User login
Over the past decade, physician-pharmacist collaborative practices have gained traction in primary care as a way to implement team-based-care models. And there is evidence pointing to the effectiveness of this multidisciplinary heath care team approach, in which pharmacists are typically responsible for such things as obtaining medication histories, identifying barriers to adherence, and adjusting medication regimens.
Several studies have shown the significant impact that physician-pharmacist collaborative management (PPCM) can have on blood pressure (BP) control among patients with hypertension (HTN).1-8 Additionally, PPCM may have positive effects on HbA1c reduction and diabetes control,9-11 suggesting that benefits may extend to other chronic diseases, too.
In the review that follows, we’ll detail the impact that PPCM can have on patient care, health-care utilization, and cost effectiveness. (For a look at PPCM “in action,” see the sidebar below.) We’ll also review the challenges of implementing this model that, at present, is mostly found in academically-affiliated clinics and large health systems.
SIDEBAR
The physician-pharmacist collaborative care model in actionFor patients with chronic diseases such as hypertension and diabetes, pharmacists can be invaluable members of multidisciplinary health care teams by providing direct consultation to optimize pharmacotherapy. Although their particular role and responsibilities can vary widely from one primary care setting to the next, the following describes the general workflow of a physician-pharmacist collaborative care model in action.
The patient, 60-year-old Isabel B, arrives for an appointment for pharmacotherapy management of her hypertension. After checking in, a registered nurse (RN), medical assistant (MA), or the pharmacist obtains her vital signs, height, and weight prior to rooming. Additionally, any necessary point-of-care lab tests are obtained at this time.
Once the patient is roomed, the pharmacist collects a thorough medication history from Ms. B, verifying and updating her current medication list, confirming the dose and frequency of each medication, and gathering information regarding adverse effects and barriers to adherence. The pharmacist may also review current laboratory results and vital signs to assess the appropriateness and therapeutic efficacy of the current drug therapy regimen.
Depending upon the collaborative practice plan in place, one of the following steps may occur:
