User login
Pregnancy after breast cancer is rockier but doesn't increase recurrence risk
Key clinical point: Breast cancer survivors are less likely to conceive and have more complications when they do, but pregnancy does not increase the risk of cancer recurrence, a review suggests.
Major finding: Relative to the general population, breast cancer survivors were 60% less likely to become pregnant, and they had higher odds of complications such as preterm birth (45% higher) and low birth weight (50% higher), but their risk of cancer recurrence was not increased.
Study details: A systematic review and meta-analysis using data from 39 studies that included a total of 114,573 breast cancer patients and 8,093,401 women from the general population.
Disclosures: The study was funded by the Italian Ministry of Health and the Italian Association for Cancer Research. Dr. Blondeaux disclosed no conflicts of interest.
Source: Blondeaux et al. SABCS 2020, Abstract GS3-09.
Key clinical point: Breast cancer survivors are less likely to conceive and have more complications when they do, but pregnancy does not increase the risk of cancer recurrence, a review suggests.
Major finding: Relative to the general population, breast cancer survivors were 60% less likely to become pregnant, and they had higher odds of complications such as preterm birth (45% higher) and low birth weight (50% higher), but their risk of cancer recurrence was not increased.
Study details: A systematic review and meta-analysis using data from 39 studies that included a total of 114,573 breast cancer patients and 8,093,401 women from the general population.
Disclosures: The study was funded by the Italian Ministry of Health and the Italian Association for Cancer Research. Dr. Blondeaux disclosed no conflicts of interest.
Source: Blondeaux et al. SABCS 2020, Abstract GS3-09.
Key clinical point: Breast cancer survivors are less likely to conceive and have more complications when they do, but pregnancy does not increase the risk of cancer recurrence, a review suggests.
Major finding: Relative to the general population, breast cancer survivors were 60% less likely to become pregnant, and they had higher odds of complications such as preterm birth (45% higher) and low birth weight (50% higher), but their risk of cancer recurrence was not increased.
Study details: A systematic review and meta-analysis using data from 39 studies that included a total of 114,573 breast cancer patients and 8,093,401 women from the general population.
Disclosures: The study was funded by the Italian Ministry of Health and the Italian Association for Cancer Research. Dr. Blondeaux disclosed no conflicts of interest.
Source: Blondeaux et al. SABCS 2020, Abstract GS3-09.
Adding atezolizumab to chemo doesn’t worsen QOL in early TNBC
Key clinical point: Adding immunotherapy to chemotherapy for early triple-negative breast cancer did not increase symptom burden.
Major finding: Health-related quality-of-life measures were similar whether patients received chemotherapy with atezolizumab or with placebo. For example, mean physical function scores were about 90% in both treatment arms at baseline, dropped to about 65% in each arm by cycle 5, and rebounded to about 80% by cycle 7.
Study details: Exploratory patient-reported outcomes from 328 patients in the phase 3 IMpassion031 trial.
Disclosures: IMpassion031 is sponsored by F. Hoffman-LaRoche. Dr. Mittendorf disclosed relationships with Roche/Genentech, GlaxoSmithKline, Physicians’ Education Resource, AstraZeneca, Exact Sciences, Merck, Peregrine Pharmaceuticals, SELLAS Life Sciences, TapImmune, EMD Serono, Galena Biopharma, Bristol Myers Squibb, and Lilly.
Source: Mittendorf E at al. SABCS 2020, Abstract GS3-02.
Key clinical point: Adding immunotherapy to chemotherapy for early triple-negative breast cancer did not increase symptom burden.
Major finding: Health-related quality-of-life measures were similar whether patients received chemotherapy with atezolizumab or with placebo. For example, mean physical function scores were about 90% in both treatment arms at baseline, dropped to about 65% in each arm by cycle 5, and rebounded to about 80% by cycle 7.
Study details: Exploratory patient-reported outcomes from 328 patients in the phase 3 IMpassion031 trial.
Disclosures: IMpassion031 is sponsored by F. Hoffman-LaRoche. Dr. Mittendorf disclosed relationships with Roche/Genentech, GlaxoSmithKline, Physicians’ Education Resource, AstraZeneca, Exact Sciences, Merck, Peregrine Pharmaceuticals, SELLAS Life Sciences, TapImmune, EMD Serono, Galena Biopharma, Bristol Myers Squibb, and Lilly.
Source: Mittendorf E at al. SABCS 2020, Abstract GS3-02.
Key clinical point: Adding immunotherapy to chemotherapy for early triple-negative breast cancer did not increase symptom burden.
Major finding: Health-related quality-of-life measures were similar whether patients received chemotherapy with atezolizumab or with placebo. For example, mean physical function scores were about 90% in both treatment arms at baseline, dropped to about 65% in each arm by cycle 5, and rebounded to about 80% by cycle 7.
Study details: Exploratory patient-reported outcomes from 328 patients in the phase 3 IMpassion031 trial.
