User login
Proteins may be therapeutic targets for AML subtype

Image by Eric Smith
Preclinical research suggests a pair of histone-modifying proteins may be promising therapeutic targets for NPM1-mutated acute myeloid leukemia (AML).
Investigators found that these proteins—MLL and DOT1L—play key roles in NPM1-mutated AML.
Pharmacologic inhibition of either protein alone produced anti-leukemic activity in vitro and in vivo, but inhibiting both proteins together had a more profound effect.
Michael Kühn, MD, of the Mainz University Medical Center in Mainz, Germany, and his colleagues reported these findings in Cancer Discovery.
The investigators noted that nearly all NPM1-mutated AMLs are characterized by aberrant HOX expression, and FLT3 is concomitantly mutated in roughly 60% of these cases. However, it hasn’t been clear how mutant NPM1 cells maintain aberrant gene expression.
With this study, Dr Kühn and his colleagues showed that MLL1 and DOT1L control HOX and FLT3 expression and differentiation in NPM1-mutated AML.
The investigators were able to demonstrate that survival of NPM1-mutated AML cells depends on these 2 proteins. And NPM1-mutated AML is “exceptionally dependent” on the menin binding site in MLL1.
The team tested MI-503, a menin–MLL1 inhibitor, and the DOT1L inhibitor EPZ4777 in human and murine models of NPM1-mutated AML.
Each of the drugs reduced the activity of HOX genes in NPM1-mutated AML cells, but combining the drugs resulted in near-complete inactivation of HOX genes.
When given alone, EPZ4777 and MI-503 each reduced the proliferation and colony-forming potential of NPM1-mutated AML cells in vitro. And each of the drugs prolonged survival in mouse models of NPM1-mutated AML.
However, EPZ4777 and MI-503 given in combination significantly delayed the onset of leukemia and significantly prolonged survival when compared to either drug given alone.
The investigators said this suggests that inhibiting both DOT1L and menin–MLL1 affects leukemia-initiating cells, and this approach represents the first molecularly targeted treatment of NPM1-mutated AML that works by reversing a key mechanism of leukemogenesis.
They added that this research paves the way for trials assessing EPZ4777 and MI-503 in patients with NPM1-mutated AML. ![]()
Image by Eric Smith
Preclinical research suggests a pair of histone-modifying proteins may be promising therapeutic targets for NPM1-mutated acute myeloid leukemia (AML).
Investigators found that these proteins—MLL and DOT1L—play key roles in NPM1-mutated AML.
Pharmacologic inhibition of either protein alone produced anti-leukemic activity in vitro and in vivo, but inhibiting both proteins together had a more profound effect.
Michael Kühn, MD, of the Mainz University Medical Center in Mainz, Germany, and his colleagues reported these findings in Cancer Discovery.
The investigators noted that nearly all NPM1-mutated AMLs are characterized by aberrant HOX expression, and FLT3 is concomitantly mutated in roughly 60% of these cases. However, it hasn’t been clear how mutant NPM1 cells maintain aberrant gene expression.
With this study, Dr Kühn and his colleagues showed that MLL1 and DOT1L control HOX and FLT3 expression and differentiation in NPM1-mutated AML.
The investigators were able to demonstrate that survival of NPM1-mutated AML cells depends on these 2 proteins. And NPM1-mutated AML is “exceptionally dependent” on the menin binding site in MLL1.
The team tested MI-503, a menin–MLL1 inhibitor, and the DOT1L inhibitor EPZ4777 in human and murine models of NPM1-mutated AML.
Each of the drugs reduced the activity of HOX genes in NPM1-mutated AML cells, but combining the drugs resulted in near-complete inactivation of HOX genes.
When given alone, EPZ4777 and MI-503 each reduced the proliferation and colony-forming potential of NPM1-mutated AML cells in vitro. And each of the drugs prolonged survival in mouse models of NPM1-mutated AML.
However, EPZ4777 and MI-503 given in combination significantly delayed the onset of leukemia and significantly prolonged survival when compared to either drug given alone.
The investigators said this suggests that inhibiting both DOT1L and menin–MLL1 affects leukemia-initiating cells, and this approach represents the first molecularly targeted treatment of NPM1-mutated AML that works by reversing a key mechanism of leukemogenesis.
They added that this research paves the way for trials assessing EPZ4777 and MI-503 in patients with NPM1-mutated AML. ![]()
Image by Eric Smith
Preclinical research suggests a pair of histone-modifying proteins may be promising therapeutic targets for NPM1-mutated acute myeloid leukemia (AML).
Investigators found that these proteins—MLL and DOT1L—play key roles in NPM1-mutated AML.
Pharmacologic inhibition of either protein alone produced anti-leukemic activity in vitro and in vivo, but inhibiting both proteins together had a more profound effect.
Michael Kühn, MD, of the Mainz University Medical Center in Mainz, Germany, and his colleagues reported these findings in Cancer Discovery.
The investigators noted that nearly all NPM1-mutated AMLs are characterized by aberrant HOX expression, and FLT3 is concomitantly mutated in roughly 60% of these cases. However, it hasn’t been clear how mutant NPM1 cells maintain aberrant gene expression.
With this study, Dr Kühn and his colleagues showed that MLL1 and DOT1L control HOX and FLT3 expression and differentiation in NPM1-mutated AML.
The investigators were able to demonstrate that survival of NPM1-mutated AML cells depends on these 2 proteins. And NPM1-mutated AML is “exceptionally dependent” on the menin binding site in MLL1.
The team tested MI-503, a menin–MLL1 inhibitor, and the DOT1L inhibitor EPZ4777 in human and murine models of NPM1-mutated AML.
Each of the drugs reduced the activity of HOX genes in NPM1-mutated AML cells, but combining the drugs resulted in near-complete inactivation of HOX genes.
When given alone, EPZ4777 and MI-503 each reduced the proliferation and colony-forming potential of NPM1-mutated AML cells in vitro. And each of the drugs prolonged survival in mouse models of NPM1-mutated AML.
However, EPZ4777 and MI-503 given in combination significantly delayed the onset of leukemia and significantly prolonged survival when compared to either drug given alone.
The investigators said this suggests that inhibiting both DOT1L and menin–MLL1 affects leukemia-initiating cells, and this approach represents the first molecularly targeted treatment of NPM1-mutated AML that works by reversing a key mechanism of leukemogenesis.
They added that this research paves the way for trials assessing EPZ4777 and MI-503 in patients with NPM1-mutated AML. ![]()
CHMP recommends conditional approval of drug for CLL

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has adopted a positive opinion of venetoclax (Venclyxto™).
The CHMP is recommending that venetoclax receive conditional marketing authorization to treat adults with chronic lymphocytic leukemia (CLL) who have 17p deletion or TP53 mutation and are unsuitable for or have failed treatment with an inhibitor of the B-cell receptor pathway.
The CHMP is also recommending the conditional authorization of venetoclax as a treatment for adults with CLL who do not have 17p deletion or TP53 mutation but have failed both chemo immunotherapy and treatment with an inhibitor of the B-cell receptor pathway.
The European Commission (EC) will review the CHMP’s opinion and is expected to make a final decision about venetoclax in late 2016.
If the EC follows the CHMP’s recommendations, venetoclax will become the first BCL-2 inhibitor approved for use in Europe. The authorization will be valid in all member states of the European Union, as well as Iceland, Liechtenstein, and Norway.
Conditional marketing authorization represents an expedited path for approval. The EC grants conditional marketing authorization to products whose benefits are thought to outweigh their risks, products that address unmet needs, and products that are expected to provide a significant public health benefit.
Conditional marketing authorization is granted before pivotal registration studies of a product are completed, but the company developing the product is required to complete post-marketing studies showing that the product provides a clinical benefit.
Venetoclax is being developed by AbbVie and Genentech, a member of the Roche Group. The drug is jointly commercialized by the companies in the US and by AbbVie outside of the US.
Venetoclax is currently approved for use in Argentina, Canada, Puerto Rico, and the US. The drug is being evaluated in phase 3 trials for the treatment of relapsed, refractory, and previously untreated CLL.
Phase 2 trial
Results from a phase 2 trial of venetoclax in CLL (M13-982, NCT01889186) were published in The Lancet Oncology in June. The trial enrolled 107 patients with relapsed or refractory CLL and 17p deletion.
Patients received venetoclax at 400 mg once daily following a weekly ramp-up schedule for the first 5 weeks. The primary endpoint was overall response rate, as determined by an independent review committee.
At a median follow-up of 12.1 months, 85 patients had responded to treatment, for an overall response rate of 79%.
Eight patients (8%) achieved a complete response or complete response with incomplete count recovery, 3 (3%) had a near-partial response, and 74 (69%) had a partial response. Twenty-two patients (21%) did not respond.
At the time of analysis, the median duration of response had not been reached. The same was true for progression-free survival and overall survival. The progression-free survival estimate for 12 months was 72%, and the overall survival estimate was 87%.
The incidence of treatment-emergent adverse events was 96%. The most frequent grade 3/4 adverse events were neutropenia (40%), infection (20%), anemia (18%), and thrombocytopenia (15%).
The incidence of serious adverse events was 55%. The most common of these were pyrexia (7%), autoimmune hemolytic anemia (7%), pneumonia (6%), and febrile neutropenia (5%).
Grade 3 laboratory tumor lysis syndrome (TLS) was reported in 5 patients during the ramp-up period only. Three of these patients continued on venetoclax, but 2 patients required a dose interruption of 1 day each.
In the past, TLS has caused deaths in patients receiving venetoclax. In response, AbbVie stopped dose-escalation in patients receiving the drug and suspended enrollment in phase 1 trials.
However, researchers subsequently found that a modified dosing schedule, prophylaxis, and patient monitoring can reduce the risk of TLS. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has adopted a positive opinion of venetoclax (Venclyxto™).