A. The pharmacist makes a change to Ms. B's medication regimen and orders any necessary laboratory tests for monitoring. A progress note is forwarded to Ms. B's primary care provider (PCP) to inform him/her of the changes made to the regimen and the follow-up interval.
B. The pharmacist presents pharmacotherapy recommendations to the attending physician or Ms. B's PCP. The therapeutic and monitoring plans are discussed and approved as a team at the time of Ms. B's visit.
C. The pharmacist sends a message to Ms. B's PCP regarding information discovered during the interview and provides recommendations for a treatment plan based on the visit. The PCP reviews the recommendations, and can either 1) send approval to the pharmacist through a message or 2) implement the appropriate drug therapy changes at Ms. B's next visit.
In Cases A and B, the pharmacist then reviews the final pharmacotherapy plan with Ms. B, discusses the medication and monitoring parameters, answers any questions related to the new treatment regimen, and schedules a follow-up visit. In Case C, the pharmacist may still provide medication counseling and answer questions related to drug therapy during the visit; however, review of the final pharmacotherapy plan may be done over the telephone after approval by the PCP. Alternatively, a follow-up appointment with Ms. B's PCP can be scheduled shortly after the visit with the pharmacist to discuss any recommended drug therapy changes.
PPCM impacts chronic diseases
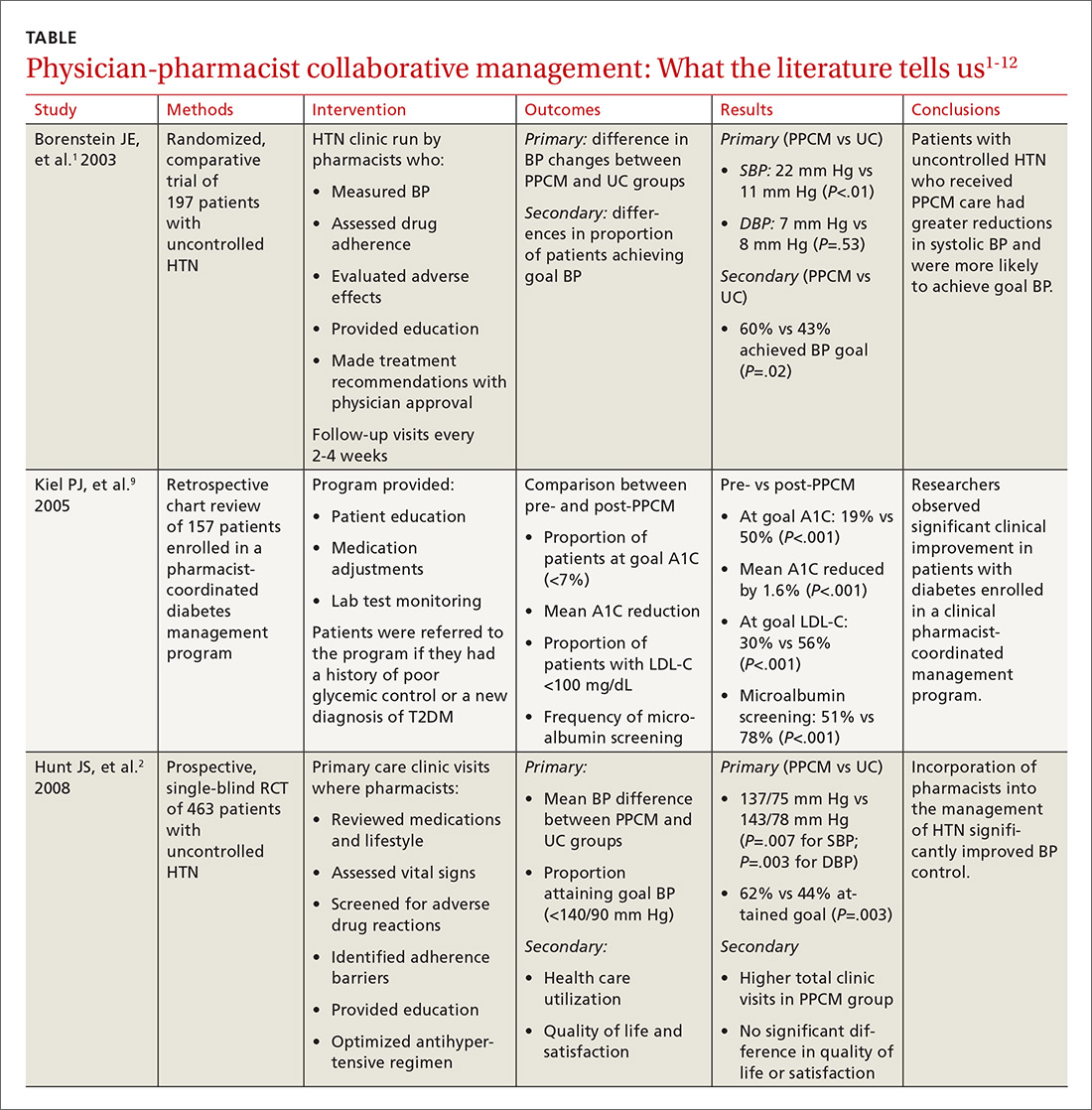
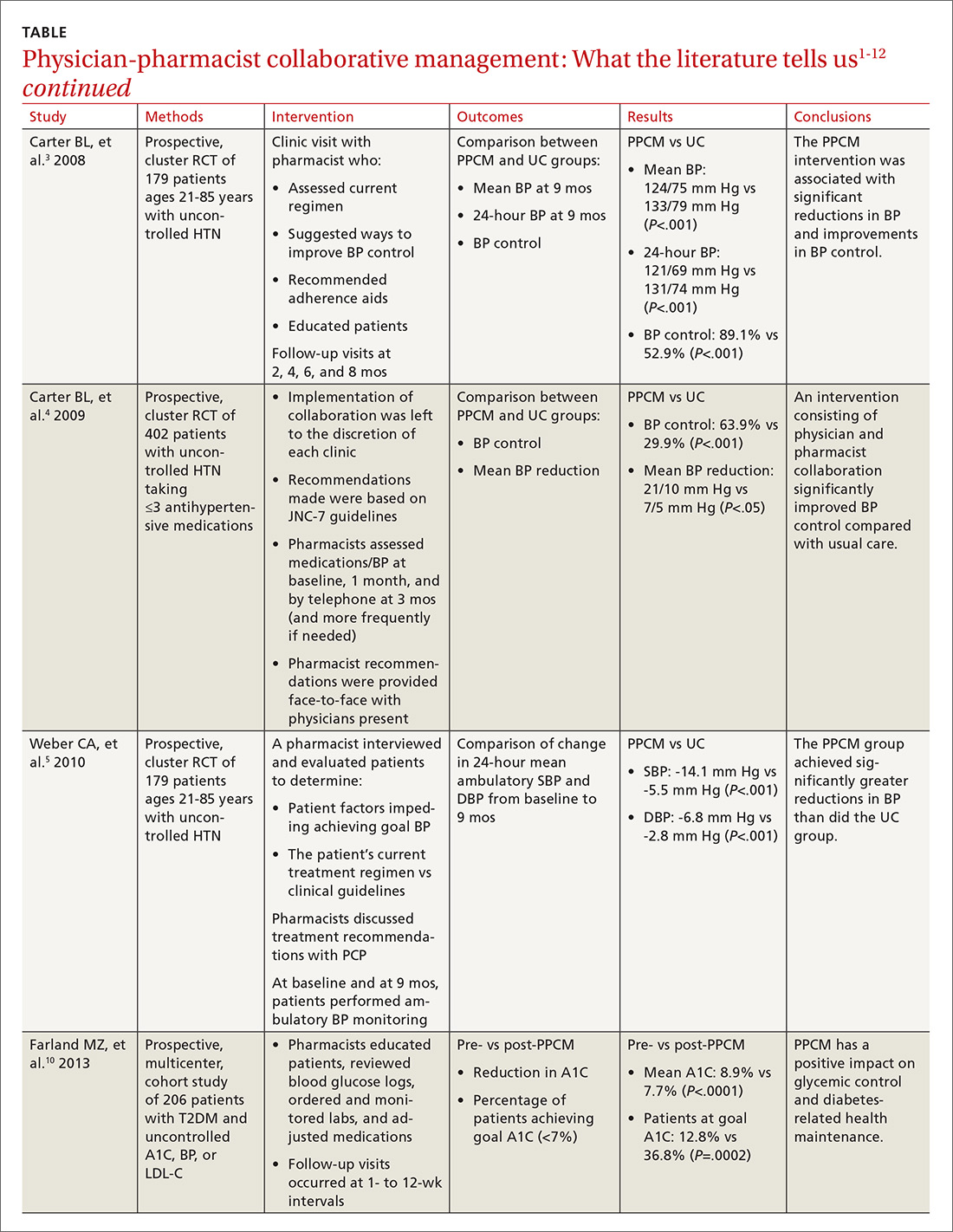
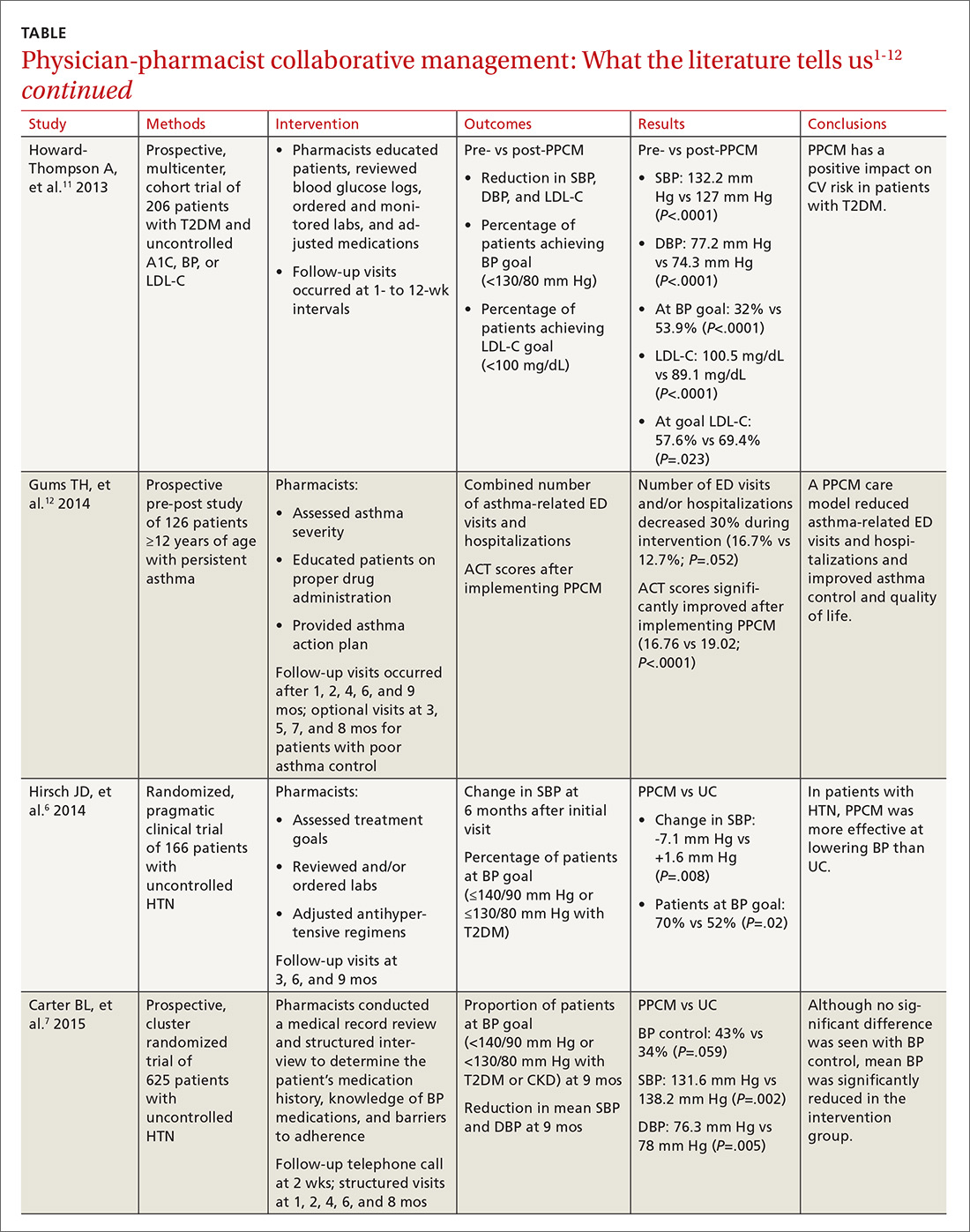
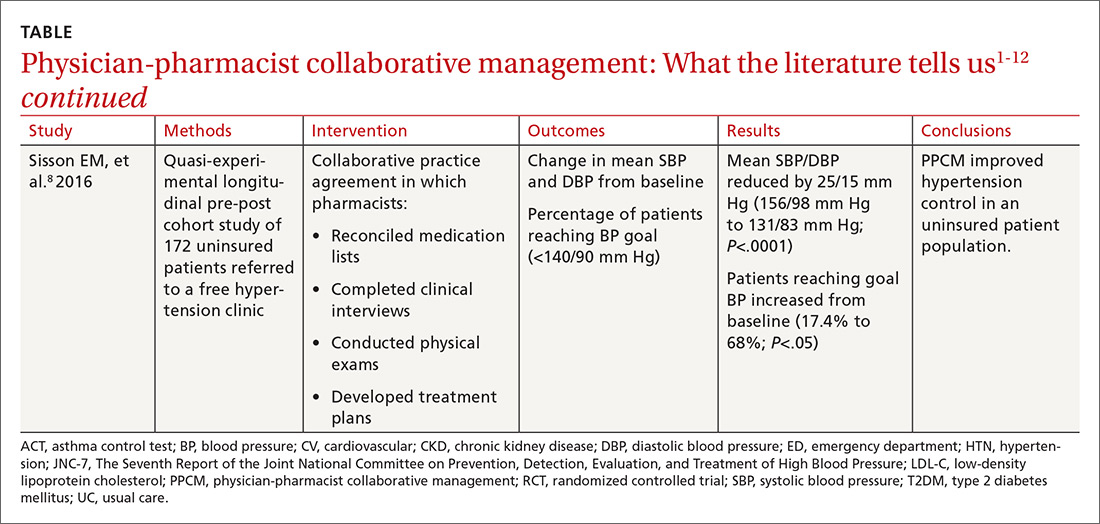
The current literature is rife with studies investigating the impact of PPCM on chronic diseases in the primary care setting.1-12 Although no specific guidelines on implementing PPCM exist, these studies utilized similar interventions that provided pharmacists with the ability to manage medication therapy under the supervision of a physician. A number of these studies incorporated collaborative practice plans to delineate the specific duties performed by physicians and pharmacists.2,6,8,10,11 Responsibilities for pharmacists often included assessing vital signs, reviewing laboratory parameters and ordering appropriate tests, providing patient education, screening for drug interactions, identifying barriers to medication adherence, and adjusting medication regimens. The TABLE1-12 provides a summary of studies investigating the impact of PPCM in the primary care setting.