Disclosures: IMpassion031 is sponsored by F. Hoffman-LaRoche. Dr. Mittendorf disclosed relationships with Roche/Genentech, GlaxoSmithKline, Physicians’ Education Resource, AstraZeneca, Exact Sciences, Merck, Peregrine Pharmaceuticals, SELLAS Life Sciences, TapImmune, EMD Serono, Galena Biopharma, Bristol Myers Squibb, and Lilly.
Source: Mittendorf E at al. SABCS 2020, Abstract GS3-02.
Depression, sleep disorders linked to early mortality in breast cancer
Key clinical point: Comorbid depression, sleep disorders, or their combination is associated with early mortality in women with breast cancer.
Major finding: Depression (adjusted hazard ratio [aHR], 1.44; 95% confidence interval [CI], 1.17-1.78) and sleep disorders (aHR, 1.37; 95% CI, 1.02-1.84) were significantly associated with an increase in 5-year mortality. For the combination of depression and sleep disorders, aHR was 1.75 (95% CI: 1.17-2.60).
Study details: The data come from a retrospective cohort study of women diagnosed with breast cancer (2008-2012) in 1 of 200 general practices in the UK (n = 6,656; age, 18-80 years).
Disclosures: The study did not receive any funding. The authors declared no conflicts of interest.
Source: Bach L et al. J Psychiatr Res. 2020 Nov 23. doi: 10.1016/j.jpsychires.2020.11.036.
Key clinical point: Comorbid depression, sleep disorders, or their combination is associated with early mortality in women with breast cancer.
Major finding: Depression (adjusted hazard ratio [aHR], 1.44; 95% confidence interval [CI], 1.17-1.78) and sleep disorders (aHR, 1.37; 95% CI, 1.02-1.84) were significantly associated with an increase in 5-year mortality. For the combination of depression and sleep disorders, aHR was 1.75 (95% CI: 1.17-2.60).
Study details: The data come from a retrospective cohort study of women diagnosed with breast cancer (2008-2012) in 1 of 200 general practices in the UK (n = 6,656; age, 18-80 years).
Disclosures: The study did not receive any funding. The authors declared no conflicts of interest.
Source: Bach L et al. J Psychiatr Res. 2020 Nov 23. doi: 10.1016/j.jpsychires.2020.11.036.
Key clinical point: Comorbid depression, sleep disorders, or their combination is associated with early mortality in women with breast cancer.
Major finding: Depression (adjusted hazard ratio [aHR], 1.44; 95% confidence interval [CI], 1.17-1.78) and sleep disorders (aHR, 1.37; 95% CI, 1.02-1.84) were significantly associated with an increase in 5-year mortality. For the combination of depression and sleep disorders, aHR was 1.75 (95% CI: 1.17-2.60).
Study details: The data come from a retrospective cohort study of women diagnosed with breast cancer (2008-2012) in 1 of 200 general practices in the UK (n = 6,656; age, 18-80 years).
Disclosures: The study did not receive any funding. The authors declared no conflicts of interest.
Source: Bach L et al. J Psychiatr Res. 2020 Nov 23. doi: 10.1016/j.jpsychires.2020.11.036.
Impact of BMI on overall survival in women with metastatic breast cancer
Key clinical point: Underweight appears as an independent negative prognostic factor for both overall survival (OS) and first-line progression-free survival (PFS) in women with metastatic breast cancer (MBC). In contrast, overweight and obesity are not associated with poorer outcomes.
Major finding: The median OS was 47.4 months (median follow-up, 48.6 months). Underweight (body mass index [BMI], less than 18.5 kg/m2) showed an independent association with worse OS (median OS, 33 months; hazard ratio [HR ], 1.14; 95% confidence interval [CI], 1.02-1.28) and first-line PFS (HR, 1.11; 95% CI, 1.01-1.22). Overweight (BMI, 25.0-29.9 kg/m2) or obesity (BMI, 30.0 kg/m2 or higher) had no impact on OS.
Study details: This study evaluated the impact of BMI on survival outcomes among patients with metastatic breast cancer (n = 12,999) in the ESME-MBC cohort (median BMI, 24.9 kg/m2; 20% of women were obese and 5% underweight).
Disclosures: The ESME MBC database receives financial support from an industrial consortium (Roche, Pfizer, AstraZeneca, MSD, Eisai, and Daiichi Sankyo). Dr. K Saleh had no disclosures. Some of his coinvestigators reported ties with pharmaceutical companies.
Source: Saleh K et al. Breast. 2020 Dec 1. doi: 10.1016/j.breast.2020.11.014.
Key clinical point: Underweight appears as an independent negative prognostic factor for both overall survival (OS) and first-line progression-free survival (PFS) in women with metastatic breast cancer (MBC). In contrast, overweight and obesity are not associated with poorer outcomes.