The CHMP is recommending that venetoclax receive conditional marketing authorization to treat adults with chronic lymphocytic leukemia (CLL) who have 17p deletion or TP53 mutation and are unsuitable for or have failed treatment with an inhibitor of the B-cell receptor pathway.
The CHMP is also recommending the conditional authorization of venetoclax as a treatment for adults with CLL who do not have 17p deletion or TP53 mutation but have failed both chemo immunotherapy and treatment with an inhibitor of the B-cell receptor pathway.
The European Commission (EC) will review the CHMP’s opinion and is expected to make a final decision about venetoclax in late 2016.
If the EC follows the CHMP’s recommendations, venetoclax will become the first BCL-2 inhibitor approved for use in Europe. The authorization will be valid in all member states of the European Union, as well as Iceland, Liechtenstein, and Norway.
Conditional marketing authorization represents an expedited path for approval. The EC grants conditional marketing authorization to products whose benefits are thought to outweigh their risks, products that address unmet needs, and products that are expected to provide a significant public health benefit.
Conditional marketing authorization is granted before pivotal registration studies of a product are completed, but the company developing the product is required to complete post-marketing studies showing that the product provides a clinical benefit.
Venetoclax is being developed by AbbVie and Genentech, a member of the Roche Group. The drug is jointly commercialized by the companies in the US and by AbbVie outside of the US.
Venetoclax is currently approved for use in Argentina, Canada, Puerto Rico, and the US. The drug is being evaluated in phase 3 trials for the treatment of relapsed, refractory, and previously untreated CLL.
Phase 2 trial
Results from a phase 2 trial of venetoclax in CLL (M13-982, NCT01889186) were published in The Lancet Oncology in June. The trial enrolled 107 patients with relapsed or refractory CLL and 17p deletion.
Patients received venetoclax at 400 mg once daily following a weekly ramp-up schedule for the first 5 weeks. The primary endpoint was overall response rate, as determined by an independent review committee.
At a median follow-up of 12.1 months, 85 patients had responded to treatment, for an overall response rate of 79%.
Eight patients (8%) achieved a complete response or complete response with incomplete count recovery, 3 (3%) had a near-partial response, and 74 (69%) had a partial response. Twenty-two patients (21%) did not respond.
At the time of analysis, the median duration of response had not been reached. The same was true for progression-free survival and overall survival. The progression-free survival estimate for 12 months was 72%, and the overall survival estimate was 87%.
The incidence of treatment-emergent adverse events was 96%. The most frequent grade 3/4 adverse events were neutropenia (40%), infection (20%), anemia (18%), and thrombocytopenia (15%).
The incidence of serious adverse events was 55%. The most common of these were pyrexia (7%), autoimmune hemolytic anemia (7%), pneumonia (6%), and febrile neutropenia (5%).
Grade 3 laboratory tumor lysis syndrome (TLS) was reported in 5 patients during the ramp-up period only. Three of these patients continued on venetoclax, but 2 patients required a dose interruption of 1 day each.
In the past, TLS has caused deaths in patients receiving venetoclax. In response, AbbVie stopped dose-escalation in patients receiving the drug and suspended enrollment in phase 1 trials.
However, researchers subsequently found that a modified dosing schedule, prophylaxis, and patient monitoring can reduce the risk of TLS. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has adopted a positive opinion of venetoclax (Venclyxto™).
The CHMP is recommending that venetoclax receive conditional marketing authorization to treat adults with chronic lymphocytic leukemia (CLL) who have 17p deletion or TP53 mutation and are unsuitable for or have failed treatment with an inhibitor of the B-cell receptor pathway.
The CHMP is also recommending the conditional authorization of venetoclax as a treatment for adults with CLL who do not have 17p deletion or TP53 mutation but have failed both chemo immunotherapy and treatment with an inhibitor of the B-cell receptor pathway.
The European Commission (EC) will review the CHMP’s opinion and is expected to make a final decision about venetoclax in late 2016.
If the EC follows the CHMP’s recommendations, venetoclax will become the first BCL-2 inhibitor approved for use in Europe. The authorization will be valid in all member states of the European Union, as well as Iceland, Liechtenstein, and Norway.
Conditional marketing authorization represents an expedited path for approval. The EC grants conditional marketing authorization to products whose benefits are thought to outweigh their risks, products that address unmet needs, and products that are expected to provide a significant public health benefit.
Conditional marketing authorization is granted before pivotal registration studies of a product are completed, but the company developing the product is required to complete post-marketing studies showing that the product provides a clinical benefit.
Venetoclax is being developed by AbbVie and Genentech, a member of the Roche Group. The drug is jointly commercialized by the companies in the US and by AbbVie outside of the US.
Venetoclax is currently approved for use in Argentina, Canada, Puerto Rico, and the US. The drug is being evaluated in phase 3 trials for the treatment of relapsed, refractory, and previously untreated CLL.
Phase 2 trial
Results from a phase 2 trial of venetoclax in CLL (M13-982, NCT01889186) were published in The Lancet Oncology in June. The trial enrolled 107 patients with relapsed or refractory CLL and 17p deletion.
Patients received venetoclax at 400 mg once daily following a weekly ramp-up schedule for the first 5 weeks. The primary endpoint was overall response rate, as determined by an independent review committee.
At a median follow-up of 12.1 months, 85 patients had responded to treatment, for an overall response rate of 79%.
Eight patients (8%) achieved a complete response or complete response with incomplete count recovery, 3 (3%) had a near-partial response, and 74 (69%) had a partial response. Twenty-two patients (21%) did not respond.
At the time of analysis, the median duration of response had not been reached. The same was true for progression-free survival and overall survival. The progression-free survival estimate for 12 months was 72%, and the overall survival estimate was 87%.
The incidence of treatment-emergent adverse events was 96%. The most frequent grade 3/4 adverse events were neutropenia (40%), infection (20%), anemia (18%), and thrombocytopenia (15%).
The incidence of serious adverse events was 55%. The most common of these were pyrexia (7%), autoimmune hemolytic anemia (7%), pneumonia (6%), and febrile neutropenia (5%).
Grade 3 laboratory tumor lysis syndrome (TLS) was reported in 5 patients during the ramp-up period only. Three of these patients continued on venetoclax, but 2 patients required a dose interruption of 1 day each.
In the past, TLS has caused deaths in patients receiving venetoclax. In response, AbbVie stopped dose-escalation in patients receiving the drug and suspended enrollment in phase 1 trials.
However, researchers subsequently found that a modified dosing schedule, prophylaxis, and patient monitoring can reduce the risk of TLS. ![]()
Gene-editing approach is ‘important advance’ in SCD, doc says
sickle cell disease
Image by Graham Beards
Researchers have described a gene-editing technique that can correct the sickle cell mutation in hematopoietic stem and progenitor cells (HSPCs) isolated from patients with sickle cell disease (SCD).
The investigators said these edited HSPCs produced wild-type adult and fetal hemoglobin.
The HSPCs were also able to engraft in mice and maintained their SCD gene edits long-term without showing any signs of side effects.
“This is an important advance because, for the first time, we show a level of correction in stem cells that should be sufficient for a clinical benefit in persons with sickle cell anemia,” said Mark Walters, MD, of UCSF Benioff Children’s Hospital Oakland in California.
Dr Walters and his colleagues described this work in Science Translational Medicine.
The researchers said they used a ribonucleoprotein complex consisting of Cas9 protein and unmodified single guide RNA, together with a single-stranded DNA oligonucleotide donor, to enable efficient replacement of the SCD mutation in human HSPCs.
The team then differentiated pools of these HSPCs into enucleated erythrocytes and late-stage erythroblasts to measure hemoglobin production.
They said the edited HSPCs produced “substantial amounts” of adult wild-type hemoglobin. The cells also showed a decrease in sickle hemoglobin and an increase in fetal hemoglobin.
When implanted in mice, the edited HSPCs repopulated and maintained their SCD gene edits for 16 weeks, with no signs of side effects. (The mice were sacrificed at 16 weeks.)
“We’re very excited about the promise of this technology,” said study author Jacob Corn, PhD, of the University of California, Berkeley.
“There is still a lot of work to be done before this approach might be used in the clinic, but we’re hopeful that it will pave the way for new kinds of treatment for patients with sickle cell disease.”
In fact, Dr Corn and his lab have joined with Dr Walters to initiate an early phase clinical trial to test this gene-editing approach within the next 5 years.
The investigators also noted that the approach might be effective for treating other disorders, such as β-thalassemia, Wiskott-Aldrich syndrome, and Fanconi anemia.
“Sickle cell disease is just one of many blood disorders caused by a single mutation in the genome,” Dr Corn said. “It’s very possible that other researchers and clinicians could use this type of gene editing to explore ways to cure a large number of diseases.” ![]()
sickle cell disease
Image by Graham Beards
Researchers have described a gene-editing technique that can correct the sickle cell mutation in hematopoietic stem and progenitor cells (HSPCs) isolated from patients with sickle cell disease (SCD).
The investigators said these edited HSPCs produced wild-type adult and fetal hemoglobin.
The HSPCs were also able to engraft in mice and maintained their SCD gene edits long-term without showing any signs of side effects.
“This is an important advance because, for the first time, we show a level of correction in stem cells that should be sufficient for a clinical benefit in persons with sickle cell anemia,” said Mark Walters, MD, of UCSF Benioff Children’s Hospital Oakland in California.
Dr Walters and his colleagues described this work in Science Translational Medicine.
The researchers said they used a ribonucleoprotein complex consisting of Cas9 protein and unmodified single guide RNA, together with a single-stranded DNA oligonucleotide donor, to enable efficient replacement of the SCD mutation in human HSPCs.
The team then differentiated pools of these HSPCs into enucleated erythrocytes and late-stage erythroblasts to measure hemoglobin production.
They said the edited HSPCs produced “substantial amounts” of adult wild-type hemoglobin. The cells also showed a decrease in sickle hemoglobin and an increase in fetal hemoglobin.
When implanted in mice, the edited HSPCs repopulated and maintained their SCD gene edits for 16 weeks, with no signs of side effects. (The mice were sacrificed at 16 weeks.)