PPCM leads to greater BP reductions, improved BP control
The majority of research surrounding PPCM has focused on uncontrolled HTN.1-8 Patients in many of these studies saw a pharmacist in a specialized HTN clinic, where the multidisciplinary staff performed a thorough evaluation of the patient’s current hypertensive management. The pharmacists in these PPCM programs closely monitored patients and made adjustments to antihypertensive regimens as necessary. Systolic and diastolic BP reductions in the intervention groups ranged from 14 to 36 mm Hg and 7 to 15 mm Hg, respectively.1-5,7,8 The percentage of patients with BP control at the end of the studies ranged from 43% to 89%.1,3,4,6,7
In a prospective, cluster-randomized trial performed at 32 primary care offices in 15 states, researchers assigned 625 patients with uncontrolled HTN to receive physician-pharmacist collaborative care or usual care with primary care provider management.7 As part of the PPCM intervention, clinical pharmacists conducted a thorough medical record review and a structured interview of the patients. During the interview, the clinical pharmacists reviewed the patient’s medication history, assessed the patient’s knowledge of BP medications, and addressed any barriers to adherence. In collaboration with the physician, the pharmacists developed a care plan with recommendations for optimizing the drug regimen. After the baseline visit, the pharmacists conducted structured face-to-face interviews with patients at 1, 2, 4, 6, and 8 months, with additional visits scheduled if BP was still uncontrolled.
At 9 months, patients in the PPCM group had significantly greater reductions in BP than those in the control group, and BP control was achieved in 43% of the PPCM group vs 34% of the control group. This study corroborates results from previous (similar) studies investigating the impact of PPCM on patients with uncontrolled HTN.1-6
PPCM helps patients reduce their HbA1c levels
Researchers have also studied the impact of PPCM strategies on the management of diabetes mellitus.9-11 In one retrospective study of 157 patients, implementation of a pharmacy-coordinated diabetes (any type) management program significantly improved HbA1c and increased the percentage of patients reaching their HbA1c goal.9 Furthermore, researchers observed improvements in low-density lipoprotein cholesterol (LDL-C) levels and an increased number of patients obtaining a microalbumin screening after initiation of the program.
A more recent prospective, multicenter cohort study of 206 patients with uncontrolled type 2 diabetes had similar results.10 In collaboration with the primary care physician (PCP), clinical pharmacists provided medication therapy management through adjustment of antihyperglycemic, antihypertensive, or lipid-lowering medications. Additional interventions provided by the pharmacists included reviewing blood glucose logs, ordering and monitoring laboratory tests, performing sensory foot examinations, and providing patient education.
Implementation of PPCM reduced the average HbA1c by 1.2% and increased the percentage of patients achieving an HbA1c <7% by about 24%. The researchers also observed improvements in BP and LDL-C levels in this patient population.11
Asthma and beyond
Future studies may well show that the benefits of PPCM extend to the management of other chronic diseases. One prospective, pre-post study of 126 patients with asthma found that the number of emergency department (ED) visits and/or hospitalizations decreased 30% during 9 months with a PPCM intervention and then returned to levels similar to baseline once the intervention ceased.12 Other potential disease areas that have been studied, or are being studied, include chronic obstructive pulmonary disease, chronic kidney disease, dyslipidemia, and congestive heart failure.13
Benefits derive from altered health care utilization
Researchers attribute much of the benefit observed with PPCM to the increased—albeit different—health-care utilization among the patients in the intervention groups. In general, patients participating in PPCM have an increased total number of visits, but more of those visits are with pharmacists and fewer are with physicians; they also are prescribed more medications, but don’t necessarily take more pills per day.1,2,5 In the end, patients have been found to achieve significantly better disease control without compromising quality of life or satisfaction.2
Some studies have found that continued pharmacist involvement may be necessary to sustain the benefits achieved.6 However, other studies have suggested that the benefits are maintained even after discontinuation of the pharmacist intervention.14,15 Thus, further research is necessary to determine which patients may benefit most from ongoing involvement with a pharmacist.
How cost-effective is the PPCM model?
Implementing a PPCM model in a primary care setting often hinges upon whether the intervention will be cost-effective. Several studies have reported the cost-effectiveness of clinical pharmacists in the management of HTN.1,16,17
Borenstein and colleagues found significantly lower provider visit costs per patient in the PPCM group ($160) compared with the usual care group ($195), a difference that the authors attributed to a decreased number of visits to PCPs and an increased number of lower cost visits with pharmacists in the PPCM group.1 However, the difference could have been affected by the arbitrary measurement of physician-pharmacist collaboration time in the study.
Overcoming implementation challenges
Implementation of pharmacist collaboration within primary care medicine may pose a challenge, as the requirements and resources vary widely among primary care settings. Health-system administrators, for example, may need to reorganize the clinic structure and budget resources in order to overcome some of the obstacles to implementing a PPCM model.
Experts have reported several strategies that help in establishing PPCM within primary care clinics,18 including proactively identifying patients who may benefit from pharmacist intervention, requiring appropriate training and credentialing of pharmacists, and establishing a set schedule for pharmacists to interview patients. Clinics would also be well served to model interventions outlined in the studies mentioned in this article and provide adequate time for pharmacists to perform structured activities, including review of medication history, assessment of current disease state control, and adjustment of medication therapy regimens. And, of course, given the diversity of primary care settings, administrators will need to identify the specific PPCM strategies that best complement their respective collaborative practice plans and environments.
The lack of well-defined reimbursement models for pharmacy services has presented a challenge for generating revenue and effectively implementing PPCM within many primary care settings. Currently, the Centers for Medicare and Medicaid Services and third-party payers do not recognize pharmacists as independent providers, creating a barrier for obtaining reimbursement for clinical pharmacy services. Typically, pharmacists have charged for clinic visits under a consultant physician through the “incident to” billing model, with the option to bill at higher levels if the patient was seen jointly with the physician.
Can this model benefit the underserved?