Major finding: The median OS was 47.4 months (median follow-up, 48.6 months). Underweight (body mass index [BMI], less than 18.5 kg/m2) showed an independent association with worse OS (median OS, 33 months; hazard ratio [HR ], 1.14; 95% confidence interval [CI], 1.02-1.28) and first-line PFS (HR, 1.11; 95% CI, 1.01-1.22). Overweight (BMI, 25.0-29.9 kg/m2) or obesity (BMI, 30.0 kg/m2 or higher) had no impact on OS.
Study details: This study evaluated the impact of BMI on survival outcomes among patients with metastatic breast cancer (n = 12,999) in the ESME-MBC cohort (median BMI, 24.9 kg/m2; 20% of women were obese and 5% underweight).
Disclosures: The ESME MBC database receives financial support from an industrial consortium (Roche, Pfizer, AstraZeneca, MSD, Eisai, and Daiichi Sankyo). Dr. K Saleh had no disclosures. Some of his coinvestigators reported ties with pharmaceutical companies.
Source: Saleh K et al. Breast. 2020 Dec 1. doi: 10.1016/j.breast.2020.11.014.
Key clinical point: Underweight appears as an independent negative prognostic factor for both overall survival (OS) and first-line progression-free survival (PFS) in women with metastatic breast cancer (MBC). In contrast, overweight and obesity are not associated with poorer outcomes.
Major finding: The median OS was 47.4 months (median follow-up, 48.6 months). Underweight (body mass index [BMI], less than 18.5 kg/m2) showed an independent association with worse OS (median OS, 33 months; hazard ratio [HR ], 1.14; 95% confidence interval [CI], 1.02-1.28) and first-line PFS (HR, 1.11; 95% CI, 1.01-1.22). Overweight (BMI, 25.0-29.9 kg/m2) or obesity (BMI, 30.0 kg/m2 or higher) had no impact on OS.
Study details: This study evaluated the impact of BMI on survival outcomes among patients with metastatic breast cancer (n = 12,999) in the ESME-MBC cohort (median BMI, 24.9 kg/m2; 20% of women were obese and 5% underweight).
Disclosures: The ESME MBC database receives financial support from an industrial consortium (Roche, Pfizer, AstraZeneca, MSD, Eisai, and Daiichi Sankyo). Dr. K Saleh had no disclosures. Some of his coinvestigators reported ties with pharmaceutical companies.
Source: Saleh K et al. Breast. 2020 Dec 1. doi: 10.1016/j.breast.2020.11.014.
Study supports clinical utility of CTC count for metastatic breast cancer
Key clinical point: Circulating tumor cell (CTC) count-driven first-line therapy (chemotherapy or endocrine therapy) is noninferior to clinician choice-driven first-line therapy for progression-free survival (PFS) in hormone receptor (HR)-positive/HER2-negative metastatic breast cancer.
Major finding: The median PFS was 15.5 (95% confidence interval [CI], 12.7-17.3) months in the CTC-guided group and 13.9 (95% CI, 12.2-16.3) months in the clinician-driven choice group. The primary end point (PFS in the per-protocol population with a noninferiority margin of 1.25 for the 90% CI of the hazard ratio [HR]) was met with an HR of 0.94 (90% CI, 0.81-1.09). Overall survival was also noninferior with CTC guidance (HR, 0.91; 95% CI, 0.71-1.16).
Study details: In this phase 3 STIC CTC trial, 755 women with HR-positive/HER2-negative metastatic breast cancer were randomly assigned (1:1) to receive a CTC-driven first-line therapy (chemotherapy if 5 CTCs or more/7.5 mL; endocrine therapy if less than 5 CTCs/7.5 mL) or clinician choice-driven first-line therapy (chemotherapy or endocrine therapy) at 17 French centers.
Disclosures: The study was funded by Institut Curie, the French National Cancer Institute as part of the Programme de Soutien aux Techniques Innovantes Coûteuses 2011, and Menarini Silicon Biosystems. The lead author reported receiving grants and nonfinancial support from Menarini Silicon Biosystems during the conduct of the study.
Source: Bidard FC et al. JAMA Oncol. 2020 Nov 5. doi: 10.1001/jamaoncol.2020.5660.
Key clinical point: Circulating tumor cell (CTC) count-driven first-line therapy (chemotherapy or endocrine therapy) is noninferior to clinician choice-driven first-line therapy for progression-free survival (PFS) in hormone receptor (HR)-positive/HER2-negative metastatic breast cancer.
Major finding: The median PFS was 15.5 (95% confidence interval [CI], 12.7-17.3) months in the CTC-guided group and 13.9 (95% CI, 12.2-16.3) months in the clinician-driven choice group. The primary end point (PFS in the per-protocol population with a noninferiority margin of 1.25 for the 90% CI of the hazard ratio [HR]) was met with an HR of 0.94 (90% CI, 0.81-1.09). Overall survival was also noninferior with CTC guidance (HR, 0.91; 95% CI, 0.71-1.16).