“We’re very excited about the promise of this technology,” said study author Jacob Corn, PhD, of the University of California, Berkeley.
“There is still a lot of work to be done before this approach might be used in the clinic, but we’re hopeful that it will pave the way for new kinds of treatment for patients with sickle cell disease.”
In fact, Dr Corn and his lab have joined with Dr Walters to initiate an early phase clinical trial to test this gene-editing approach within the next 5 years.
The investigators also noted that the approach might be effective for treating other disorders, such as β-thalassemia, Wiskott-Aldrich syndrome, and Fanconi anemia.
“Sickle cell disease is just one of many blood disorders caused by a single mutation in the genome,” Dr Corn said. “It’s very possible that other researchers and clinicians could use this type of gene editing to explore ways to cure a large number of diseases.” ![]()
sickle cell disease
Image by Graham Beards
Researchers have described a gene-editing technique that can correct the sickle cell mutation in hematopoietic stem and progenitor cells (HSPCs) isolated from patients with sickle cell disease (SCD).
The investigators said these edited HSPCs produced wild-type adult and fetal hemoglobin.
The HSPCs were also able to engraft in mice and maintained their SCD gene edits long-term without showing any signs of side effects.
“This is an important advance because, for the first time, we show a level of correction in stem cells that should be sufficient for a clinical benefit in persons with sickle cell anemia,” said Mark Walters, MD, of UCSF Benioff Children’s Hospital Oakland in California.
Dr Walters and his colleagues described this work in Science Translational Medicine.
The researchers said they used a ribonucleoprotein complex consisting of Cas9 protein and unmodified single guide RNA, together with a single-stranded DNA oligonucleotide donor, to enable efficient replacement of the SCD mutation in human HSPCs.
The team then differentiated pools of these HSPCs into enucleated erythrocytes and late-stage erythroblasts to measure hemoglobin production.
They said the edited HSPCs produced “substantial amounts” of adult wild-type hemoglobin. The cells also showed a decrease in sickle hemoglobin and an increase in fetal hemoglobin.
When implanted in mice, the edited HSPCs repopulated and maintained their SCD gene edits for 16 weeks, with no signs of side effects. (The mice were sacrificed at 16 weeks.)
“We’re very excited about the promise of this technology,” said study author Jacob Corn, PhD, of the University of California, Berkeley.
“There is still a lot of work to be done before this approach might be used in the clinic, but we’re hopeful that it will pave the way for new kinds of treatment for patients with sickle cell disease.”
In fact, Dr Corn and his lab have joined with Dr Walters to initiate an early phase clinical trial to test this gene-editing approach within the next 5 years.
The investigators also noted that the approach might be effective for treating other disorders, such as β-thalassemia, Wiskott-Aldrich syndrome, and Fanconi anemia.
“Sickle cell disease is just one of many blood disorders caused by a single mutation in the genome,” Dr Corn said. “It’s very possible that other researchers and clinicians could use this type of gene editing to explore ways to cure a large number of diseases.” ![]()
Combo could treat AML, other cancers

A novel combination has shown promise for treating acute myeloid leukemia (AML) and other cancers, according to preclinical research published in Cancer Cell.
Researchers found that combining a DNMT inhibitor and a PARP inhibitor greatly increases the drugs’ anti-tumor activity, and the combination could be effective in malignancies that are not responsive to PARP inhibitors or DNMT inhibitors alone.
Experiments showed that, when combined, the 2 types of inhibitors cause interactions that significantly disrupt cancer cells’ ability to survive DNA damage.
“Our preclinical data suggest that combining low doses of these inhibitors will enhance the clinical effects of both drugs as a potential treatment for patients with AML,” said study author Feyruz V. Rassool, PhD, of the University of Maryland School of Medicine in Baltimore.
“Moreover, our initial data suggest that subtypes of AML with a poor prognosis are likely to be sensitive to this new therapeutic approach.”
Dr Rassool and her colleagues assessed the activity of a DNMT inhibitor—decitabine or 5-azacytidine—in combination with a PARP inhibitor—veliparib or talazoparib—against AML and breast cancer.
In both AML and breast cancer cells, combination treatment increased cytotoxicity and decreased clonogenicity, compared to treatment with either type of inhibitor alone.
The combination of 5-azacytidine and talazoparib produced “very robust responses” in 2 mouse models of AML (MV411 and MOLM14), according to the researchers.
“[It was] somewhat of a surprise that leukemia cells were this sensitive to the combination treatment,” said study author Stephen B. Baylin, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Medical Institutions in Baltimore.
“And if further research confirms our findings, it looks like it also could be useful for breast cancer and ovarian cancers for which PARP inhibitors have not been useful as yet.”
How the inhibitors work together
Dr Baylin noted that PARP helps repair naturally occurring breaks in strands of DNA, and some cancers rely more frequently on PARP than others.
“[PARP inhibitors] work according to how intensely and durably the PARP enzyme is trapped at certain DNA damage sites,” he explained. “If you can ramp up the duration and intensity of this trapping, you could potentially increase the efficacy of the drug[s].”
“We figured that if we pair 5-azacytidine and a PARP inhibitor like talazoparib, we may be able to increase PARP trapping at DNA damage sites.”
That’s because 5-azacytidine blocks proteins that attach gene-regulating methyl groups to DNA and traps those proteins on DNA. The proteins blocked by 5-azacytidine also interact with PARP enzymes at DNA damage sites.
In fact, the researchers did find that combining 5-azacytidine and talazoparib increased the time that PARP was trapped at sites of DNA damage in cancer cells. The time was extended from 30 minutes to 3-6 hours after treatment.
Next steps
Based on the results of this research, a clinical trial is planned to test whether low doses of decitabine and talazoparib can be safely combined and whether this therapy will be effective in AML patients.
The researchers are especially interested in testing the combination in patients who cannot receive intensive chemotherapy, whose leukemia is resistant to treatment, or who have relapsed after treatment.
“This is really a new paradigm mechanism that is being translated into a clinical trial,” Dr Rassool said. “It’s not just putting 2 drugs together.”
“We have shown in the laboratory that the proteins that these inhibitors target actually interact, so the effects of these inhibitors are enhanced through this interaction. Therein lies the novelty of this new approach.” ![]()
A novel combination has shown promise for treating acute myeloid leukemia (AML) and other cancers, according to preclinical research published in Cancer Cell.
Researchers found that combining a DNMT inhibitor and a PARP inhibitor greatly increases the drugs’ anti-tumor activity, and the combination could be effective in malignancies that are not responsive to PARP inhibitors or DNMT inhibitors alone.
Experiments showed that, when combined, the 2 types of inhibitors cause interactions that significantly disrupt cancer cells’ ability to survive DNA damage.
“Our preclinical data suggest that combining low doses of these inhibitors will enhance the clinical effects of both drugs as a potential treatment for patients with AML,” said study author Feyruz V. Rassool, PhD, of the University of Maryland School of Medicine in Baltimore.
“Moreover, our initial data suggest that subtypes of AML with a poor prognosis are likely to be sensitive to this new therapeutic approach.”
Dr Rassool and her colleagues assessed the activity of a DNMT inhibitor—decitabine or 5-azacytidine—in combination with a PARP inhibitor—veliparib or talazoparib—against AML and breast cancer.
In both AML and breast cancer cells, combination treatment increased cytotoxicity and decreased clonogenicity, compared to treatment with either type of inhibitor alone.
The combination of 5-azacytidine and talazoparib produced “very robust responses” in 2 mouse models of AML (MV411 and MOLM14), according to the researchers.
“[It was] somewhat of a surprise that leukemia cells were this sensitive to the combination treatment,” said study author Stephen B. Baylin, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Medical Institutions in Baltimore.
“And if further research confirms our findings, it looks like it also could be useful for breast cancer and ovarian cancers for which PARP inhibitors have not been useful as yet.”
How the inhibitors work together
Dr Baylin noted that PARP helps repair naturally occurring breaks in strands of DNA, and some cancers rely more frequently on PARP than others.
“[PARP inhibitors] work according to how intensely and durably the PARP enzyme is trapped at certain DNA damage sites,” he explained. “If you can ramp up the duration and intensity of this trapping, you could potentially increase the efficacy of the drug[s].”
“We figured that if we pair 5-azacytidine and a PARP inhibitor like talazoparib, we may be able to increase PARP trapping at DNA damage sites.”
That’s because 5-azacytidine blocks proteins that attach gene-regulating methyl groups to DNA and traps those proteins on DNA. The proteins blocked by 5-azacytidine also interact with PARP enzymes at DNA damage sites.
In fact, the researchers did find that combining 5-azacytidine and talazoparib increased the time that PARP was trapped at sites of DNA damage in cancer cells. The time was extended from 30 minutes to 3-6 hours after treatment.
Next steps
Based on the results of this research, a clinical trial is planned to test whether low doses of decitabine and talazoparib can be safely combined and whether this therapy will be effective in AML patients.
The researchers are especially interested in testing the combination in patients who cannot receive intensive chemotherapy, whose leukemia is resistant to treatment, or who have relapsed after treatment.
“This is really a new paradigm mechanism that is being translated into a clinical trial,” Dr Rassool said. “It’s not just putting 2 drugs together.”
“We have shown in the laboratory that the proteins that these inhibitors target actually interact, so the effects of these inhibitors are enhanced through this interaction. Therein lies the novelty of this new approach.” ![]()
A novel combination has shown promise for treating acute myeloid leukemia (AML) and other cancers, according to preclinical research published in Cancer Cell.
Researchers found that combining a DNMT inhibitor and a PARP inhibitor greatly increases the drugs’ anti-tumor activity, and the combination could be effective in malignancies that are not responsive to PARP inhibitors or DNMT inhibitors alone.
Experiments showed that, when combined, the 2 types of inhibitors cause interactions that significantly disrupt cancer cells’ ability to survive DNA damage.