A prospective, cluster-randomized clinic study has shown pharmacist intervention to reduce racial and socioeconomic disparities in the treatment of elevated BP.19 This study is the first to show that a team-care model can overcome inequalities arising from low income, low patient education status, and little or no insurance to produce the same health care benefit as in those with higher socioeconomic and educational status. This type of collaborative care model may be particularly beneficial when incorporated within a PCMH catering to underserved populations.20
However, sparse data currently exist regarding the benefits of the PPCM model within a PCMH, despite the fact that integration of this type of collaborative model is expected to contribute positively to patient care.21
Physician acceptance of pharmacist involvement is mixed
While physician acceptance of pharmacist recommendations is generally high, at least one study indicated that some health-care professionals in patient-care teams are reluctant to incorporate pharmacists into a PCMH. Reasons include difficulty in coordination of care with pharmacy services and limited knowledge by other professionals of pharmacists’ training.22
Centralization can combat a lack of resources
As noted earlier, primary care offices that implement PPCM models are mostly academically affiliated or are part of large health systems. Many private primary care offices lack the resources to employ a pharmacist in their office. As an alternative, prospective clinical trials are looking at a centralized, Web-based cardiovascular risk service managed by pharmacists.23,24 This service’s primary objective is to improve adherence to metric-based outcomes developed as part of The Guideline Advantage quality improvement program put forth by the American Cancer Society, American Diabetes Association, and the American Heart and Stroke Associations. (See http://www.guidelineadvantage.org/TGA/ for more information.)
Researchers hope to prove that a centralized, pharmacist-run, clinical service can meet metric-driven outcomes that many primary care offices are now being required to meet in order to receive compensation from insurance companies. One of these studies is specifically looking at rural private offices that lack many of the resources that many large academic offices possess.23 The study is ongoing and results are expected sometime in 2018.
CORRESPONDENCE
John G. Gums, PharmD, College of Pharmacy, University of Florida, 1225 Center Drive, HPNP 4332, Gainesville, FL 32601; [email protected].
1. Borenstein JE, Graber G, Saltiel E, et al. Physician-pharmacist comanagement of hypertension: a randomized, comparative trial. Pharmacotherapy. 2003;23:209-216.
2. Hunt JS, Siemienczuk J, Pape G, et al. A randomized controlled trial of team-based care: impact of physician-pharmacist collaboration on uncontrolled hypertension. J Gen Intern Med. 2008;23:1966-1972.
3. Carter BL, Bergus GR, Dawson JD, et al. A cluster randomized trial to evaluate physician/pharmacist collaboration to improve blood pressure control. J Clin Hypertens (Greenwich). 2008;10:260-271.
4. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. 2009;169:1996-2002.
5. Weber CA, Ernst ME, Sezate GS, et al. Pharmacist-physician comanagement of hypertension and reduction in 24-hour ambulatory blood pressures. Arch Intern Med. 2010;170:1634-1639.
6. Hirsch JD, Steers N, Adler DS, et al. Primary care-based, pharmacist-physician collaborative medication-therapy management of hypertension: a randomized, pragmatic trial. Clin Ther. 2014;36:1244-1254.
7. Carter BL, Coffey CS, Ardery G, et al. Cluster-randomized trial of a physician/pharmacist collaborative model to improve blood pressure control. Circ Cardiovasc Qual Outcomes. 2015;8:235-243.
8. Sisson EM, Dixon DL, Kildow DC, et al. Effectiveness of a pharmacist-physician team-based collaboration to improve long-term blood pressure control at an inner-city safety-net clinic. Pharmacotherapy. 2016;36:342-347.
9. Kiel PJ, McCord AD. Pharmacist impact on clinical outcomes in a diabetes disease management program via collaborative practice. Ann Pharmacother. 2005;39:1828-1832.
10. Farland MZ, Byrd DC, McFarland MS, et al. Pharmacist-physician collaboration for diabetes care: the diabetes initiative program. Ann Pharmacother. 2013;47:781-789.
11. Howard-Thompson A, Farland MZ, Byrd DC, et al. Pharmacist-physician collaboration for diabetes care: cardiovascular outcomes. Ann Pharmacother. 2013;47:1471-1477.
12. Gums TH, Carter BL, Milavetz G, et al. Physician-pharmacist collaborative management of asthma in primary care. Pharmacotherapy. 2014;34:1033-1042.
13. Greer N, Bolduc J, Geurkink E, et al. VA Evidence-based Synthesis Program Reports. Pharmacist-Led Chronic Disease Management: A Systematic Review of Effectiveness and Harms Compared to Usual Care. Washington (DC): Department of Veterans Affairs (US); 2015.
14. Wentzlaff DM, Carter BL, Ardery G, et al. Sustained blood pressure control following discontinuation of a pharmacist intervention. J Clin Hypertens (Greenwich). 2011;13:431-437.
15. Carter BL, Vander Weg MW, Parker CP, et al. Sustained blood pressure control following discontinuation of a pharmacist intervention for veterans. J Clin Hypertens (Greenwich). 2015;17:701-708.
16. Kulchaitanaroaj P, Brooks JM, Ardery G, et al. Incremental costs associated with physician and pharmacist collaboration to improve blood pressure control. Pharmacotherapy. 2012;32:772-780.
17. Polgreen LA, Han J, Carter BL, et al. Cost effectiveness of a physician-pharmacist collaboration intervention to improve blood pressure control. Hypertension. 2015;66:1145-1151.
18. Carter BL. Primary care physician-pharmacist collaborative care model: strategies for implementation. Pharmacotherapy. 2016;36:363-373.
19. Anderegg MD, Gums TH, Uribe L, et al. Physician-pharmacist collaborative management: narrowing the socioeconomic blood pressure gap. Hypertension. 2016;68:1314-1320.
20. Moczygemba LR, Goode JV, Gatewood SBS, et al. Integration of collaborative medication therapy management in a safety net patient-centered medical home. J Am Pharm Assoc (2003). 2011;51:167-172.
21. Scott MA, Hitch B, Ray L, et al. Integration of pharmacists into a patient-centered medical home. J Am Pharm Assoc (2003). 2011;51:161-166.
22. Patterson BJ, Solimeo SL, Stewart KR, et al. Perceptions of pharmacists’ integration into patient-centered medical home teams. Res Social Adm Pharm. 2015;11:85-95.
23. Carter BL, Levy BT, Gryzlak B, et al. A centralized cardiovascular risk service to improve guideline adherence in private primary care offices. Contemp Clin Trials. 2015;43:25-32.
24. Carter BL, Coffey CS, Chrischilles EA, et al. A cluster-randomized trial of a centralized clinical pharmacy cardiovascular risk service to improve guideline adherence. Pharmacotherapy. 2015;35:653-662.
Over the past decade, physician-pharmacist collaborative practices have gained traction in primary care as a way to implement team-based-care models. And there is evidence pointing to the effectiveness of this multidisciplinary heath care team approach, in which pharmacists are typically responsible for such things as obtaining medication histories, identifying barriers to adherence, and adjusting medication regimens.
Several studies have shown the significant impact that physician-pharmacist collaborative management (PPCM) can have on blood pressure (BP) control among patients with hypertension (HTN).1-8 Additionally, PPCM may have positive effects on HbA1c reduction and diabetes control,9-11 suggesting that benefits may extend to other chronic diseases, too.
In the review that follows, we’ll detail the impact that PPCM can have on patient care, health-care utilization, and cost effectiveness. (For a look at PPCM “in action,” see the sidebar below.) We’ll also review the challenges of implementing this model that, at present, is mostly found in academically-affiliated clinics and large health systems.
SIDEBAR
The physician-pharmacist collaborative care model in actionFor patients with chronic diseases such as hypertension and diabetes, pharmacists can be invaluable members of multidisciplinary health care teams by providing direct consultation to optimize pharmacotherapy. Although their particular role and responsibilities can vary widely from one primary care setting to the next, the following describes the general workflow of a physician-pharmacist collaborative care model in action.
The patient, 60-year-old Isabel B, arrives for an appointment for pharmacotherapy management of her hypertension. After checking in, a registered nurse (RN), medical assistant (MA), or the pharmacist obtains her vital signs, height, and weight prior to rooming. Additionally, any necessary point-of-care lab tests are obtained at this time.
