User login
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
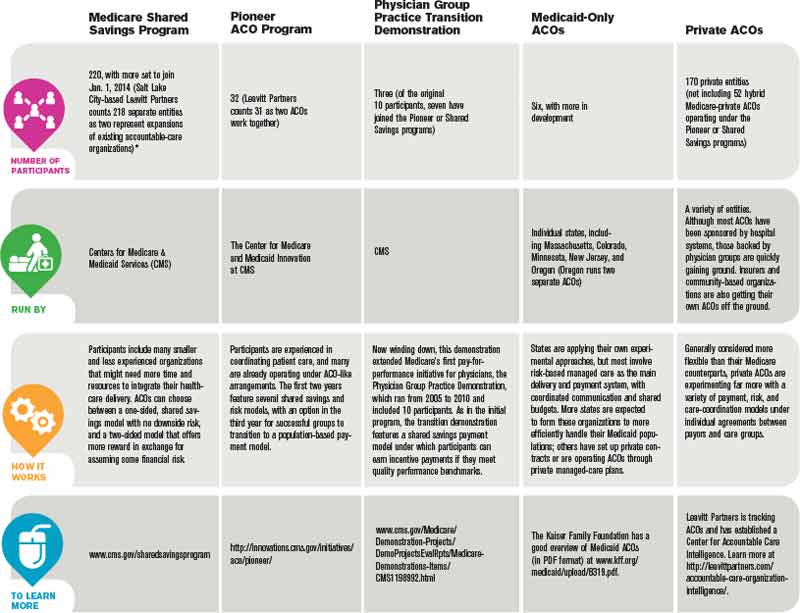
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.

—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”

Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.

—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.

Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.
—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”
Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.
—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.
Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.
—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”
Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.
—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.
Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.