“Our preclinical data suggest that combining low doses of these inhibitors will enhance the clinical effects of both drugs as a potential treatment for patients with AML,” said study author Feyruz V. Rassool, PhD, of the University of Maryland School of Medicine in Baltimore.
“Moreover, our initial data suggest that subtypes of AML with a poor prognosis are likely to be sensitive to this new therapeutic approach.”
Dr Rassool and her colleagues assessed the activity of a DNMT inhibitor—decitabine or 5-azacytidine—in combination with a PARP inhibitor—veliparib or talazoparib—against AML and breast cancer.
In both AML and breast cancer cells, combination treatment increased cytotoxicity and decreased clonogenicity, compared to treatment with either type of inhibitor alone.
The combination of 5-azacytidine and talazoparib produced “very robust responses” in 2 mouse models of AML (MV411 and MOLM14), according to the researchers.
“[It was] somewhat of a surprise that leukemia cells were this sensitive to the combination treatment,” said study author Stephen B. Baylin, MD, of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Medical Institutions in Baltimore.
“And if further research confirms our findings, it looks like it also could be useful for breast cancer and ovarian cancers for which PARP inhibitors have not been useful as yet.”
How the inhibitors work together
Dr Baylin noted that PARP helps repair naturally occurring breaks in strands of DNA, and some cancers rely more frequently on PARP than others.
“[PARP inhibitors] work according to how intensely and durably the PARP enzyme is trapped at certain DNA damage sites,” he explained. “If you can ramp up the duration and intensity of this trapping, you could potentially increase the efficacy of the drug[s].”
“We figured that if we pair 5-azacytidine and a PARP inhibitor like talazoparib, we may be able to increase PARP trapping at DNA damage sites.”
That’s because 5-azacytidine blocks proteins that attach gene-regulating methyl groups to DNA and traps those proteins on DNA. The proteins blocked by 5-azacytidine also interact with PARP enzymes at DNA damage sites.
In fact, the researchers did find that combining 5-azacytidine and talazoparib increased the time that PARP was trapped at sites of DNA damage in cancer cells. The time was extended from 30 minutes to 3-6 hours after treatment.
Next steps
Based on the results of this research, a clinical trial is planned to test whether low doses of decitabine and talazoparib can be safely combined and whether this therapy will be effective in AML patients.
The researchers are especially interested in testing the combination in patients who cannot receive intensive chemotherapy, whose leukemia is resistant to treatment, or who have relapsed after treatment.
“This is really a new paradigm mechanism that is being translated into a clinical trial,” Dr Rassool said. “It’s not just putting 2 drugs together.”
“We have shown in the laboratory that the proteins that these inhibitors target actually interact, so the effects of these inhibitors are enhanced through this interaction. Therein lies the novelty of this new approach.” ![]()
How a protein regulates blood cell fate
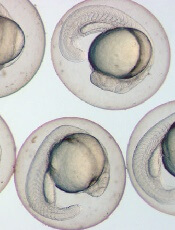
Image by Ian Johnston
Results of preclinical research explain the role endoglin plays in hematopoietic cell fate during embryogenesis.
Previous research showed that endoglin, a cell surface protein belonging to the TGF-beta receptor complex, is required for early hematopoietic lineage specification.
A new study shows that endoglin modulates the BMP and Wnt signaling pathways to encourage progenitor cells to develop into blood cells rather than cardiac cells.
This study was published in Nature Communications.
“During the early stages of development, cells have to make decisions very quickly,” said study author Rita Perlingeiro, PhD, of the University of Minnesota in Minneapolis.
“Fine-tuning of these early cell fate decisions can be easily disrupted by levels of key proteins within these cells. When one cell type is favored, this implies less of another. In this case, high levels of endoglin expression enhance the cell differentiation into blood cells, whereas cardiac cells are in deficit.”
Dr Perlingeiro and her colleagues made this discovery studying zebrafish and mouse models. The team wanted to pinpoint the mechanism underlying the dual function of endoglin in blood cell and cardiac cell fate.
The researchers found that endoglin is expressed in early mesoderm, and it marks both hematopoietic and cardiac progenitors.
Experiments showed that high levels of endoglin increase hematopoiesis while inhibiting cardiogenesis. And the levels of endoglin determine the activation of the BMP and Wnt signaling pathways.
With further investigation, the researchers identified JDP2, a member of the AP-1 transcription factor family, as an endoglin-dependent downstream target of Wnt signaling.
The team found that JDP2 expression is sufficient to establish blood cell fate when BMP and Wnt crosstalk is disturbed.
“The blood and heart systems are the first organs to develop in mammals, but the mechanisms regulating these earliest cell fate decisions are poorly understood,” Dr Perlingeiro said.
“By using multiple model systems, combined with specialized cell sorting technology and sequencing tools, our findings help uncover mechanisms previously unseen in the few cells engaged in these early development decisions.” ![]()
Image by Ian Johnston
Results of preclinical research explain the role endoglin plays in hematopoietic cell fate during embryogenesis.
Previous research showed that endoglin, a cell surface protein belonging to the TGF-beta receptor complex, is required for early hematopoietic lineage specification.
A new study shows that endoglin modulates the BMP and Wnt signaling pathways to encourage progenitor cells to develop into blood cells rather than cardiac cells.
This study was published in Nature Communications.
“During the early stages of development, cells have to make decisions very quickly,” said study author Rita Perlingeiro, PhD, of the University of Minnesota in Minneapolis.
“Fine-tuning of these early cell fate decisions can be easily disrupted by levels of key proteins within these cells. When one cell type is favored, this implies less of another. In this case, high levels of endoglin expression enhance the cell differentiation into blood cells, whereas cardiac cells are in deficit.”
Dr Perlingeiro and her colleagues made this discovery studying zebrafish and mouse models. The team wanted to pinpoint the mechanism underlying the dual function of endoglin in blood cell and cardiac cell fate.
The researchers found that endoglin is expressed in early mesoderm, and it marks both hematopoietic and cardiac progenitors.
Experiments showed that high levels of endoglin increase hematopoiesis while inhibiting cardiogenesis. And the levels of endoglin determine the activation of the BMP and Wnt signaling pathways.
With further investigation, the researchers identified JDP2, a member of the AP-1 transcription factor family, as an endoglin-dependent downstream target of Wnt signaling.
The team found that JDP2 expression is sufficient to establish blood cell fate when BMP and Wnt crosstalk is disturbed.
“The blood and heart systems are the first organs to develop in mammals, but the mechanisms regulating these earliest cell fate decisions are poorly understood,” Dr Perlingeiro said.
“By using multiple model systems, combined with specialized cell sorting technology and sequencing tools, our findings help uncover mechanisms previously unseen in the few cells engaged in these early development decisions.” ![]()
Image by Ian Johnston
Results of preclinical research explain the role endoglin plays in hematopoietic cell fate during embryogenesis.
Previous research showed that endoglin, a cell surface protein belonging to the TGF-beta receptor complex, is required for early hematopoietic lineage specification.
A new study shows that endoglin modulates the BMP and Wnt signaling pathways to encourage progenitor cells to develop into blood cells rather than cardiac cells.
This study was published in Nature Communications.
“During the early stages of development, cells have to make decisions very quickly,” said study author Rita Perlingeiro, PhD, of the University of Minnesota in Minneapolis.
“Fine-tuning of these early cell fate decisions can be easily disrupted by levels of key proteins within these cells. When one cell type is favored, this implies less of another. In this case, high levels of endoglin expression enhance the cell differentiation into blood cells, whereas cardiac cells are in deficit.”
Dr Perlingeiro and her colleagues made this discovery studying zebrafish and mouse models. The team wanted to pinpoint the mechanism underlying the dual function of endoglin in blood cell and cardiac cell fate.
The researchers found that endoglin is expressed in early mesoderm, and it marks both hematopoietic and cardiac progenitors.
Experiments showed that high levels of endoglin increase hematopoiesis while inhibiting cardiogenesis. And the levels of endoglin determine the activation of the BMP and Wnt signaling pathways.
With further investigation, the researchers identified JDP2, a member of the AP-1 transcription factor family, as an endoglin-dependent downstream target of Wnt signaling.
The team found that JDP2 expression is sufficient to establish blood cell fate when BMP and Wnt crosstalk is disturbed.
“The blood and heart systems are the first organs to develop in mammals, but the mechanisms regulating these earliest cell fate decisions are poorly understood,” Dr Perlingeiro said.
“By using multiple model systems, combined with specialized cell sorting technology and sequencing tools, our findings help uncover mechanisms previously unseen in the few cells engaged in these early development decisions.” ![]()
Device could aid treatment decisions in ALL, other cancers

A new device might help physicians choose the optimal treatment for cancer patients, according to research published in Nature Biotechnology.
The device was designed to predict responses to treatment by measuring individual cell growth after drug exposure.
Researchers found they could predict whether a particular drug would kill leukemia or glioblastoma cells, based on how the drug affected the cells’ mass.
“We’ve developed a functional assay that can measure drug response of individual cells while maintaining viability for downstream analysis such as sequencing,” said study author Scott Manalis, PhD, of the Massachusetts Institute of Technology in Cambridge.
He and his colleagues were inspired to develop their assay, in part, by a test that has been used for decades to choose antibiotics to treat bacterial infections. The antibiotic susceptibility test involves simply taking bacteria from a patient, exposing them to a range of antibiotics, and observing whether the bacteria grow or die.
To translate that approach to cancer, the researchers needed a way to rapidly measure cell responses to drugs, and to do it with a limited number of cells.
For the past several years, Dr Manalis’s lab has been developing a device known as a suspended microchannel resonator (SMR).
According to the researchers, the SMR can measure cell masses 10 to 100 times more accurately than any other technique. This allows for the precise calculation of growth rates of single cells over short periods of time.
For this study, Dr Manalis and his colleagues used the SMR to determine whether drug susceptibility could be predicted by measuring cancer cell growth rates following drug exposure.
