
Doing this showed that the presence of ankylosis had “an almost 10 times stronger performance in men,” with a DOR of 40.1 versus 4.7 for women.
“Interestingly, this was not only caused by low prevalence in females, but also by high rates of false positives,” she said.
DOR for the other parameters in men and women were 18.6 and 6.3 for fat metaplasia, 2.5 and 3.0 for sclerosis, 17.6 and 11.1 for joint erosion, and 2.5 and 3.7 for bone edema.
Overall, diagnostic accuracy was improved only when middle and dorsal lesions were considered.
‘Remarkably different’ results
“By definition, these patients have the same disease,” said Hendrik Schulze-Koops, MD, of Ludwig Maximilian University of Munich (Germany).
Yet these are “remarkably different” findings, Dr. Schulze-Koops said during a closing highlights session of the congress.
Current imaging practices don’t differentiate between the sexes but perhaps they might need to, he said, because these data suggest “female patients have a different MRI pattern from what we learn from the textbooks.
“[The investigators] say diagnostic performance of established imaging markers on MRI is significantly lower in female axSpA patients, and we should consider this when we are in the situation where we question the disease.”
Marta Mosca, MD, PhD, of the University of Pisa (Italy) and who cochaired the session in which Dr. Ulas had presented the findings commented: “I think is very interesting. We always talk about gender differences in treatment and in the assessment.”
However, Dr. Mosca asked if there were plans to study other patient cohorts, notably those not just referred by a rheumatologist, as that was “a big limitation.”
Dr. Ulas replied: “I think we need follow-up studies to investigate this problem, because we know that there are differences in the clinical presentation and also in the imaging, and this is an important point.”
Of course, there are other limitations, Dr. Ulas said, such as the sole use of conventional T1-weighted spin echo sequences. Although often routinely used in clinical practice, this imaging technique can lead to overestimation of structural damage. Moreover, “subtle differences might have been missed” in bone marrow edema because it wasn’t included in the semiquantitative scoring system used.
“Most importantly, the MRI images under investigation were also used in the diagnostic process, which carries the risk of circular reasoning,” Dr. Ulas said.
However, there are clearly some differences in imaging appearance between men and women, and “we show a significantly lower performance of many typical MRI findings in women,” Dr. Ulas said. “We hope that these findings might spark a critical discussion on the appropriateness of sex-blind classification criteria for axSpA, and hopefully, eventually lead to refined criteria for both sexes.”
Dr. Ulas had no conflicts of interest to disclose. Dr. Schulze-Koops and Dr. Mosca were not involved in the study and had no relevant disclosures.
FROM THE EULAR 2022 CONGRESS
Autoimmune disease linked to better late-stage breast cancer survival
CHICAGO – Comorbid autoimmune disease is associated with a greater chance of survival among women with stage IV breast cancer, according to a retrospective study presented at the annual meeting of the American Society of Clinical Oncology.
“It’s counterintuitive that, if you have two diseases instead of one, that you live longer, so then we had to scratch our heads a little bit and think about why these people are living longer,” said lead author Demitrios Dedousis, MD, University Hospitals, Case Medical Center, Cleveland.
Dr. Dedousis and colleagues conducted a retrospective analysis of patients from Surveillance, Epidemiology, and End Results–Medicare databases between 2007 and 2014 with breast cancer. The study included data from 137,324 patients diagnosed between 2007 and 2012, before the widespread use of immunotherapy. 27% of patients had an autoimmune disease, most commonly rheumatoid arthritis (23%), psoriasis (2.4%), and systemic lupus erythematosus (1.1%).
When all patients were included in the analysis, those with autoimmune disorders had slightly longer survival times, but these weren’t clinically significant. A subanalysis found a greater difference in survival.
The association appears more pronounced in metastatic cancer. Patients with stage 4 breast cancer and autoimmune disease had a longer mean overall survival (36 months vs. 30 months; hazard ratio, 1.46; P < .0001. Cancer-specific survival: HR, 1.39; P < .0001). Patients with autoimmune disease and stage 1-3 breast cancer had lower overall survival (P < .0001, P < 0.0001, and P = 0.026 respectively), compared with patients without autoimmune disease.