Study details: In this phase 3 STIC CTC trial, 755 women with HR-positive/HER2-negative metastatic breast cancer were randomly assigned (1:1) to receive a CTC-driven first-line therapy (chemotherapy if 5 CTCs or more/7.5 mL; endocrine therapy if less than 5 CTCs/7.5 mL) or clinician choice-driven first-line therapy (chemotherapy or endocrine therapy) at 17 French centers.
Disclosures: The study was funded by Institut Curie, the French National Cancer Institute as part of the Programme de Soutien aux Techniques Innovantes Coûteuses 2011, and Menarini Silicon Biosystems. The lead author reported receiving grants and nonfinancial support from Menarini Silicon Biosystems during the conduct of the study.
Source: Bidard FC et al. JAMA Oncol. 2020 Nov 5. doi: 10.1001/jamaoncol.2020.5660.
Key clinical point: Circulating tumor cell (CTC) count-driven first-line therapy (chemotherapy or endocrine therapy) is noninferior to clinician choice-driven first-line therapy for progression-free survival (PFS) in hormone receptor (HR)-positive/HER2-negative metastatic breast cancer.
Major finding: The median PFS was 15.5 (95% confidence interval [CI], 12.7-17.3) months in the CTC-guided group and 13.9 (95% CI, 12.2-16.3) months in the clinician-driven choice group. The primary end point (PFS in the per-protocol population with a noninferiority margin of 1.25 for the 90% CI of the hazard ratio [HR]) was met with an HR of 0.94 (90% CI, 0.81-1.09). Overall survival was also noninferior with CTC guidance (HR, 0.91; 95% CI, 0.71-1.16).
Study details: In this phase 3 STIC CTC trial, 755 women with HR-positive/HER2-negative metastatic breast cancer were randomly assigned (1:1) to receive a CTC-driven first-line therapy (chemotherapy if 5 CTCs or more/7.5 mL; endocrine therapy if less than 5 CTCs/7.5 mL) or clinician choice-driven first-line therapy (chemotherapy or endocrine therapy) at 17 French centers.
Disclosures: The study was funded by Institut Curie, the French National Cancer Institute as part of the Programme de Soutien aux Techniques Innovantes Coûteuses 2011, and Menarini Silicon Biosystems. The lead author reported receiving grants and nonfinancial support from Menarini Silicon Biosystems during the conduct of the study.
Source: Bidard FC et al. JAMA Oncol. 2020 Nov 5. doi: 10.1001/jamaoncol.2020.5660.
TNBC: Add-on ipatasertib fails to improve progression-free survival
Key clinical point: Addition of ipatasertib to paclitaxel does not improve progression-free survival (PFS) in patients with PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer (TNBC).
Major finding: The median PFS was 7.4 months with ipatasertib + paclitaxel vs 6.1 months with placebo + paclitaxel (hazard ratio, 1.02; P = .9237).
Study details: The data come from the Cohort A of phase 3 trial IPATunity130. 255 patients with PIK3CA/AKT1/PTEN-altered TNBC were randomly assigned (2:1) to receive paclitaxel with either ipatasertib or placebo.
Disclosures: The study was funded by Hoffmann-La Roche. The presenting author Rebecca Dent declared relationships with AstraZeneca, Eisai, Lilly, Merck, Novartis, Pfizer, and Roche.
Source: Dent R et al. Abstract 4. SABCS 2020. 2020 Dec 10.
Key clinical point: Addition of ipatasertib to paclitaxel does not improve progression-free survival (PFS) in patients with PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer (TNBC).
Major finding: The median PFS was 7.4 months with ipatasertib + paclitaxel vs 6.1 months with placebo + paclitaxel (hazard ratio, 1.02; P = .9237).
Study details: The data come from the Cohort A of phase 3 trial IPATunity130. 255 patients with PIK3CA/AKT1/PTEN-altered TNBC were randomly assigned (2:1) to receive paclitaxel with either ipatasertib or placebo.
Disclosures: The study was funded by Hoffmann-La Roche. The presenting author Rebecca Dent declared relationships with AstraZeneca, Eisai, Lilly, Merck, Novartis, Pfizer, and Roche.
Source: Dent R et al. Abstract 4. SABCS 2020. 2020 Dec 10.
Key clinical point: Addition of ipatasertib to paclitaxel does not improve progression-free survival (PFS) in patients with PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer (TNBC).
Major finding: The median PFS was 7.4 months with ipatasertib + paclitaxel vs 6.1 months with placebo + paclitaxel (hazard ratio, 1.02; P = .9237).
Study details: The data come from the Cohort A of phase 3 trial IPATunity130. 255 patients with PIK3CA/AKT1/PTEN-altered TNBC were randomly assigned (2:1) to receive paclitaxel with either ipatasertib or placebo.
Disclosures: The study was funded by Hoffmann-La Roche. The presenting author Rebecca Dent declared relationships with AstraZeneca, Eisai, Lilly, Merck, Novartis, Pfizer, and Roche.