Once the patient is roomed, the pharmacist collects a thorough medication history from Ms. B, verifying and updating her current medication list, confirming the dose and frequency of each medication, and gathering information regarding adverse effects and barriers to adherence. The pharmacist may also review current laboratory results and vital signs to assess the appropriateness and therapeutic efficacy of the current drug therapy regimen.
Depending upon the collaborative practice plan in place, one of the following steps may occur:
A. The pharmacist makes a change to Ms. B's medication regimen and orders any necessary laboratory tests for monitoring. A progress note is forwarded to Ms. B's primary care provider (PCP) to inform him/her of the changes made to the regimen and the follow-up interval.
B. The pharmacist presents pharmacotherapy recommendations to the attending physician or Ms. B's PCP. The therapeutic and monitoring plans are discussed and approved as a team at the time of Ms. B's visit.
C. The pharmacist sends a message to Ms. B's PCP regarding information discovered during the interview and provides recommendations for a treatment plan based on the visit. The PCP reviews the recommendations, and can either 1) send approval to the pharmacist through a message or 2) implement the appropriate drug therapy changes at Ms. B's next visit.
In Cases A and B, the pharmacist then reviews the final pharmacotherapy plan with Ms. B, discusses the medication and monitoring parameters, answers any questions related to the new treatment regimen, and schedules a follow-up visit. In Case C, the pharmacist may still provide medication counseling and answer questions related to drug therapy during the visit; however, review of the final pharmacotherapy plan may be done over the telephone after approval by the PCP. Alternatively, a follow-up appointment with Ms. B's PCP can be scheduled shortly after the visit with the pharmacist to discuss any recommended drug therapy changes.
PPCM impacts chronic diseases
The current literature is rife with studies investigating the impact of PPCM on chronic diseases in the primary care setting.1-12 Although no specific guidelines on implementing PPCM exist, these studies utilized similar interventions that provided pharmacists with the ability to manage medication therapy under the supervision of a physician. A number of these studies incorporated collaborative practice plans to delineate the specific duties performed by physicians and pharmacists.2,6,8,10,11 Responsibilities for pharmacists often included assessing vital signs, reviewing laboratory parameters and ordering appropriate tests, providing patient education, screening for drug interactions, identifying barriers to medication adherence, and adjusting medication regimens. The TABLE1-12 provides a summary of studies investigating the impact of PPCM in the primary care setting.
PPCM leads to greater BP reductions, improved BP control
The majority of research surrounding PPCM has focused on uncontrolled HTN.1-8 Patients in many of these studies saw a pharmacist in a specialized HTN clinic, where the multidisciplinary staff performed a thorough evaluation of the patient’s current hypertensive management. The pharmacists in these PPCM programs closely monitored patients and made adjustments to antihypertensive regimens as necessary. Systolic and diastolic BP reductions in the intervention groups ranged from 14 to 36 mm Hg and 7 to 15 mm Hg, respectively.1-5,7,8 The percentage of patients with BP control at the end of the studies ranged from 43% to 89%.1,3,4,6,7
In a prospective, cluster-randomized trial performed at 32 primary care offices in 15 states, researchers assigned 625 patients with uncontrolled HTN to receive physician-pharmacist collaborative care or usual care with primary care provider management.7 As part of the PPCM intervention, clinical pharmacists conducted a thorough medical record review and a structured interview of the patients. During the interview, the clinical pharmacists reviewed the patient’s medication history, assessed the patient’s knowledge of BP medications, and addressed any barriers to adherence. In collaboration with the physician, the pharmacists developed a care plan with recommendations for optimizing the drug regimen. After the baseline visit, the pharmacists conducted structured face-to-face interviews with patients at 1, 2, 4, 6, and 8 months, with additional visits scheduled if BP was still uncontrolled.
At 9 months, patients in the PPCM group had significantly greater reductions in BP than those in the control group, and BP control was achieved in 43% of the PPCM group vs 34% of the control group. This study corroborates results from previous (similar) studies investigating the impact of PPCM on patients with uncontrolled HTN.1-6
PPCM helps patients reduce their HbA1c levels
Researchers have also studied the impact of PPCM strategies on the management of diabetes mellitus.9-11 In one retrospective study of 157 patients, implementation of a pharmacy-coordinated diabetes (any type) management program significantly improved HbA1c and increased the percentage of patients reaching their HbA1c goal.9 Furthermore, researchers observed improvements in low-density lipoprotein cholesterol (LDL-C) levels and an increased number of patients obtaining a microalbumin screening after initiation of the program.
A more recent prospective, multicenter cohort study of 206 patients with uncontrolled type 2 diabetes had similar results.10 In collaboration with the primary care physician (PCP), clinical pharmacists provided medication therapy management through adjustment of antihyperglycemic, antihypertensive, or lipid-lowering medications. Additional interventions provided by the pharmacists included reviewing blood glucose logs, ordering and monitoring laboratory tests, performing sensory foot examinations, and providing patient education.
Implementation of PPCM reduced the average HbA1c by 1.2% and increased the percentage of patients achieving an HbA1c <7% by about 24%. The researchers also observed improvements in BP and LDL-C levels in this patient population.11
Asthma and beyond
Future studies may well show that the benefits of PPCM extend to the management of other chronic diseases. One prospective, pre-post study of 126 patients with asthma found that the number of emergency department (ED) visits and/or hospitalizations decreased 30% during 9 months with a PPCM intervention and then returned to levels similar to baseline once the intervention ceased.12 Other potential disease areas that have been studied, or are being studied, include chronic obstructive pulmonary disease, chronic kidney disease, dyslipidemia, and congestive heart failure.13
Benefits derive from altered health care utilization
Researchers attribute much of the benefit observed with PPCM to the increased—albeit different—health-care utilization among the patients in the intervention groups. In general, patients participating in PPCM have an increased total number of visits, but more of those visits are with pharmacists and fewer are with physicians; they also are prescribed more medications, but don’t necessarily take more pills per day.1,2,5 In the end, patients have been found to achieve significantly better disease control without compromising quality of life or satisfaction.2
Some studies have found that continued pharmacist involvement may be necessary to sustain the benefits achieved.6 However, other studies have suggested that the benefits are maintained even after discontinuation of the pharmacist intervention.14,15 Thus, further research is necessary to determine which patients may benefit most from ongoing involvement with a pharmacist.
How cost-effective is the PPCM model?
Implementing a PPCM model in a primary care setting often hinges upon whether the intervention will be cost-effective. Several studies have reported the cost-effectiveness of clinical pharmacists in the management of HTN.1,16,17
Borenstein and colleagues found significantly lower provider visit costs per patient in the PPCM group ($160) compared with the usual care group ($195), a difference that the authors attributed to a decreased number of visits to PCPs and an increased number of lower cost visits with pharmacists in the PPCM group.1 However, the difference could have been affected by the arbitrary measurement of physician-pharmacist collaboration time in the study.
Overcoming implementation challenges
Implementation of pharmacist collaboration within primary care medicine may pose a challenge, as the requirements and resources vary widely among primary care settings. Health-system administrators, for example, may need to reorganize the clinic structure and budget resources in order to overcome some of the obstacles to implementing a PPCM model.
Experts have reported several strategies that help in establishing PPCM within primary care clinics,18 including proactively identifying patients who may benefit from pharmacist intervention, requiring appropriate training and credentialing of pharmacists, and establishing a set schedule for pharmacists to interview patients. Clinics would also be well served to model interventions outlined in the studies mentioned in this article and provide adequate time for pharmacists to perform structured activities, including review of medication history, assessment of current disease state control, and adjustment of medication therapy regimens. And, of course, given the diversity of primary care settings, administrators will need to identify the specific PPCM strategies that best complement their respective collaborative practice plans and environments.