“What we thought was happening is that the lack of increased survival in stages 1 through 3 was hiding the increase in survival among the stage IV patients when looking at the overall cohort,” Dr. Dedousis said.
The retrospective nature of the study makes it impossible to draw any firm conclusions about causation. It could be that patients who have already been diagnosed with an autoimmune disease are more vigilant about going to health checkups. “There are other possible explanations, but the one that’s most interesting to us is that their immune system is involved in fighting the cancer. Our study certainly didn’t prove that, but it’s suggesting that’s a possibility,” Dr. Dedousis said.
He and his coauthors anticipate conducting similar studies in other cancers to see if there are similar relationships. Some preliminary work has already suggested something similar in lung cancer. “I think demonstrating this in a few kinds of cancer goes part of the way towards showing that this is a real biological phenomenon,” he said.
Another research avenue is to examine the immune systems and pathology specimens in patients with both an autoimmune disease and cancer to see if there is a greater immune response within the tumor. If so, that could suggest new immunotherapy strategies.
Another possibility is to look at the specific immune pathways within “protective” autoimmune conditions. “For the sake of argument, if we find a particular autoimmune condition is improving survival across multiple kinds of cancers, we could look at those pathways that are specifically involved in that autoimmune condition. It might help us identify a target for drug development,” Dr. Dedousis said.
Asked why a potential benefit might be more apparent in late-stage disease, he suggested that, in early-stage breast cancer, surgery and other treatments may be so effective that the immune system’s role only rarely makes a difference. It could play a larger role in late-stage disease when there are less effective therapies. It could also be that the immune system doesn’t recognize the cancer until it has spread beyond the regional lymph nodes on its way to metastasizing.
According to the National Cancer Institute, 10%-30% of people with cancer also have an autoimmune disease.
Dr. Dedousis has no relevant financial disclosures.
CHICAGO – Comorbid autoimmune disease is associated with a greater chance of survival among women with stage IV breast cancer, according to a retrospective study presented at the annual meeting of the American Society of Clinical Oncology.
“It’s counterintuitive that, if you have two diseases instead of one, that you live longer, so then we had to scratch our heads a little bit and think about why these people are living longer,” said lead author Demitrios Dedousis, MD, University Hospitals, Case Medical Center, Cleveland.
Dr. Dedousis and colleagues conducted a retrospective analysis of patients from Surveillance, Epidemiology, and End Results–Medicare databases between 2007 and 2014 with breast cancer. The study included data from 137,324 patients diagnosed between 2007 and 2012, before the widespread use of immunotherapy. 27% of patients had an autoimmune disease, most commonly rheumatoid arthritis (23%), psoriasis (2.4%), and systemic lupus erythematosus (1.1%).
When all patients were included in the analysis, those with autoimmune disorders had slightly longer survival times, but these weren’t clinically significant. A subanalysis found a greater difference in survival.
The association appears more pronounced in metastatic cancer. Patients with stage 4 breast cancer and autoimmune disease had a longer mean overall survival (36 months vs. 30 months; hazard ratio, 1.46; P < .0001. Cancer-specific survival: HR, 1.39; P < .0001). Patients with autoimmune disease and stage 1-3 breast cancer had lower overall survival (P < .0001, P < 0.0001, and P = 0.026 respectively), compared with patients without autoimmune disease.
“What we thought was happening is that the lack of increased survival in stages 1 through 3 was hiding the increase in survival among the stage IV patients when looking at the overall cohort,” Dr. Dedousis said.
The retrospective nature of the study makes it impossible to draw any firm conclusions about causation. It could be that patients who have already been diagnosed with an autoimmune disease are more vigilant about going to health checkups. “There are other possible explanations, but the one that’s most interesting to us is that their immune system is involved in fighting the cancer. Our study certainly didn’t prove that, but it’s suggesting that’s a possibility,” Dr. Dedousis said.