Source: Dent R et al. Abstract 4. SABCS 2020. 2020 Dec 10.
Sequential Targeted Treatment for a Geriatric Patient with Acute Myeloid Leukemia with Concurrent FLT3-TKD and IDH1 Mutations
Nearly 20,000 patients are diagnosed with acute myeloid leukemia (AML) in the US annually.1 Despite the use of aggressive chemotherapeutic agents, the prognosis remains poor, with a mean 5-year survival of 28.3%.2 Fortunately, with the refinement of next-generation sequencing (NGS) hematology panels and development of systemic targeted therapies, the treatment landscape for eligible patients has improved, both in frontline and relapsed or refractory (R/R) patients.
Specifically, investigations into alterations within the FMS-like tyrosine kinase (FLT3) and isocitrate dehydrogenase (IDH) genes have led to the discovery of a number of targeted treatments. Midostaurin is US Food and Drug Administration (FDA)-approved for use in combination with induction chemotherapy for patients with internal tandem duplication of the FLT3 (FLT3-ITD) gene or mutations within the tyrosine kinase domain (FLT3-TKD).3 Ivosidenib is indicated for frontline treatment for those who are poor candidates for induction chemotherapy, and R/R patients who have an R132H mutation in IDH1.4,5 Enasidenib is FDA-approved for R/R patients with R140Q, R172S, and R172K mutations in IDH2.6
The optimal treatment for patients with AML with ≥ 2 clinically actionable mutations has not been established. In this article we describe a geriatric patient who initially was diagnosed with AML with concurrent FLT3-TKD and IDH1 mutations and received targeted, sequential management. We detail changes in disease phenotype and mutational status by repeating an NGS hematology panel and cytogenetic studies after each stage of therapy. Lastly, we discuss the clonal evolution apparent within leukemic cells with use of ≥ 1 or more targeted agents.
Case Presentation
A 68-year-old man presented to the Emergency Department at The Durham Veterans Affairs Medical Center in North Carolina with fatigue and light-headedness. Because of his symptoms and pancytopenia, a bone marrow aspiration and trephine biopsy were performed, which showed 57% myeloblasts, 12% promyelocytes/myelocytes, and 2% metamyelocytes in 20 to 30% cellular bone marrow. Flow cytometry confirmed a blast population consistent with AML. A LeukoVantage (Quest Diagnostics) hematologic NGS panel revealed the presence of FLT3-TKD, IDH1, RUNX1, BCOR-E1477, and SF3B1 mutations (Table). Initial fluorescence in situ hybridization (FISH) results showed a normal pattern of hybridization with no translocations. His disease was deemed to be intermediate-high risk because of the presence of FLT3-TKD and RUNX1 mutations, despite the normal cytogenetic profile and absence of additional clinical features.
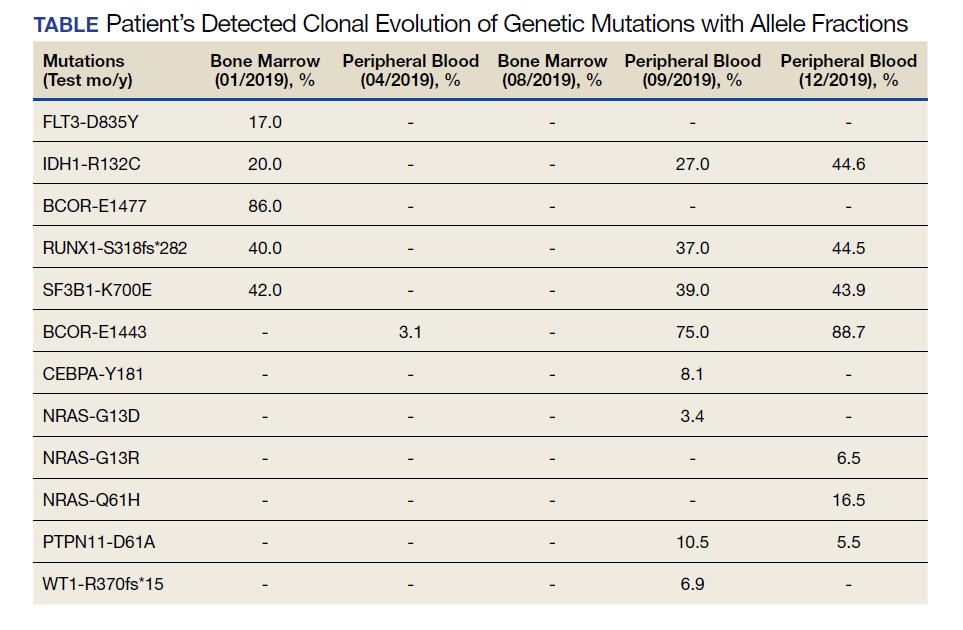
Induction chemotherapy was started with idarubicin, 12 mg/m2, on days 1 to 3 and cytarabine, 200 mg/m2, on days 1 to 7. Because of the presence of a FLT3-TKD mutation, midostaurin was planned for days 8 to 21. After induction chemotherapy, a bone marrow biopsy on day 14 revealed an acellular marrow with no observed myeloblasts. A bone marrow biopsy conducted before initiating consolidation therapy, revealed 30% cellularity with morphologic remission. However, flow cytometry found 5% myeloblasts expressing CD34, CD117, CD13, CD38, and HLA-DR, consistent with measurable residual disease. He received 2 cycles of consolidation therapy with high-dose cytarabine combined with midostaurin. After the patient's second cycle of consolidation, he continued to experience transfusion-dependent cytopenias. Another bone marrow evaluation demonstrated 10% cellularity with nearly all cells appearing to be myeloblasts. A repeat LeukoVantage NGS panel demonstrated undetectable FLT3-TKD mutation and persistent IDH1-R123C mutation. FISH studies revealed a complex karyotype with monosomy of chromosomes 5 and 7 and trisomy of chromosome 8.