The lack of well-defined reimbursement models for pharmacy services has presented a challenge for generating revenue and effectively implementing PPCM within many primary care settings. Currently, the Centers for Medicare and Medicaid Services and third-party payers do not recognize pharmacists as independent providers, creating a barrier for obtaining reimbursement for clinical pharmacy services. Typically, pharmacists have charged for clinic visits under a consultant physician through the “incident to” billing model, with the option to bill at higher levels if the patient was seen jointly with the physician.
Can this model benefit the underserved?
A prospective, cluster-randomized clinic study has shown pharmacist intervention to reduce racial and socioeconomic disparities in the treatment of elevated BP.19 This study is the first to show that a team-care model can overcome inequalities arising from low income, low patient education status, and little or no insurance to produce the same health care benefit as in those with higher socioeconomic and educational status. This type of collaborative care model may be particularly beneficial when incorporated within a PCMH catering to underserved populations.20
However, sparse data currently exist regarding the benefits of the PPCM model within a PCMH, despite the fact that integration of this type of collaborative model is expected to contribute positively to patient care.21
Physician acceptance of pharmacist involvement is mixed
While physician acceptance of pharmacist recommendations is generally high, at least one study indicated that some health-care professionals in patient-care teams are reluctant to incorporate pharmacists into a PCMH. Reasons include difficulty in coordination of care with pharmacy services and limited knowledge by other professionals of pharmacists’ training.22
Centralization can combat a lack of resources
As noted earlier, primary care offices that implement PPCM models are mostly academically affiliated or are part of large health systems. Many private primary care offices lack the resources to employ a pharmacist in their office. As an alternative, prospective clinical trials are looking at a centralized, Web-based cardiovascular risk service managed by pharmacists.23,24 This service’s primary objective is to improve adherence to metric-based outcomes developed as part of The Guideline Advantage quality improvement program put forth by the American Cancer Society, American Diabetes Association, and the American Heart and Stroke Associations. (See http://www.guidelineadvantage.org/TGA/ for more information.)
Researchers hope to prove that a centralized, pharmacist-run, clinical service can meet metric-driven outcomes that many primary care offices are now being required to meet in order to receive compensation from insurance companies. One of these studies is specifically looking at rural private offices that lack many of the resources that many large academic offices possess.23 The study is ongoing and results are expected sometime in 2018.
CORRESPONDENCE
John G. Gums, PharmD, College of Pharmacy, University of Florida, 1225 Center Drive, HPNP 4332, Gainesville, FL 32601; [email protected].
Over the past decade, physician-pharmacist collaborative practices have gained traction in primary care as a way to implement team-based-care models. And there is evidence pointing to the effectiveness of this multidisciplinary heath care team approach, in which pharmacists are typically responsible for such things as obtaining medication histories, identifying barriers to adherence, and adjusting medication regimens.
Several studies have shown the significant impact that physician-pharmacist collaborative management (PPCM) can have on blood pressure (BP) control among patients with hypertension (HTN).1-8 Additionally, PPCM may have positive effects on HbA1c reduction and diabetes control,9-11 suggesting that benefits may extend to other chronic diseases, too.
In the review that follows, we’ll detail the impact that PPCM can have on patient care, health-care utilization, and cost effectiveness. (For a look at PPCM “in action,” see the sidebar below.) We’ll also review the challenges of implementing this model that, at present, is mostly found in academically-affiliated clinics and large health systems.
SIDEBAR
The physician-pharmacist collaborative care model in actionFor patients with chronic diseases such as hypertension and diabetes, pharmacists can be invaluable members of multidisciplinary health care teams by providing direct consultation to optimize pharmacotherapy. Although their particular role and responsibilities can vary widely from one primary care setting to the next, the following describes the general workflow of a physician-pharmacist collaborative care model in action.
The patient, 60-year-old Isabel B, arrives for an appointment for pharmacotherapy management of her hypertension. After checking in, a registered nurse (RN), medical assistant (MA), or the pharmacist obtains her vital signs, height, and weight prior to rooming. Additionally, any necessary point-of-care lab tests are obtained at this time.
Once the patient is roomed, the pharmacist collects a thorough medication history from Ms. B, verifying and updating her current medication list, confirming the dose and frequency of each medication, and gathering information regarding adverse effects and barriers to adherence. The pharmacist may also review current laboratory results and vital signs to assess the appropriateness and therapeutic efficacy of the current drug therapy regimen.
Depending upon the collaborative practice plan in place, one of the following steps may occur:
A. The pharmacist makes a change to Ms. B's medication regimen and orders any necessary laboratory tests for monitoring. A progress note is forwarded to Ms. B's primary care provider (PCP) to inform him/her of the changes made to the regimen and the follow-up interval.
B. The pharmacist presents pharmacotherapy recommendations to the attending physician or Ms. B's PCP. The therapeutic and monitoring plans are discussed and approved as a team at the time of Ms. B's visit.
C. The pharmacist sends a message to Ms. B's PCP regarding information discovered during the interview and provides recommendations for a treatment plan based on the visit. The PCP reviews the recommendations, and can either 1) send approval to the pharmacist through a message or 2) implement the appropriate drug therapy changes at Ms. B's next visit.
In Cases A and B, the pharmacist then reviews the final pharmacotherapy plan with Ms. B, discusses the medication and monitoring parameters, answers any questions related to the new treatment regimen, and schedules a follow-up visit. In Case C, the pharmacist may still provide medication counseling and answer questions related to drug therapy during the visit; however, review of the final pharmacotherapy plan may be done over the telephone after approval by the PCP. Alternatively, a follow-up appointment with Ms. B's PCP can be scheduled shortly after the visit with the pharmacist to discuss any recommended drug therapy changes.
PPCM impacts chronic diseases
The current literature is rife with studies investigating the impact of PPCM on chronic diseases in the primary care setting.1-12 Although no specific guidelines on implementing PPCM exist, these studies utilized similar interventions that provided pharmacists with the ability to manage medication therapy under the supervision of a physician. A number of these studies incorporated collaborative practice plans to delineate the specific duties performed by physicians and pharmacists.2,6,8,10,11 Responsibilities for pharmacists often included assessing vital signs, reviewing laboratory parameters and ordering appropriate tests, providing patient education, screening for drug interactions, identifying barriers to medication adherence, and adjusting medication regimens. The TABLE1-12 provides a summary of studies investigating the impact of PPCM in the primary care setting.
PPCM leads to greater BP reductions, improved BP control
The majority of research surrounding PPCM has focused on uncontrolled HTN.1-8 Patients in many of these studies saw a pharmacist in a specialized HTN clinic, where the multidisciplinary staff performed a thorough evaluation of the patient’s current hypertensive management. The pharmacists in these PPCM programs closely monitored patients and made adjustments to antihypertensive regimens as necessary. Systolic and diastolic BP reductions in the intervention groups ranged from 14 to 36 mm Hg and 7 to 15 mm Hg, respectively.1-5,7,8 The percentage of patients with BP control at the end of the studies ranged from 43% to 89%.1,3,4,6,7
In a prospective, cluster-randomized trial performed at 32 primary care offices in 15 states, researchers assigned 625 patients with uncontrolled HTN to receive physician-pharmacist collaborative care or usual care with primary care provider management.7 As part of the PPCM intervention, clinical pharmacists conducted a thorough medical record review and a structured interview of the patients. During the interview, the clinical pharmacists reviewed the patient’s medication history, assessed the patient’s knowledge of BP medications, and addressed any barriers to adherence. In collaboration with the physician, the pharmacists developed a care plan with recommendations for optimizing the drug regimen. After the baseline visit, the pharmacists conducted structured face-to-face interviews with patients at 1, 2, 4, 6, and 8 months, with additional visits scheduled if BP was still uncontrolled.