He and his coauthors anticipate conducting similar studies in other cancers to see if there are similar relationships. Some preliminary work has already suggested something similar in lung cancer. “I think demonstrating this in a few kinds of cancer goes part of the way towards showing that this is a real biological phenomenon,” he said.
Another research avenue is to examine the immune systems and pathology specimens in patients with both an autoimmune disease and cancer to see if there is a greater immune response within the tumor. If so, that could suggest new immunotherapy strategies.
Another possibility is to look at the specific immune pathways within “protective” autoimmune conditions. “For the sake of argument, if we find a particular autoimmune condition is improving survival across multiple kinds of cancers, we could look at those pathways that are specifically involved in that autoimmune condition. It might help us identify a target for drug development,” Dr. Dedousis said.
Asked why a potential benefit might be more apparent in late-stage disease, he suggested that, in early-stage breast cancer, surgery and other treatments may be so effective that the immune system’s role only rarely makes a difference. It could play a larger role in late-stage disease when there are less effective therapies. It could also be that the immune system doesn’t recognize the cancer until it has spread beyond the regional lymph nodes on its way to metastasizing.
According to the National Cancer Institute, 10%-30% of people with cancer also have an autoimmune disease.
Dr. Dedousis has no relevant financial disclosures.
CHICAGO – Comorbid autoimmune disease is associated with a greater chance of survival among women with stage IV breast cancer, according to a retrospective study presented at the annual meeting of the American Society of Clinical Oncology.
“It’s counterintuitive that, if you have two diseases instead of one, that you live longer, so then we had to scratch our heads a little bit and think about why these people are living longer,” said lead author Demitrios Dedousis, MD, University Hospitals, Case Medical Center, Cleveland.
Dr. Dedousis and colleagues conducted a retrospective analysis of patients from Surveillance, Epidemiology, and End Results–Medicare databases between 2007 and 2014 with breast cancer. The study included data from 137,324 patients diagnosed between 2007 and 2012, before the widespread use of immunotherapy. 27% of patients had an autoimmune disease, most commonly rheumatoid arthritis (23%), psoriasis (2.4%), and systemic lupus erythematosus (1.1%).
When all patients were included in the analysis, those with autoimmune disorders had slightly longer survival times, but these weren’t clinically significant. A subanalysis found a greater difference in survival.
The association appears more pronounced in metastatic cancer. Patients with stage 4 breast cancer and autoimmune disease had a longer mean overall survival (36 months vs. 30 months; hazard ratio, 1.46; P < .0001. Cancer-specific survival: HR, 1.39; P < .0001). Patients with autoimmune disease and stage 1-3 breast cancer had lower overall survival (P < .0001, P < 0.0001, and P = 0.026 respectively), compared with patients without autoimmune disease.
“What we thought was happening is that the lack of increased survival in stages 1 through 3 was hiding the increase in survival among the stage IV patients when looking at the overall cohort,” Dr. Dedousis said.
The retrospective nature of the study makes it impossible to draw any firm conclusions about causation. It could be that patients who have already been diagnosed with an autoimmune disease are more vigilant about going to health checkups. “There are other possible explanations, but the one that’s most interesting to us is that their immune system is involved in fighting the cancer. Our study certainly didn’t prove that, but it’s suggesting that’s a possibility,” Dr. Dedousis said.
He and his coauthors anticipate conducting similar studies in other cancers to see if there are similar relationships. Some preliminary work has already suggested something similar in lung cancer. “I think demonstrating this in a few kinds of cancer goes part of the way towards showing that this is a real biological phenomenon,” he said.
Another research avenue is to examine the immune systems and pathology specimens in patients with both an autoimmune disease and cancer to see if there is a greater immune response within the tumor. If so, that could suggest new immunotherapy strategies.
Another possibility is to look at the specific immune pathways within “protective” autoimmune conditions. “For the sake of argument, if we find a particular autoimmune condition is improving survival across multiple kinds of cancers, we could look at those pathways that are specifically involved in that autoimmune condition. It might help us identify a target for drug development,” Dr. Dedousis said.