We discussed with the patient and his family the options available, which included initiating targeted therapy for his IDH1 mutation, administering hypomethylation therapy with or without venetoclax, or pursuing palliative measures. We collectively decided to pursue therapy with single-agent oral ivosidenib, 500 mg daily. After 1 month of treatment, our patient developed worsening fatigue. His white blood cell count had increased to > 43 k/cm2, raising concern for differentiation syndrome.
A review of the peripheral smear showed a wide-spectrum of maturing granulocytes, with a large percentage of blasts. Peripheral flow cytometry confirmed a blast population of 15%. After a short period of symptom improvement with steroids, the patient developed worsening confusion. Brain imaging identified 2 subdural hemorrhages. Because of a significant peripheral blast population and the development of these hemorrhages, palliative measures were pursued, and the patient was discharged to an inpatient hospice facility. A final NGS panel performed from peripheral blood detected mutations in IDH1, RUNX1, PTPN11, NRAS, BCOR-E1443, and SF3B1 genes.
Discussion
To our knowledge, this is the first reported case of a patient who sequentially received targeted treatments directed against both FLT3 and IDH1 mutations. Initial management with midostaurin and cytarabine resulted in sustained remission of his FLT3-TKD mutation. However, despite receiving prompt standard of care with combination induction chemotherapy and targeted therapy, the patient experienced unfavorable clonal evolution based upon his molecular and cytogenetic testing. Addition of ivosidenib as a second targeting agent for his IDH1 mutation did not achieve a second remission.
Clonal evolution is a well-described phenomenon in hematology. Indolent conditions, such as clonal hematopoiesis of intermediate potential, or malignancies, such as myelodysplastic syndromes and myeloproliferative neoplasms, could transform into acute leukemia through the accumulation of driver mutations and/or cytogenetic abnormalities. Clonal evolution often is viewed as the culprit in patients with AML whose disease relapses after remission with initial chemotherapy.7-10 With the increasing availability of commercial NGS panels designed to assess mutations among patients experiencing hematologic malignancies, patterns of relapse, and, models of clonal evolution could be observed closely in patients with AML.
We were able to monitor molecular changes within our patient’s predominant clonal populations by repeating peripheral comprehensive NGS panels after lines of targeted therapies. The repeated sequencing revealed that clones with FLT3-TKD mutations responded to midostaurin with first-line chemotherapy whereas it was unclear whether clones with IDH1 mutation responded to ivosidenib. Development of complex cytogenetic findings along with the clonal expansion of BCOR mutation-harboring cells likely contributed to our patient’s acutely worsening condition. Several studies have found that the presence of a BCOR mutation in adults with AML leads to lower overall survival and relapse-free survival.11,12 As of now, there are no treatments specifically targeting BCOR mutations.