The team analyzed cells from patients with different subtypes of glioblastoma and B-cell acute lymphocytic leukemia (ALL) that have previously been shown to be either sensitive or resistant to specific therapies—MDM2 inhibitors for glioblastoma and BCR-ABL inhibitors for ALL.
After exposing the cancer cells to the drugs, the researchers waited about 15 hours, then measured the cell’s growth rates. Each cell was measured several times over a period of 15 to 20 minutes, providing enough data for the team to calculate the mass accumulation rate.
They found that cells known to be susceptible to a given therapy changed the way they accumulate mass, whereas resistant cells continued to grow as if unaffected.
“We’re able to show that cells we know are sensitive to therapy respond by dramatically reducing their growth rate relative to cells that are resistant,” said study author Mark Stevens, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“And because the cells are still alive, we have the opportunity to study the same cells following our measurement.”
The researchers said a major advantage of this technique is that it can be done with very small numbers of cells. In the experiments with ALL cells, the team showed they could get accurate results with a droplet of blood containing about 1000 ALL cells.
Another advantage is the speed at which small changes in cell mass can be measured, said Anthony Letai, MD, PhD, of the Dana-Farber Cancer Institute.
“This system is well suited to making rapid measurements,” said Dr Letai, who was not involved in this study. “I look forward to seeing them apply this to many more cancers and many more drugs.”
The researchers are now using their technique to test cells’ susceptibility to drugs, then isolate the cells and sequence the RNA found in them, revealing which genes are turned on.
“Now that we have a way to identify cells that are not responding to a given therapy, we are excited about isolating these cells and analyzing them to understand mechanisms of resistance,” Dr Manalis said.
In another recent paper published in Nature Biotechnology, the researchers described a higher throughput version of the SMR device that can do in 1 day the same number of measurements that took several months with the device used in this study.
This is an important step toward making the approach suitable for clinical samples, Dr Manalis said. ![]()
A new device might help physicians choose the optimal treatment for cancer patients, according to research published in Nature Biotechnology.
The device was designed to predict responses to treatment by measuring individual cell growth after drug exposure.
Researchers found they could predict whether a particular drug would kill leukemia or glioblastoma cells, based on how the drug affected the cells’ mass.
“We’ve developed a functional assay that can measure drug response of individual cells while maintaining viability for downstream analysis such as sequencing,” said study author Scott Manalis, PhD, of the Massachusetts Institute of Technology in Cambridge.
He and his colleagues were inspired to develop their assay, in part, by a test that has been used for decades to choose antibiotics to treat bacterial infections. The antibiotic susceptibility test involves simply taking bacteria from a patient, exposing them to a range of antibiotics, and observing whether the bacteria grow or die.
To translate that approach to cancer, the researchers needed a way to rapidly measure cell responses to drugs, and to do it with a limited number of cells.
For the past several years, Dr Manalis’s lab has been developing a device known as a suspended microchannel resonator (SMR).
According to the researchers, the SMR can measure cell masses 10 to 100 times more accurately than any other technique. This allows for the precise calculation of growth rates of single cells over short periods of time.
For this study, Dr Manalis and his colleagues used the SMR to determine whether drug susceptibility could be predicted by measuring cancer cell growth rates following drug exposure.
The team analyzed cells from patients with different subtypes of glioblastoma and B-cell acute lymphocytic leukemia (ALL) that have previously been shown to be either sensitive or resistant to specific therapies—MDM2 inhibitors for glioblastoma and BCR-ABL inhibitors for ALL.
After exposing the cancer cells to the drugs, the researchers waited about 15 hours, then measured the cell’s growth rates. Each cell was measured several times over a period of 15 to 20 minutes, providing enough data for the team to calculate the mass accumulation rate.
They found that cells known to be susceptible to a given therapy changed the way they accumulate mass, whereas resistant cells continued to grow as if unaffected.
“We’re able to show that cells we know are sensitive to therapy respond by dramatically reducing their growth rate relative to cells that are resistant,” said study author Mark Stevens, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“And because the cells are still alive, we have the opportunity to study the same cells following our measurement.”
The researchers said a major advantage of this technique is that it can be done with very small numbers of cells. In the experiments with ALL cells, the team showed they could get accurate results with a droplet of blood containing about 1000 ALL cells.
Another advantage is the speed at which small changes in cell mass can be measured, said Anthony Letai, MD, PhD, of the Dana-Farber Cancer Institute.
“This system is well suited to making rapid measurements,” said Dr Letai, who was not involved in this study. “I look forward to seeing them apply this to many more cancers and many more drugs.”
The researchers are now using their technique to test cells’ susceptibility to drugs, then isolate the cells and sequence the RNA found in them, revealing which genes are turned on.
“Now that we have a way to identify cells that are not responding to a given therapy, we are excited about isolating these cells and analyzing them to understand mechanisms of resistance,” Dr Manalis said.
In another recent paper published in Nature Biotechnology, the researchers described a higher throughput version of the SMR device that can do in 1 day the same number of measurements that took several months with the device used in this study.
This is an important step toward making the approach suitable for clinical samples, Dr Manalis said. ![]()
A new device might help physicians choose the optimal treatment for cancer patients, according to research published in Nature Biotechnology.
The device was designed to predict responses to treatment by measuring individual cell growth after drug exposure.
Researchers found they could predict whether a particular drug would kill leukemia or glioblastoma cells, based on how the drug affected the cells’ mass.
“We’ve developed a functional assay that can measure drug response of individual cells while maintaining viability for downstream analysis such as sequencing,” said study author Scott Manalis, PhD, of the Massachusetts Institute of Technology in Cambridge.
He and his colleagues were inspired to develop their assay, in part, by a test that has been used for decades to choose antibiotics to treat bacterial infections. The antibiotic susceptibility test involves simply taking bacteria from a patient, exposing them to a range of antibiotics, and observing whether the bacteria grow or die.
To translate that approach to cancer, the researchers needed a way to rapidly measure cell responses to drugs, and to do it with a limited number of cells.
For the past several years, Dr Manalis’s lab has been developing a device known as a suspended microchannel resonator (SMR).
According to the researchers, the SMR can measure cell masses 10 to 100 times more accurately than any other technique. This allows for the precise calculation of growth rates of single cells over short periods of time.
For this study, Dr Manalis and his colleagues used the SMR to determine whether drug susceptibility could be predicted by measuring cancer cell growth rates following drug exposure.
The team analyzed cells from patients with different subtypes of glioblastoma and B-cell acute lymphocytic leukemia (ALL) that have previously been shown to be either sensitive or resistant to specific therapies—MDM2 inhibitors for glioblastoma and BCR-ABL inhibitors for ALL.
After exposing the cancer cells to the drugs, the researchers waited about 15 hours, then measured the cell’s growth rates. Each cell was measured several times over a period of 15 to 20 minutes, providing enough data for the team to calculate the mass accumulation rate.
They found that cells known to be susceptible to a given therapy changed the way they accumulate mass, whereas resistant cells continued to grow as if unaffected.
“We’re able to show that cells we know are sensitive to therapy respond by dramatically reducing their growth rate relative to cells that are resistant,” said study author Mark Stevens, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“And because the cells are still alive, we have the opportunity to study the same cells following our measurement.”
The researchers said a major advantage of this technique is that it can be done with very small numbers of cells. In the experiments with ALL cells, the team showed they could get accurate results with a droplet of blood containing about 1000 ALL cells.
Another advantage is the speed at which small changes in cell mass can be measured, said Anthony Letai, MD, PhD, of the Dana-Farber Cancer Institute.
“This system is well suited to making rapid measurements,” said Dr Letai, who was not involved in this study. “I look forward to seeing them apply this to many more cancers and many more drugs.”
The researchers are now using their technique to test cells’ susceptibility to drugs, then isolate the cells and sequence the RNA found in them, revealing which genes are turned on.
“Now that we have a way to identify cells that are not responding to a given therapy, we are excited about isolating these cells and analyzing them to understand mechanisms of resistance,” Dr Manalis said.
In another recent paper published in Nature Biotechnology, the researchers described a higher throughput version of the SMR device that can do in 1 day the same number of measurements that took several months with the device used in this study.
This is an important step toward making the approach suitable for clinical samples, Dr Manalis said. ![]()
Holographic imaging and deep learning diagnose malaria

Image by Peter H. Seeberger
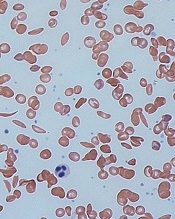
Scientists say they have devised a technique that can be used to diagnose malaria quickly and with clinically relevant accuracy.
The technique involves using computer deep learning and light-based, holographic scans to spot malaria-infected cells from an untouched blood sample without any help from a human.
The scientists believe this could form the basis of a fast, reliable malaria test that could be given by most anyone, anywhere in the field.
The team described the method in PLOS ONE.
“With this technique, the path is there to be able to process thousands of cells per minute,” said study author Adam Wax, PhD, of Duke University in Durham, North Carolina.
“That’s a huge improvement to the 40 minutes it currently takes a field technician to stain, prepare, and read a slide to personally look for infection.”
The new technique is based on a technology called quantitative phase spectroscopy. As a laser sweeps through the visible spectrum of light, sensors capture how each discrete light frequency interacts with a sample of blood.
The resulting data captures a holographic image that provides a wide array of information that can indicate a malaria infection.
“We identified 23 parameters that are statistically significant for spotting malaria,” said study author Han Sang Park, a doctoral student in Dr Wax’s lab.
For example, as the disease progresses, red blood cells decrease in volume, lose hemoglobin, and deform as the parasite within grows larger. This affects features such as cell volume, perimeter, shape, and center of mass.
“However, none of the parameters were reliable more than 90% of the time on their own,” Park said. “So we decided to use them all.”
“To be adopted, any new diagnostic device has to be just as reliable as a trained field worker with a microscope,” Dr Wax said. “Otherwise, even with a 90% success rate, you’d still miss more than 20 million [malaria] cases a year.”