Asked why a potential benefit might be more apparent in late-stage disease, he suggested that, in early-stage breast cancer, surgery and other treatments may be so effective that the immune system’s role only rarely makes a difference. It could play a larger role in late-stage disease when there are less effective therapies. It could also be that the immune system doesn’t recognize the cancer until it has spread beyond the regional lymph nodes on its way to metastasizing.
According to the National Cancer Institute, 10%-30% of people with cancer also have an autoimmune disease.
Dr. Dedousis has no relevant financial disclosures.
AT ASCO 2022
California doctor to pay $9.5 million in Medicare, Medi-Cal fraud scheme
Part of the payment was a settlement in a civil case in which Minas Kochumian, MD, an internist who ran a solo practice in Northridge, Calif., was accused of submitting claims to Medicare and Medi-Cal for procedures, services, and tests that were never performed. The procedures he falsely billed for included injecting a medication for treating osteoarthritis and osteoporosis, draining tailbone cysts, and removal of various growths.
As part of the settlement, Dr. Kochumian admitted that he intentionally submitted false claims with the intent to deceive the United States and the State of California. The damages and penalties were possible under the federal False Claims Act and the California False Claims Act.
According to the Medical Board of California, Dr. Kochumian’s license is current and set to expire next July.
The allegations against Dr. Kochumian were first brought to the attention of authorities in a whistleblower lawsuit filed by Elize Oganesyan, Dr. Kochumian’s former medical assistant, and Damon Davies, former information technology consultant for the practice. Among her other duties, Ms. Oganesyan was responsible for verifying insurance eligibility and obtaining authorization for drugs, procedures, services, and tests.
The medical assistant first realized that something was amiss when a patient brought her a Medicare Explanation of Benefits document that included charges for an injection the practice had not administered, according to court records. Ms. Oganesyan then realized the clinic was filing claims for other services that were never provided. She stated in the original complaint that the clinic did not even have the necessary equipment for providing some of these tests — skin allergy tests, for example.
The False Claims Act permits private parties to sue on behalf of the government for false claims for government funds and to receive a share of any recovery. Ms. Oganesyan and Davies will receive more than $1.75 million as their share of the recovery. The whistleblowers’ claims for attorneys’ fees are not resolved by this settlement, according to a statement from the U.S. Attorney’s Office, Eastern District of California.
The $9.5 million payment includes $5.4 million owed by Dr. Kochumian as criminal restitution following his guilty plea to one count of healthcare fraud in a separate criminal case filed in the Central District of California. In addition to the fine, Dr. Kochumian was sentenced to 41 months in prison, according to a statement by California Attorney General Rob Bonta.
“When doctors misuse the state’s Medi-Cal funds, they violate their Hippocratic Oath by harming a program which exists to help California’s Medi-Cal population, including the elderly, the sick, and the vulnerable,” said Mr. Bonta. “Dr. Kochumian’s alleged misconduct violated the trust of the patients in his care, and he selfishly pocketed funds that would otherwise have gone toward critical publicly funded healthcare services.”
A version of this article first appeared on Medscape.com.
Part of the payment was a settlement in a civil case in which Minas Kochumian, MD, an internist who ran a solo practice in Northridge, Calif., was accused of submitting claims to Medicare and Medi-Cal for procedures, services, and tests that were never performed. The procedures he falsely billed for included injecting a medication for treating osteoarthritis and osteoporosis, draining tailbone cysts, and removal of various growths.
As part of the settlement, Dr. Kochumian admitted that he intentionally submitted false claims with the intent to deceive the United States and the State of California. The damages and penalties were possible under the federal False Claims Act and the California False Claims Act.
According to the Medical Board of California, Dr. Kochumian’s license is current and set to expire next July.
The allegations against Dr. Kochumian were first brought to the attention of authorities in a whistleblower lawsuit filed by Elize Oganesyan, Dr. Kochumian’s former medical assistant, and Damon Davies, former information technology consultant for the practice. Among her other duties, Ms. Oganesyan was responsible for verifying insurance eligibility and obtaining authorization for drugs, procedures, services, and tests.