At 9 months, patients in the PPCM group had significantly greater reductions in BP than those in the control group, and BP control was achieved in 43% of the PPCM group vs 34% of the control group. This study corroborates results from previous (similar) studies investigating the impact of PPCM on patients with uncontrolled HTN.1-6
PPCM helps patients reduce their HbA1c levels
Researchers have also studied the impact of PPCM strategies on the management of diabetes mellitus.9-11 In one retrospective study of 157 patients, implementation of a pharmacy-coordinated diabetes (any type) management program significantly improved HbA1c and increased the percentage of patients reaching their HbA1c goal.9 Furthermore, researchers observed improvements in low-density lipoprotein cholesterol (LDL-C) levels and an increased number of patients obtaining a microalbumin screening after initiation of the program.
A more recent prospective, multicenter cohort study of 206 patients with uncontrolled type 2 diabetes had similar results.10 In collaboration with the primary care physician (PCP), clinical pharmacists provided medication therapy management through adjustment of antihyperglycemic, antihypertensive, or lipid-lowering medications. Additional interventions provided by the pharmacists included reviewing blood glucose logs, ordering and monitoring laboratory tests, performing sensory foot examinations, and providing patient education.
Implementation of PPCM reduced the average HbA1c by 1.2% and increased the percentage of patients achieving an HbA1c <7% by about 24%. The researchers also observed improvements in BP and LDL-C levels in this patient population.11
Asthma and beyond
Future studies may well show that the benefits of PPCM extend to the management of other chronic diseases. One prospective, pre-post study of 126 patients with asthma found that the number of emergency department (ED) visits and/or hospitalizations decreased 30% during 9 months with a PPCM intervention and then returned to levels similar to baseline once the intervention ceased.12 Other potential disease areas that have been studied, or are being studied, include chronic obstructive pulmonary disease, chronic kidney disease, dyslipidemia, and congestive heart failure.13
Benefits derive from altered health care utilization
Researchers attribute much of the benefit observed with PPCM to the increased—albeit different—health-care utilization among the patients in the intervention groups. In general, patients participating in PPCM have an increased total number of visits, but more of those visits are with pharmacists and fewer are with physicians; they also are prescribed more medications, but don’t necessarily take more pills per day.1,2,5 In the end, patients have been found to achieve significantly better disease control without compromising quality of life or satisfaction.2
Some studies have found that continued pharmacist involvement may be necessary to sustain the benefits achieved.6 However, other studies have suggested that the benefits are maintained even after discontinuation of the pharmacist intervention.14,15 Thus, further research is necessary to determine which patients may benefit most from ongoing involvement with a pharmacist.
How cost-effective is the PPCM model?
Implementing a PPCM model in a primary care setting often hinges upon whether the intervention will be cost-effective. Several studies have reported the cost-effectiveness of clinical pharmacists in the management of HTN.1,16,17
Borenstein and colleagues found significantly lower provider visit costs per patient in the PPCM group ($160) compared with the usual care group ($195), a difference that the authors attributed to a decreased number of visits to PCPs and an increased number of lower cost visits with pharmacists in the PPCM group.1 However, the difference could have been affected by the arbitrary measurement of physician-pharmacist collaboration time in the study.
Overcoming implementation challenges
Implementation of pharmacist collaboration within primary care medicine may pose a challenge, as the requirements and resources vary widely among primary care settings. Health-system administrators, for example, may need to reorganize the clinic structure and budget resources in order to overcome some of the obstacles to implementing a PPCM model.
Experts have reported several strategies that help in establishing PPCM within primary care clinics,18 including proactively identifying patients who may benefit from pharmacist intervention, requiring appropriate training and credentialing of pharmacists, and establishing a set schedule for pharmacists to interview patients. Clinics would also be well served to model interventions outlined in the studies mentioned in this article and provide adequate time for pharmacists to perform structured activities, including review of medication history, assessment of current disease state control, and adjustment of medication therapy regimens. And, of course, given the diversity of primary care settings, administrators will need to identify the specific PPCM strategies that best complement their respective collaborative practice plans and environments.
The lack of well-defined reimbursement models for pharmacy services has presented a challenge for generating revenue and effectively implementing PPCM within many primary care settings. Currently, the Centers for Medicare and Medicaid Services and third-party payers do not recognize pharmacists as independent providers, creating a barrier for obtaining reimbursement for clinical pharmacy services. Typically, pharmacists have charged for clinic visits under a consultant physician through the “incident to” billing model, with the option to bill at higher levels if the patient was seen jointly with the physician.
Can this model benefit the underserved?
A prospective, cluster-randomized clinic study has shown pharmacist intervention to reduce racial and socioeconomic disparities in the treatment of elevated BP.19 This study is the first to show that a team-care model can overcome inequalities arising from low income, low patient education status, and little or no insurance to produce the same health care benefit as in those with higher socioeconomic and educational status. This type of collaborative care model may be particularly beneficial when incorporated within a PCMH catering to underserved populations.20
However, sparse data currently exist regarding the benefits of the PPCM model within a PCMH, despite the fact that integration of this type of collaborative model is expected to contribute positively to patient care.21
Physician acceptance of pharmacist involvement is mixed
While physician acceptance of pharmacist recommendations is generally high, at least one study indicated that some health-care professionals in patient-care teams are reluctant to incorporate pharmacists into a PCMH. Reasons include difficulty in coordination of care with pharmacy services and limited knowledge by other professionals of pharmacists’ training.22
Centralization can combat a lack of resources
As noted earlier, primary care offices that implement PPCM models are mostly academically affiliated or are part of large health systems. Many private primary care offices lack the resources to employ a pharmacist in their office. As an alternative, prospective clinical trials are looking at a centralized, Web-based cardiovascular risk service managed by pharmacists.23,24 This service’s primary objective is to improve adherence to metric-based outcomes developed as part of The Guideline Advantage quality improvement program put forth by the American Cancer Society, American Diabetes Association, and the American Heart and Stroke Associations. (See http://www.guidelineadvantage.org/TGA/ for more information.)
Researchers hope to prove that a centralized, pharmacist-run, clinical service can meet metric-driven outcomes that many primary care offices are now being required to meet in order to receive compensation from insurance companies. One of these studies is specifically looking at rural private offices that lack many of the resources that many large academic offices possess.23 The study is ongoing and results are expected sometime in 2018.
CORRESPONDENCE
John G. Gums, PharmD, College of Pharmacy, University of Florida, 1225 Center Drive, HPNP 4332, Gainesville, FL 32601; [email protected].
1. Borenstein JE, Graber G, Saltiel E, et al. Physician-pharmacist comanagement of hypertension: a randomized, comparative trial. Pharmacotherapy. 2003;23:209-216.
2. Hunt JS, Siemienczuk J, Pape G, et al. A randomized controlled trial of team-based care: impact of physician-pharmacist collaboration on uncontrolled hypertension. J Gen Intern Med. 2008;23:1966-1972.
3. Carter BL, Bergus GR, Dawson JD, et al. A cluster randomized trial to evaluate physician/pharmacist collaboration to improve blood pressure control. J Clin Hypertens (Greenwich). 2008;10:260-271.
4. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. 2009;169:1996-2002.
5. Weber CA, Ernst ME, Sezate GS, et al. Pharmacist-physician comanagement of hypertension and reduction in 24-hour ambulatory blood pressures. Arch Intern Med. 2010;170:1634-1639.
6. Hirsch JD, Steers N, Adler DS, et al. Primary care-based, pharmacist-physician collaborative medication-therapy management of hypertension: a randomized, pragmatic trial. Clin Ther. 2014;36:1244-1254.
7. Carter BL, Coffey CS, Ardery G, et al. Cluster-randomized trial of a physician/pharmacist collaborative model to improve blood pressure control. Circ Cardiovasc Qual Outcomes. 2015;8:235-243.
8. Sisson EM, Dixon DL, Kildow DC, et al. Effectiveness of a pharmacist-physician team-based collaboration to improve long-term blood pressure control at an inner-city safety-net clinic. Pharmacotherapy. 2016;36:342-347.
9. Kiel PJ, McCord AD. Pharmacist impact on clinical outcomes in a diabetes disease management program via collaborative practice. Ann Pharmacother. 2005;39:1828-1832.