To get a more accurate reading, Dr Wax and his colleagues turned to deep learning—a method by which computers teach themselves how to distinguish between different objects.
Feeding data on healthy and diseased cells into a computer enabled the deep learning program to determine which sets of measurements at which thresholds most clearly distinguished healthy cells from diseased cells.
When the scientists put the resulting algorithm to the test with hundreds of cells, the algorithm was able to correctly spot malaria more than 95% of the time—a number the team believes will increase as more cells are used to train the program.
The team noted that, because the technique breaks data-rich holograms down to just 23 numbers, tests can be easily transmitted in bulk. They said this is important for locations that often do not have reliable, fast internet connections.
Dr Wax and his colleagues are now looking to develop the technology into a diagnostic device through a startup company called M2 Photonics Innovations. They hope to show that a device based on this technology would be accurate and cost-efficient enough to be useful in the field.
Dr Wax has also received funding to begin exploring the use of the technique for spotting cancerous cells in blood samples. ![]()
Image by Peter H. Seeberger
Scientists say they have devised a technique that can be used to diagnose malaria quickly and with clinically relevant accuracy.
The technique involves using computer deep learning and light-based, holographic scans to spot malaria-infected cells from an untouched blood sample without any help from a human.
The scientists believe this could form the basis of a fast, reliable malaria test that could be given by most anyone, anywhere in the field.
The team described the method in PLOS ONE.
“With this technique, the path is there to be able to process thousands of cells per minute,” said study author Adam Wax, PhD, of Duke University in Durham, North Carolina.
“That’s a huge improvement to the 40 minutes it currently takes a field technician to stain, prepare, and read a slide to personally look for infection.”
The new technique is based on a technology called quantitative phase spectroscopy. As a laser sweeps through the visible spectrum of light, sensors capture how each discrete light frequency interacts with a sample of blood.
The resulting data captures a holographic image that provides a wide array of information that can indicate a malaria infection.
“We identified 23 parameters that are statistically significant for spotting malaria,” said study author Han Sang Park, a doctoral student in Dr Wax’s lab.
For example, as the disease progresses, red blood cells decrease in volume, lose hemoglobin, and deform as the parasite within grows larger. This affects features such as cell volume, perimeter, shape, and center of mass.
“However, none of the parameters were reliable more than 90% of the time on their own,” Park said. “So we decided to use them all.”
“To be adopted, any new diagnostic device has to be just as reliable as a trained field worker with a microscope,” Dr Wax said. “Otherwise, even with a 90% success rate, you’d still miss more than 20 million [malaria] cases a year.”
To get a more accurate reading, Dr Wax and his colleagues turned to deep learning—a method by which computers teach themselves how to distinguish between different objects.
Feeding data on healthy and diseased cells into a computer enabled the deep learning program to determine which sets of measurements at which thresholds most clearly distinguished healthy cells from diseased cells.
When the scientists put the resulting algorithm to the test with hundreds of cells, the algorithm was able to correctly spot malaria more than 95% of the time—a number the team believes will increase as more cells are used to train the program.
The team noted that, because the technique breaks data-rich holograms down to just 23 numbers, tests can be easily transmitted in bulk. They said this is important for locations that often do not have reliable, fast internet connections.
Dr Wax and his colleagues are now looking to develop the technology into a diagnostic device through a startup company called M2 Photonics Innovations. They hope to show that a device based on this technology would be accurate and cost-efficient enough to be useful in the field.
Dr Wax has also received funding to begin exploring the use of the technique for spotting cancerous cells in blood samples. ![]()
Image by Peter H. Seeberger
Scientists say they have devised a technique that can be used to diagnose malaria quickly and with clinically relevant accuracy.
The technique involves using computer deep learning and light-based, holographic scans to spot malaria-infected cells from an untouched blood sample without any help from a human.
The scientists believe this could form the basis of a fast, reliable malaria test that could be given by most anyone, anywhere in the field.
The team described the method in PLOS ONE.
“With this technique, the path is there to be able to process thousands of cells per minute,” said study author Adam Wax, PhD, of Duke University in Durham, North Carolina.
“That’s a huge improvement to the 40 minutes it currently takes a field technician to stain, prepare, and read a slide to personally look for infection.”
The new technique is based on a technology called quantitative phase spectroscopy. As a laser sweeps through the visible spectrum of light, sensors capture how each discrete light frequency interacts with a sample of blood.
The resulting data captures a holographic image that provides a wide array of information that can indicate a malaria infection.
“We identified 23 parameters that are statistically significant for spotting malaria,” said study author Han Sang Park, a doctoral student in Dr Wax’s lab.
For example, as the disease progresses, red blood cells decrease in volume, lose hemoglobin, and deform as the parasite within grows larger. This affects features such as cell volume, perimeter, shape, and center of mass.
“However, none of the parameters were reliable more than 90% of the time on their own,” Park said. “So we decided to use them all.”
“To be adopted, any new diagnostic device has to be just as reliable as a trained field worker with a microscope,” Dr Wax said. “Otherwise, even with a 90% success rate, you’d still miss more than 20 million [malaria] cases a year.”
To get a more accurate reading, Dr Wax and his colleagues turned to deep learning—a method by which computers teach themselves how to distinguish between different objects.
Feeding data on healthy and diseased cells into a computer enabled the deep learning program to determine which sets of measurements at which thresholds most clearly distinguished healthy cells from diseased cells.
When the scientists put the resulting algorithm to the test with hundreds of cells, the algorithm was able to correctly spot malaria more than 95% of the time—a number the team believes will increase as more cells are used to train the program.
The team noted that, because the technique breaks data-rich holograms down to just 23 numbers, tests can be easily transmitted in bulk. They said this is important for locations that often do not have reliable, fast internet connections.
Dr Wax and his colleagues are now looking to develop the technology into a diagnostic device through a startup company called M2 Photonics Innovations. They hope to show that a device based on this technology would be accurate and cost-efficient enough to be useful in the field.
Dr Wax has also received funding to begin exploring the use of the technique for spotting cancerous cells in blood samples.
‘Fresher’ RBCs no safer than standard RBCs, AABB says
![]()
Photo courtesy of UAB Hospital
AABB has released new guidelines on when to perform red blood cell (RBC) transfusions and the optimal duration of RBC storage.
The guidelines state that a restrictive transfusion threshold—waiting to transfuse until a patient’s hemoglobin level is 7-8 g/dL—is safe in most clinical settings.
And, for most patients, “fresh” RBCs—stored for less than 10 days—are no safer than standard-issue RBCs—stored for up to 42 days.
“One of the biggest controversies concerning transfusion therapy is whether older blood is harmful compared to fresher blood,” said guideline author Aaron Tobian, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
“Now, we have information that can accurately inform guidelines about red blood cell storage duration. If data suggest no harm from the use of standard-issue blood and fresher blood would only constrain the use of a limited resource, continuing with standard practice of using older blood is appropriate. The newly released guidelines now clearly inform the community.”
The guidelines were published in JAMA alongside a related editorial.
The recommendations in the guidelines are based on an analysis of randomized clinical trials in which researchers evaluated hemoglobin thresholds for RBC transfusion (trials conducted from 1950 through May 2016) and RBC storage duration (trials conducted from 1948 through May 2016).
For transfusion thresholds, there were 31 trials including 12,587 subjects. The results of these trials suggested that restrictive transfusion thresholds (transfusing when the hemoglobin level is 7-8 g/dL) were not associated with higher rates of adverse clinical outcomes when compared to liberal thresholds (transfusing when the hemoglobin level is 9-10 g/dL).
For RBC storage duration, there were 13 trials including 5515 subjects. The results suggested that transfusing fresher blood did not improve clinical outcomes.
Transfusion threshold
The guideline authors said it is good practice, when making transfusion decisions, to consider the patient’s hemoglobin level, the overall clinical context, patient preference, and alternative therapies.
However, in general, a hemoglobin level of 7 g/dL should serve as the threshold for transfusing adult patients who are hemodynamically stable, even if they are in critical care. This is a strong recommendation based on moderate-quality evidence.
“While the recommended threshold of 7 g/dL is consistent with previous AABB guidelines, the strength of the new recommendation reflects the quality and quantity of the new data, much of which was generated since 2012,” said guideline author Jeffrey Carson, MD, of Robert Wood Johnson University Hospital in New Brunswick, New Jersey.
“Clinically, these results show that no harm will come from waiting to transfuse a patient until the hemoglobin level reaches a lower point. The restrictive approach is associated with reductions in blood use, blood conservation, and lower expenses.”
The guidelines also state that, for patients with pre-existing cardiovascular disease and those undergoing cardiac or orthopedic surgery, the threshold should be 8 g/dL. This is a strong recommendation based on moderate-quality evidence.
Neither of the aforementioned recommendations apply to patients with acute coronary syndrome, severe thrombocytopenia, or chronic transfusion-dependent anemia.
Dr Carson said additional trials are needed to determine whether these patients benefit from transfusion at higher hemoglobin levels.
“We are about to embark on a large, international clinical trial supported by the NIH [National Institutes of Health] that will provide the evidence needed to determine the best course of action for patients who have had a heart attack,” he said.
Dr Carson and his colleagues also noted that, although the recommendations are based on the available evidence, the hemoglobin transfusion thresholds assessed may not be optimal. And the use of hemoglobin transfusion thresholds may be an imperfect surrogate for oxygen delivery.
Storage duration
The guidelines state that most patients, including neonates, should receive standard-issue RBCs (stored for 42 days or less) rather than limiting patients to only fresh RBCs (stored for less than 10 days). This is a strong recommendation based on moderate-quality evidence.
The trials analyzed showed that patients who received standard-issue RBCs faced no higher risk of complications—including 30-day mortality, myocardial infarction, cerebrovascular accident, rebleeding, pneumonia, or thromboembolism—than those who received fresh RBCs.
However, the guideline authors said the trial results may not apply to RBCs nearing their expiration date (stored for 35 to 42 days), as only a small proportion of patients in these trials were exposed to such RBCs.