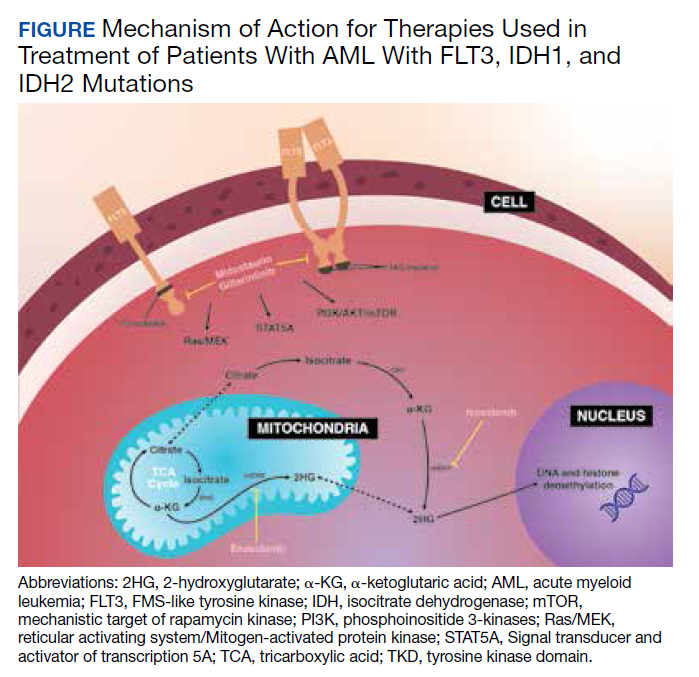
Although there are novel targeting agents with proven efficacy for both FLT3 and IDH1 mutations (Figure), it is difficult to determine which pathogenic mutation drives disease onset. No evidence suggests that these drugs could be administered in tandem. At the present time, interest is directed towards targeting all AML subclones simultaneously, which could reduce the likelihood of evolution among founder clones.7,10,13 In their comparison between molecular profiles and outcomes of patients with AML, Papaemmanuil and colleagues observed that > 80% of patients with AML harbor ≥ 2 driver mutations concurrently.14 Moreover, FLT3-ITD and IDH1 mutations tend to co-occur in approximately 9 to 27% of AML cases.15-18 Available targeted agents for AML are relatively new and hematologists’ familiarity with these drugs is continuing to grow. As the number of novel agents increases, investigations directed toward assessing the safety profile and efficacy of combining targeted agents will be beneficial for patients with AML with ≥ 1 driver mutation.
Conclusions
For our patient with AML, sequential targeted management of FLT3-TKD and IDH1 mutations was not beneficial. Higher-risk disease features, such as the development of a complex karyotype, likely contributed to our patient’s poor response to second-line ivosidenib. The sequential NGS malignant hematology panels allowed us to closely monitor changes to the molecular structure of our patient’s AML after each line of targeted therapy. Future investigations of combining targeted agents for patients with AML with concurrent actionable mutations would provide insight into outcomes of treating multiple clonal populations simultaneously.
1. De Kouchkovsky I, Abdul-Hay M. Acute myeloid leukemia: a comprehensive review and 2016 update. Blood Cancer J. 2016;6(7):e441. doi:10.1038/bcj.2016.50.
2. National Cancer Institute. Cancer Stat Facts: Leukemia — acute myeloid leukemia (AML). Accessed November 4, 2020. https://seer.cancer.gov/statfacts/html/amyl.html
3. Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus chemotherapy for acute myeloid leukemia with a FLT3 mutation. N Engl J Med. 2017;377(5):454-464. doi:10.1056/NEJMoa1614359.
4. DiNardo CD, Stein EM, de Botton S, et al. Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med. 2018;378(25):2386-2398. doi:10.1056/NEJMoa1716984.
5. Roboz, GJ, DiNardo, CD, Stein, EM, et al. Ivosidenib induces deep durable remissions in patients with newly diagnosed IDH1-mutant acute myeloid leukemia. Blood. 2019;135(7), 463-471. doi: 10.1182/blood.2019002140
6. Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722-731. doi:10.1182/blood-2017-04-779405.
7. Jan M, Majeti R. Clonal evolution of acute leukemia genomes. Oncogene. 2013;32(2):135-140. doi:10.1038/onc.2012.48.
8. Grove CS, Vassiliou GS. Acute myeloid leukaemia: a paradigm for the clonal evolution of cancer? Dis Model Mech. 2014;7(8):941-951. doi:10.1242/dmm.015974.
9. Anderson K, Lutz C, van Delft FW, et al. Genetic variegation of clonal architecture and propagating cells in leukaemia. Nature. 2011;469(7330):356-561. doi: 10.1038/nature09650.
10. Ding L, Ley TJ, Larson DE, et al. Clonal evolution in relapsed acute myeloid leukaemia revealed by whole-genome sequencing. Nature. 2012;481(7382):506-510. doi:10.1038/nature10738.
11. Terada K, Yamaguchi H, Ueki T, et al. Usefulness of BCOR gene mutation as a prognostic factor in acute myeloid leukemia with intermediate cytogenetic prognosis. Genes Chromosomes Cancer. 2018;57(8):401-408. doi:10.1002/gcc.22542.
12. Grossmann V, Tiacci E, Holmes AB, et al. Whole-exome sequencing identifies somatic mutations of BCOR in acute myeloid leukemia with normal karyotype. Blood. 2011;118(23):6153-6163. doi:10.1182/blood-2011-07-365320.
13. Parkin B, Ouillette P, Li Y, et al. Clonal evolution and devolution after chemotherapy in adult acute myelogenous leukemia. Blood. 2013;121(2):369-377. doi:10.1182/blood-2012-04-427039.
14. Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic classification and prognosis in acute myeloid leukemia. N Engl J Med. 2016;374(23):2209-2221. doi:10.1056/NEJMoa1516192.
15. DiNardo CD, Ravandi F, Agresta S, et al. Characteristics, clinical outcome, and prognostic significance of IDH mutations in AML. Am J Hematol. 2015;90(8):732-736. doi:10.1002/ajh.24072.