10. Farland MZ, Byrd DC, McFarland MS, et al. Pharmacist-physician collaboration for diabetes care: the diabetes initiative program. Ann Pharmacother. 2013;47:781-789.
11. Howard-Thompson A, Farland MZ, Byrd DC, et al. Pharmacist-physician collaboration for diabetes care: cardiovascular outcomes. Ann Pharmacother. 2013;47:1471-1477.
12. Gums TH, Carter BL, Milavetz G, et al. Physician-pharmacist collaborative management of asthma in primary care. Pharmacotherapy. 2014;34:1033-1042.
13. Greer N, Bolduc J, Geurkink E, et al. VA Evidence-based Synthesis Program Reports. Pharmacist-Led Chronic Disease Management: A Systematic Review of Effectiveness and Harms Compared to Usual Care. Washington (DC): Department of Veterans Affairs (US); 2015.
14. Wentzlaff DM, Carter BL, Ardery G, et al. Sustained blood pressure control following discontinuation of a pharmacist intervention. J Clin Hypertens (Greenwich). 2011;13:431-437.
15. Carter BL, Vander Weg MW, Parker CP, et al. Sustained blood pressure control following discontinuation of a pharmacist intervention for veterans. J Clin Hypertens (Greenwich). 2015;17:701-708.
16. Kulchaitanaroaj P, Brooks JM, Ardery G, et al. Incremental costs associated with physician and pharmacist collaboration to improve blood pressure control. Pharmacotherapy. 2012;32:772-780.
17. Polgreen LA, Han J, Carter BL, et al. Cost effectiveness of a physician-pharmacist collaboration intervention to improve blood pressure control. Hypertension. 2015;66:1145-1151.
18. Carter BL. Primary care physician-pharmacist collaborative care model: strategies for implementation. Pharmacotherapy. 2016;36:363-373.
19. Anderegg MD, Gums TH, Uribe L, et al. Physician-pharmacist collaborative management: narrowing the socioeconomic blood pressure gap. Hypertension. 2016;68:1314-1320.
20. Moczygemba LR, Goode JV, Gatewood SBS, et al. Integration of collaborative medication therapy management in a safety net patient-centered medical home. J Am Pharm Assoc (2003). 2011;51:167-172.
21. Scott MA, Hitch B, Ray L, et al. Integration of pharmacists into a patient-centered medical home. J Am Pharm Assoc (2003). 2011;51:161-166.
22. Patterson BJ, Solimeo SL, Stewart KR, et al. Perceptions of pharmacists’ integration into patient-centered medical home teams. Res Social Adm Pharm. 2015;11:85-95.
23. Carter BL, Levy BT, Gryzlak B, et al. A centralized cardiovascular risk service to improve guideline adherence in private primary care offices. Contemp Clin Trials. 2015;43:25-32.
24. Carter BL, Coffey CS, Chrischilles EA, et al. A cluster-randomized trial of a centralized clinical pharmacy cardiovascular risk service to improve guideline adherence. Pharmacotherapy. 2015;35:653-662.
1. Borenstein JE, Graber G, Saltiel E, et al. Physician-pharmacist comanagement of hypertension: a randomized, comparative trial. Pharmacotherapy. 2003;23:209-216.
2. Hunt JS, Siemienczuk J, Pape G, et al. A randomized controlled trial of team-based care: impact of physician-pharmacist collaboration on uncontrolled hypertension. J Gen Intern Med. 2008;23:1966-1972.
3. Carter BL, Bergus GR, Dawson JD, et al. A cluster randomized trial to evaluate physician/pharmacist collaboration to improve blood pressure control. J Clin Hypertens (Greenwich). 2008;10:260-271.
4. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. 2009;169:1996-2002.
5. Weber CA, Ernst ME, Sezate GS, et al. Pharmacist-physician comanagement of hypertension and reduction in 24-hour ambulatory blood pressures. Arch Intern Med. 2010;170:1634-1639.
6. Hirsch JD, Steers N, Adler DS, et al. Primary care-based, pharmacist-physician collaborative medication-therapy management of hypertension: a randomized, pragmatic trial. Clin Ther. 2014;36:1244-1254.
7. Carter BL, Coffey CS, Ardery G, et al. Cluster-randomized trial of a physician/pharmacist collaborative model to improve blood pressure control. Circ Cardiovasc Qual Outcomes. 2015;8:235-243.
8. Sisson EM, Dixon DL, Kildow DC, et al. Effectiveness of a pharmacist-physician team-based collaboration to improve long-term blood pressure control at an inner-city safety-net clinic. Pharmacotherapy. 2016;36:342-347.
9. Kiel PJ, McCord AD. Pharmacist impact on clinical outcomes in a diabetes disease management program via collaborative practice. Ann Pharmacother. 2005;39:1828-1832.
10. Farland MZ, Byrd DC, McFarland MS, et al. Pharmacist-physician collaboration for diabetes care: the diabetes initiative program. Ann Pharmacother. 2013;47:781-789.
11. Howard-Thompson A, Farland MZ, Byrd DC, et al. Pharmacist-physician collaboration for diabetes care: cardiovascular outcomes. Ann Pharmacother. 2013;47:1471-1477.
12. Gums TH, Carter BL, Milavetz G, et al. Physician-pharmacist collaborative management of asthma in primary care. Pharmacotherapy. 2014;34:1033-1042.
13. Greer N, Bolduc J, Geurkink E, et al. VA Evidence-based Synthesis Program Reports. Pharmacist-Led Chronic Disease Management: A Systematic Review of Effectiveness and Harms Compared to Usual Care. Washington (DC): Department of Veterans Affairs (US); 2015.
14. Wentzlaff DM, Carter BL, Ardery G, et al. Sustained blood pressure control following discontinuation of a pharmacist intervention. J Clin Hypertens (Greenwich). 2011;13:431-437.
15. Carter BL, Vander Weg MW, Parker CP, et al. Sustained blood pressure control following discontinuation of a pharmacist intervention for veterans. J Clin Hypertens (Greenwich). 2015;17:701-708.
16. Kulchaitanaroaj P, Brooks JM, Ardery G, et al. Incremental costs associated with physician and pharmacist collaboration to improve blood pressure control. Pharmacotherapy. 2012;32:772-780.
17. Polgreen LA, Han J, Carter BL, et al. Cost effectiveness of a physician-pharmacist collaboration intervention to improve blood pressure control. Hypertension. 2015;66:1145-1151.
18. Carter BL. Primary care physician-pharmacist collaborative care model: strategies for implementation. Pharmacotherapy. 2016;36:363-373.
19. Anderegg MD, Gums TH, Uribe L, et al. Physician-pharmacist collaborative management: narrowing the socioeconomic blood pressure gap. Hypertension. 2016;68:1314-1320.
20. Moczygemba LR, Goode JV, Gatewood SBS, et al. Integration of collaborative medication therapy management in a safety net patient-centered medical home. J Am Pharm Assoc (2003). 2011;51:167-172.
21. Scott MA, Hitch B, Ray L, et al. Integration of pharmacists into a patient-centered medical home. J Am Pharm Assoc (2003). 2011;51:161-166.
22. Patterson BJ, Solimeo SL, Stewart KR, et al. Perceptions of pharmacists’ integration into patient-centered medical home teams. Res Social Adm Pharm. 2015;11:85-95.
23. Carter BL, Levy BT, Gryzlak B, et al. A centralized cardiovascular risk service to improve guideline adherence in private primary care offices. Contemp Clin Trials. 2015;43:25-32.
24. Carter BL, Coffey CS, Chrischilles EA, et al. A cluster-randomized trial of a centralized clinical pharmacy cardiovascular risk service to improve guideline adherence. Pharmacotherapy. 2015;35:653-662.
PRACTICE RECOMMENDATIONS
› Consider physician-pharmacist collaboration as a way by which to improve the management of your patients with hypertension and diabetes. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