Furthermore, the trials did not include patients undergoing a massive or exchange transfusion, neonates and children with underlying renal disease at higher risk of hyperkalemia, patients undergoing intrauterine transfusions, or patients with hemoglobinopathies requiring chronic transfusion support.
So the optimal RBC storage duration for these patients is unknown.
![]()
Photo courtesy of UAB Hospital
AABB has released new guidelines on when to perform red blood cell (RBC) transfusions and the optimal duration of RBC storage.
The guidelines state that a restrictive transfusion threshold—waiting to transfuse until a patient’s hemoglobin level is 7-8 g/dL—is safe in most clinical settings.
And, for most patients, “fresh” RBCs—stored for less than 10 days—are no safer than standard-issue RBCs—stored for up to 42 days.
“One of the biggest controversies concerning transfusion therapy is whether older blood is harmful compared to fresher blood,” said guideline author Aaron Tobian, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
“Now, we have information that can accurately inform guidelines about red blood cell storage duration. If data suggest no harm from the use of standard-issue blood and fresher blood would only constrain the use of a limited resource, continuing with standard practice of using older blood is appropriate. The newly released guidelines now clearly inform the community.”
The guidelines were published in JAMA alongside a related editorial.
The recommendations in the guidelines are based on an analysis of randomized clinical trials in which researchers evaluated hemoglobin thresholds for RBC transfusion (trials conducted from 1950 through May 2016) and RBC storage duration (trials conducted from 1948 through May 2016).
For transfusion thresholds, there were 31 trials including 12,587 subjects. The results of these trials suggested that restrictive transfusion thresholds (transfusing when the hemoglobin level is 7-8 g/dL) were not associated with higher rates of adverse clinical outcomes when compared to liberal thresholds (transfusing when the hemoglobin level is 9-10 g/dL).
For RBC storage duration, there were 13 trials including 5515 subjects. The results suggested that transfusing fresher blood did not improve clinical outcomes.
Transfusion threshold
The guideline authors said it is good practice, when making transfusion decisions, to consider the patient’s hemoglobin level, the overall clinical context, patient preference, and alternative therapies.
However, in general, a hemoglobin level of 7 g/dL should serve as the threshold for transfusing adult patients who are hemodynamically stable, even if they are in critical care. This is a strong recommendation based on moderate-quality evidence.
“While the recommended threshold of 7 g/dL is consistent with previous AABB guidelines, the strength of the new recommendation reflects the quality and quantity of the new data, much of which was generated since 2012,” said guideline author Jeffrey Carson, MD, of Robert Wood Johnson University Hospital in New Brunswick, New Jersey.
“Clinically, these results show that no harm will come from waiting to transfuse a patient until the hemoglobin level reaches a lower point. The restrictive approach is associated with reductions in blood use, blood conservation, and lower expenses.”
The guidelines also state that, for patients with pre-existing cardiovascular disease and those undergoing cardiac or orthopedic surgery, the threshold should be 8 g/dL. This is a strong recommendation based on moderate-quality evidence.
Neither of the aforementioned recommendations apply to patients with acute coronary syndrome, severe thrombocytopenia, or chronic transfusion-dependent anemia.
Dr Carson said additional trials are needed to determine whether these patients benefit from transfusion at higher hemoglobin levels.
“We are about to embark on a large, international clinical trial supported by the NIH [National Institutes of Health] that will provide the evidence needed to determine the best course of action for patients who have had a heart attack,” he said.
Dr Carson and his colleagues also noted that, although the recommendations are based on the available evidence, the hemoglobin transfusion thresholds assessed may not be optimal. And the use of hemoglobin transfusion thresholds may be an imperfect surrogate for oxygen delivery.
Storage duration
The guidelines state that most patients, including neonates, should receive standard-issue RBCs (stored for 42 days or less) rather than limiting patients to only fresh RBCs (stored for less than 10 days). This is a strong recommendation based on moderate-quality evidence.
The trials analyzed showed that patients who received standard-issue RBCs faced no higher risk of complications—including 30-day mortality, myocardial infarction, cerebrovascular accident, rebleeding, pneumonia, or thromboembolism—than those who received fresh RBCs.
However, the guideline authors said the trial results may not apply to RBCs nearing their expiration date (stored for 35 to 42 days), as only a small proportion of patients in these trials were exposed to such RBCs.
Furthermore, the trials did not include patients undergoing a massive or exchange transfusion, neonates and children with underlying renal disease at higher risk of hyperkalemia, patients undergoing intrauterine transfusions, or patients with hemoglobinopathies requiring chronic transfusion support.
So the optimal RBC storage duration for these patients is unknown.
![]()
Photo courtesy of UAB Hospital
AABB has released new guidelines on when to perform red blood cell (RBC) transfusions and the optimal duration of RBC storage.
The guidelines state that a restrictive transfusion threshold—waiting to transfuse until a patient’s hemoglobin level is 7-8 g/dL—is safe in most clinical settings.
And, for most patients, “fresh” RBCs—stored for less than 10 days—are no safer than standard-issue RBCs—stored for up to 42 days.
“One of the biggest controversies concerning transfusion therapy is whether older blood is harmful compared to fresher blood,” said guideline author Aaron Tobian, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
“Now, we have information that can accurately inform guidelines about red blood cell storage duration. If data suggest no harm from the use of standard-issue blood and fresher blood would only constrain the use of a limited resource, continuing with standard practice of using older blood is appropriate. The newly released guidelines now clearly inform the community.”
The guidelines were published in JAMA alongside a related editorial.
The recommendations in the guidelines are based on an analysis of randomized clinical trials in which researchers evaluated hemoglobin thresholds for RBC transfusion (trials conducted from 1950 through May 2016) and RBC storage duration (trials conducted from 1948 through May 2016).
For transfusion thresholds, there were 31 trials including 12,587 subjects. The results of these trials suggested that restrictive transfusion thresholds (transfusing when the hemoglobin level is 7-8 g/dL) were not associated with higher rates of adverse clinical outcomes when compared to liberal thresholds (transfusing when the hemoglobin level is 9-10 g/dL).
For RBC storage duration, there were 13 trials including 5515 subjects. The results suggested that transfusing fresher blood did not improve clinical outcomes.
Transfusion threshold
The guideline authors said it is good practice, when making transfusion decisions, to consider the patient’s hemoglobin level, the overall clinical context, patient preference, and alternative therapies.
However, in general, a hemoglobin level of 7 g/dL should serve as the threshold for transfusing adult patients who are hemodynamically stable, even if they are in critical care. This is a strong recommendation based on moderate-quality evidence.
“While the recommended threshold of 7 g/dL is consistent with previous AABB guidelines, the strength of the new recommendation reflects the quality and quantity of the new data, much of which was generated since 2012,” said guideline author Jeffrey Carson, MD, of Robert Wood Johnson University Hospital in New Brunswick, New Jersey.
“Clinically, these results show that no harm will come from waiting to transfuse a patient until the hemoglobin level reaches a lower point. The restrictive approach is associated with reductions in blood use, blood conservation, and lower expenses.”
The guidelines also state that, for patients with pre-existing cardiovascular disease and those undergoing cardiac or orthopedic surgery, the threshold should be 8 g/dL. This is a strong recommendation based on moderate-quality evidence.
Neither of the aforementioned recommendations apply to patients with acute coronary syndrome, severe thrombocytopenia, or chronic transfusion-dependent anemia.
Dr Carson said additional trials are needed to determine whether these patients benefit from transfusion at higher hemoglobin levels.
“We are about to embark on a large, international clinical trial supported by the NIH [National Institutes of Health] that will provide the evidence needed to determine the best course of action for patients who have had a heart attack,” he said.
Dr Carson and his colleagues also noted that, although the recommendations are based on the available evidence, the hemoglobin transfusion thresholds assessed may not be optimal. And the use of hemoglobin transfusion thresholds may be an imperfect surrogate for oxygen delivery.
Storage duration
The guidelines state that most patients, including neonates, should receive standard-issue RBCs (stored for 42 days or less) rather than limiting patients to only fresh RBCs (stored for less than 10 days). This is a strong recommendation based on moderate-quality evidence.
The trials analyzed showed that patients who received standard-issue RBCs faced no higher risk of complications—including 30-day mortality, myocardial infarction, cerebrovascular accident, rebleeding, pneumonia, or thromboembolism—than those who received fresh RBCs.
However, the guideline authors said the trial results may not apply to RBCs nearing their expiration date (stored for 35 to 42 days), as only a small proportion of patients in these trials were exposed to such RBCs.
Furthermore, the trials did not include patients undergoing a massive or exchange transfusion, neonates and children with underlying renal disease at higher risk of hyperkalemia, patients undergoing intrauterine transfusions, or patients with hemoglobinopathies requiring chronic transfusion support.
So the optimal RBC storage duration for these patients is unknown.
Cord blood product granted breakthrough designation

Photo courtesy of NHS
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for NiCord®, a product in development as a graft modality for patients undergoing hematopoietic stem cell transplant to treat high-risk hematologic malignancies.
NiCord consists of cells from a single unit of umbilical cord blood cultured in nicotinamide (a vitamin B derivative) and cytokines that are typically used for expansion (thrombopoietin, interleukin 6, FLT3 ligand, and stem cell factor).
Data from the pilot and phase 1/2 studies of NiCord have suggested the therapy can provide a clinically meaningful improvement in time to neutrophil engraftment over traditional cord blood transplant.
Additional research presented at EBMT 2016 showed that patients who received NiCord had fewer infections, shorter hospital stays, quicker platelet engraftment, and improved non-relapse mortality when compared to patients who received a traditional cord blood transplant.
The phase 3 registration study of NiCord is scheduled to begin before the end of this year.
In addition to breakthrough designation, NiCord also has orphan designation from the FDA as a treatment for patients with acute lymphoblastic leukemia, acute myeloid leukemia, Hodgkin lymphoma, or myelodysplastic syndromes.