The medical assistant first realized that something was amiss when a patient brought her a Medicare Explanation of Benefits document that included charges for an injection the practice had not administered, according to court records. Ms. Oganesyan then realized the clinic was filing claims for other services that were never provided. She stated in the original complaint that the clinic did not even have the necessary equipment for providing some of these tests — skin allergy tests, for example.
The False Claims Act permits private parties to sue on behalf of the government for false claims for government funds and to receive a share of any recovery. Ms. Oganesyan and Davies will receive more than $1.75 million as their share of the recovery. The whistleblowers’ claims for attorneys’ fees are not resolved by this settlement, according to a statement from the U.S. Attorney’s Office, Eastern District of California.
The $9.5 million payment includes $5.4 million owed by Dr. Kochumian as criminal restitution following his guilty plea to one count of healthcare fraud in a separate criminal case filed in the Central District of California. In addition to the fine, Dr. Kochumian was sentenced to 41 months in prison, according to a statement by California Attorney General Rob Bonta.
“When doctors misuse the state’s Medi-Cal funds, they violate their Hippocratic Oath by harming a program which exists to help California’s Medi-Cal population, including the elderly, the sick, and the vulnerable,” said Mr. Bonta. “Dr. Kochumian’s alleged misconduct violated the trust of the patients in his care, and he selfishly pocketed funds that would otherwise have gone toward critical publicly funded healthcare services.”
A version of this article first appeared on Medscape.com.
Part of the payment was a settlement in a civil case in which Minas Kochumian, MD, an internist who ran a solo practice in Northridge, Calif., was accused of submitting claims to Medicare and Medi-Cal for procedures, services, and tests that were never performed. The procedures he falsely billed for included injecting a medication for treating osteoarthritis and osteoporosis, draining tailbone cysts, and removal of various growths.
As part of the settlement, Dr. Kochumian admitted that he intentionally submitted false claims with the intent to deceive the United States and the State of California. The damages and penalties were possible under the federal False Claims Act and the California False Claims Act.
According to the Medical Board of California, Dr. Kochumian’s license is current and set to expire next July.
The allegations against Dr. Kochumian were first brought to the attention of authorities in a whistleblower lawsuit filed by Elize Oganesyan, Dr. Kochumian’s former medical assistant, and Damon Davies, former information technology consultant for the practice. Among her other duties, Ms. Oganesyan was responsible for verifying insurance eligibility and obtaining authorization for drugs, procedures, services, and tests.
The medical assistant first realized that something was amiss when a patient brought her a Medicare Explanation of Benefits document that included charges for an injection the practice had not administered, according to court records. Ms. Oganesyan then realized the clinic was filing claims for other services that were never provided. She stated in the original complaint that the clinic did not even have the necessary equipment for providing some of these tests — skin allergy tests, for example.
The False Claims Act permits private parties to sue on behalf of the government for false claims for government funds and to receive a share of any recovery. Ms. Oganesyan and Davies will receive more than $1.75 million as their share of the recovery. The whistleblowers’ claims for attorneys’ fees are not resolved by this settlement, according to a statement from the U.S. Attorney’s Office, Eastern District of California.
The $9.5 million payment includes $5.4 million owed by Dr. Kochumian as criminal restitution following his guilty plea to one count of healthcare fraud in a separate criminal case filed in the Central District of California. In addition to the fine, Dr. Kochumian was sentenced to 41 months in prison, according to a statement by California Attorney General Rob Bonta.
“When doctors misuse the state’s Medi-Cal funds, they violate their Hippocratic Oath by harming a program which exists to help California’s Medi-Cal population, including the elderly, the sick, and the vulnerable,” said Mr. Bonta. “Dr. Kochumian’s alleged misconduct violated the trust of the patients in his care, and he selfishly pocketed funds that would otherwise have gone toward critical publicly funded healthcare services.”
A version of this article first appeared on Medscape.com.