NiCord is being developed by Gamida Cell.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
Breakthrough designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as a rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Photo courtesy of NHS
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for NiCord®, a product in development as a graft modality for patients undergoing hematopoietic stem cell transplant to treat high-risk hematologic malignancies.
NiCord consists of cells from a single unit of umbilical cord blood cultured in nicotinamide (a vitamin B derivative) and cytokines that are typically used for expansion (thrombopoietin, interleukin 6, FLT3 ligand, and stem cell factor).
Data from the pilot and phase 1/2 studies of NiCord have suggested the therapy can provide a clinically meaningful improvement in time to neutrophil engraftment over traditional cord blood transplant.
Additional research presented at EBMT 2016 showed that patients who received NiCord had fewer infections, shorter hospital stays, quicker platelet engraftment, and improved non-relapse mortality when compared to patients who received a traditional cord blood transplant.
The phase 3 registration study of NiCord is scheduled to begin before the end of this year.
In addition to breakthrough designation, NiCord also has orphan designation from the FDA as a treatment for patients with acute lymphoblastic leukemia, acute myeloid leukemia, Hodgkin lymphoma, or myelodysplastic syndromes.
NiCord is being developed by Gamida Cell.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
Breakthrough designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as a rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Photo courtesy of NHS
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for NiCord®, a product in development as a graft modality for patients undergoing hematopoietic stem cell transplant to treat high-risk hematologic malignancies.
NiCord consists of cells from a single unit of umbilical cord blood cultured in nicotinamide (a vitamin B derivative) and cytokines that are typically used for expansion (thrombopoietin, interleukin 6, FLT3 ligand, and stem cell factor).
Data from the pilot and phase 1/2 studies of NiCord have suggested the therapy can provide a clinically meaningful improvement in time to neutrophil engraftment over traditional cord blood transplant.
Additional research presented at EBMT 2016 showed that patients who received NiCord had fewer infections, shorter hospital stays, quicker platelet engraftment, and improved non-relapse mortality when compared to patients who received a traditional cord blood transplant.
The phase 3 registration study of NiCord is scheduled to begin before the end of this year.
In addition to breakthrough designation, NiCord also has orphan designation from the FDA as a treatment for patients with acute lymphoblastic leukemia, acute myeloid leukemia, Hodgkin lymphoma, or myelodysplastic syndromes.
NiCord is being developed by Gamida Cell.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new therapies for serious or life-threatening conditions.
Breakthrough designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as a rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Bovine heparin may be comparable to porcine heparin

A new study suggests that heparin derived from cattle may be as effective as heparin derived from pigs, but more research is needed.
Investigators found differences in the structural and molecular characteristics of bovine and porcine heparins, but these differences did not appear to have a significant effect on the drugs’ anticoagulant properties in vitro.
Still, the researchers said it is not clear if these differences affect the drugs’ activity in humans.
Jawed Fareed, PhD, of Loyola University Chicago Stritch School of Medicine in Illinois, and his colleagues conducted this research and reported the results in Clinical and Applied Thrombosis/Hemostasis.
Heparin used in the US now comes from the intestines of pigs that are slaughtered for meat. Seventy-five percent of the heparin used in the US comes from China, which is the world’s largest pork producer.
As heparin is a widely used drug that, in certain cases, has no medical alternatives, the US healthcare system could be vulnerable to fluctuations in the crude heparin supply, according to the US Food and Drug Administration’s Center for Drug Evaluation and Research.
Therefore, the center is evaluating reintroducing bovine heparin to the market in order to avoid shortages, particularly in case the porcine heparin supply is contaminated, as occurred in 2008.
Bovine heparin was voluntarily withdrawn from the market during the 1980s due to worries that it could, in rare cases, cause thrombocytopenia or be contaminated with bovine spongiform encephalopathy (mad cow disease).
According to Dr Fareed, those fears have been put to rest by advancements in manufacturing and quality control that have resulted in purer forms of heparin. Still, some experts remain skeptical about bovine heparin.
With this in mind, Dr Fareed and his colleagues compared individually manufactured batches of bovine heparin (historical samples from a variety of manufacturers) with individually manufactured batches of porcine heparin (current samples from 2 different manufacturers).
The investigators studied heparins isolated from pig intestines (PI), bovine lungs (BL), and bovine intestines (BI).
They found the BL, BI, and PI heparins all produced a concentration-dependent anticoagulant effect. And there was no significant difference in the anti-Xa and anti-IIa potencies of the BL, BI, and PI heparins.
The researchers noted that there were significant structural differences between PI and BI heparins, and it isn’t clear whether these differences would have an impact in patients.
Likewise, although the BL heparin samples were “highly similar” to the PI heparin samples, the BL heparins had a lower molecular weight. And the investigators said it was unclear if this would adversely affect the BL heparins’ pharmacology.
Furthermore, the researchers noted that there was greater variability among the BL heparins than the PI heparins. However, they said this could be due to the multiple historic manufacturers of BL heparins.
The investigators concluded that more research is needed to examine these possibilities.
A new study suggests that heparin derived from cattle may be as effective as heparin derived from pigs, but more research is needed.
Investigators found differences in the structural and molecular characteristics of bovine and porcine heparins, but these differences did not appear to have a significant effect on the drugs’ anticoagulant properties in vitro.
Still, the researchers said it is not clear if these differences affect the drugs’ activity in humans.
Jawed Fareed, PhD, of Loyola University Chicago Stritch School of Medicine in Illinois, and his colleagues conducted this research and reported the results in Clinical and Applied Thrombosis/Hemostasis.
Heparin used in the US now comes from the intestines of pigs that are slaughtered for meat. Seventy-five percent of the heparin used in the US comes from China, which is the world’s largest pork producer.
As heparin is a widely used drug that, in certain cases, has no medical alternatives, the US healthcare system could be vulnerable to fluctuations in the crude heparin supply, according to the US Food and Drug Administration’s Center for Drug Evaluation and Research.
Therefore, the center is evaluating reintroducing bovine heparin to the market in order to avoid shortages, particularly in case the porcine heparin supply is contaminated, as occurred in 2008.
Bovine heparin was voluntarily withdrawn from the market during the 1980s due to worries that it could, in rare cases, cause thrombocytopenia or be contaminated with bovine spongiform encephalopathy (mad cow disease).
According to Dr Fareed, those fears have been put to rest by advancements in manufacturing and quality control that have resulted in purer forms of heparin. Still, some experts remain skeptical about bovine heparin.
With this in mind, Dr Fareed and his colleagues compared individually manufactured batches of bovine heparin (historical samples from a variety of manufacturers) with individually manufactured batches of porcine heparin (current samples from 2 different manufacturers).
The investigators studied heparins isolated from pig intestines (PI), bovine lungs (BL), and bovine intestines (BI).
They found the BL, BI, and PI heparins all produced a concentration-dependent anticoagulant effect. And there was no significant difference in the anti-Xa and anti-IIa potencies of the BL, BI, and PI heparins.
The researchers noted that there were significant structural differences between PI and BI heparins, and it isn’t clear whether these differences would have an impact in patients.
Likewise, although the BL heparin samples were “highly similar” to the PI heparin samples, the BL heparins had a lower molecular weight. And the investigators said it was unclear if this would adversely affect the BL heparins’ pharmacology.
Furthermore, the researchers noted that there was greater variability among the BL heparins than the PI heparins. However, they said this could be due to the multiple historic manufacturers of BL heparins.
The investigators concluded that more research is needed to examine these possibilities.
A new study suggests that heparin derived from cattle may be as effective as heparin derived from pigs, but more research is needed.
Investigators found differences in the structural and molecular characteristics of bovine and porcine heparins, but these differences did not appear to have a significant effect on the drugs’ anticoagulant properties in vitro.
Still, the researchers said it is not clear if these differences affect the drugs’ activity in humans.
Jawed Fareed, PhD, of Loyola University Chicago Stritch School of Medicine in Illinois, and his colleagues conducted this research and reported the results in Clinical and Applied Thrombosis/Hemostasis.
Heparin used in the US now comes from the intestines of pigs that are slaughtered for meat. Seventy-five percent of the heparin used in the US comes from China, which is the world’s largest pork producer.
As heparin is a widely used drug that, in certain cases, has no medical alternatives, the US healthcare system could be vulnerable to fluctuations in the crude heparin supply, according to the US Food and Drug Administration’s Center for Drug Evaluation and Research.
Therefore, the center is evaluating reintroducing bovine heparin to the market in order to avoid shortages, particularly in case the porcine heparin supply is contaminated, as occurred in 2008.
Bovine heparin was voluntarily withdrawn from the market during the 1980s due to worries that it could, in rare cases, cause thrombocytopenia or be contaminated with bovine spongiform encephalopathy (mad cow disease).
According to Dr Fareed, those fears have been put to rest by advancements in manufacturing and quality control that have resulted in purer forms of heparin. Still, some experts remain skeptical about bovine heparin.
With this in mind, Dr Fareed and his colleagues compared individually manufactured batches of bovine heparin (historical samples from a variety of manufacturers) with individually manufactured batches of porcine heparin (current samples from 2 different manufacturers).
The investigators studied heparins isolated from pig intestines (PI), bovine lungs (BL), and bovine intestines (BI).
They found the BL, BI, and PI heparins all produced a concentration-dependent anticoagulant effect. And there was no significant difference in the anti-Xa and anti-IIa potencies of the BL, BI, and PI heparins.
The researchers noted that there were significant structural differences between PI and BI heparins, and it isn’t clear whether these differences would have an impact in patients.
Likewise, although the BL heparin samples were “highly similar” to the PI heparin samples, the BL heparins had a lower molecular weight. And the investigators said it was unclear if this would adversely affect the BL heparins’ pharmacology.
Furthermore, the researchers noted that there was greater variability among the BL heparins than the PI heparins. However, they said this could be due to the multiple historic manufacturers of BL heparins.
The investigators concluded that more research is needed to examine these possibilities.