16. Rakheja D, Konoplev S, Medeiros LJ, Chen W. IDH mutations in acute myeloid leukemia. Hum Pathol. 2012;43 (10):1541-1551. doi:10.1016/j.humpath.2012.05.003.
17. Lai C, Doucette K, Norsworthy K. Recent drug approvals for acute myeloid leukemia. J H Oncol. 2019;12(1):100. doi:10.1186/s13045-019-0774-x.
18. Boddu P, Takahashi K, Pemmaraju N, et al. Influence of IDH on FLT3-ITD status in newly diagnosed AML. Leukemia. 2017;31(11):2526-2529. doi:10.1038/leu.2017.244.
Nearly 20,000 patients are diagnosed with acute myeloid leukemia (AML) in the US annually.1 Despite the use of aggressive chemotherapeutic agents, the prognosis remains poor, with a mean 5-year survival of 28.3%.2 Fortunately, with the refinement of next-generation sequencing (NGS) hematology panels and development of systemic targeted therapies, the treatment landscape for eligible patients has improved, both in frontline and relapsed or refractory (R/R) patients.
Specifically, investigations into alterations within the FMS-like tyrosine kinase (FLT3) and isocitrate dehydrogenase (IDH) genes have led to the discovery of a number of targeted treatments. Midostaurin is US Food and Drug Administration (FDA)-approved for use in combination with induction chemotherapy for patients with internal tandem duplication of the FLT3 (FLT3-ITD) gene or mutations within the tyrosine kinase domain (FLT3-TKD).3 Ivosidenib is indicated for frontline treatment for those who are poor candidates for induction chemotherapy, and R/R patients who have an R132H mutation in IDH1.4,5 Enasidenib is FDA-approved for R/R patients with R140Q, R172S, and R172K mutations in IDH2.6
The optimal treatment for patients with AML with ≥ 2 clinically actionable mutations has not been established. In this article we describe a geriatric patient who initially was diagnosed with AML with concurrent FLT3-TKD and IDH1 mutations and received targeted, sequential management. We detail changes in disease phenotype and mutational status by repeating an NGS hematology panel and cytogenetic studies after each stage of therapy. Lastly, we discuss the clonal evolution apparent within leukemic cells with use of ≥ 1 or more targeted agents.
Case Presentation
A 68-year-old man presented to the Emergency Department at The Durham Veterans Affairs Medical Center in North Carolina with fatigue and light-headedness. Because of his symptoms and pancytopenia, a bone marrow aspiration and trephine biopsy were performed, which showed 57% myeloblasts, 12% promyelocytes/myelocytes, and 2% metamyelocytes in 20 to 30% cellular bone marrow. Flow cytometry confirmed a blast population consistent with AML. A LeukoVantage (Quest Diagnostics) hematologic NGS panel revealed the presence of FLT3-TKD, IDH1, RUNX1, BCOR-E1477, and SF3B1 mutations (Table). Initial fluorescence in situ hybridization (FISH) results showed a normal pattern of hybridization with no translocations. His disease was deemed to be intermediate-high risk because of the presence of FLT3-TKD and RUNX1 mutations, despite the normal cytogenetic profile and absence of additional clinical features.
Induction chemotherapy was started with idarubicin, 12 mg/m2, on days 1 to 3 and cytarabine, 200 mg/m2, on days 1 to 7. Because of the presence of a FLT3-TKD mutation, midostaurin was planned for days 8 to 21. After induction chemotherapy, a bone marrow biopsy on day 14 revealed an acellular marrow with no observed myeloblasts. A bone marrow biopsy conducted before initiating consolidation therapy, revealed 30% cellularity with morphologic remission. However, flow cytometry found 5% myeloblasts expressing CD34, CD117, CD13, CD38, and HLA-DR, consistent with measurable residual disease. He received 2 cycles of consolidation therapy with high-dose cytarabine combined with midostaurin. After the patient's second cycle of consolidation, he continued to experience transfusion-dependent cytopenias. Another bone marrow evaluation demonstrated 10% cellularity with nearly all cells appearing to be myeloblasts. A repeat LeukoVantage NGS panel demonstrated undetectable FLT3-TKD mutation and persistent IDH1-R123C mutation. FISH studies revealed a complex karyotype with monosomy of chromosomes 5 and 7 and trisomy of chromosome 8.
We discussed with the patient and his family the options available, which included initiating targeted therapy for his IDH1 mutation, administering hypomethylation therapy with or without venetoclax, or pursuing palliative measures. We collectively decided to pursue therapy with single-agent oral ivosidenib, 500 mg daily. After 1 month of treatment, our patient developed worsening fatigue. His white blood cell count had increased to > 43 k/cm2, raising concern for differentiation syndrome.
A review of the peripheral smear showed a wide-spectrum of maturing granulocytes, with a large percentage of blasts. Peripheral flow cytometry confirmed a blast population of 15%. After a short period of symptom improvement with steroids, the patient developed worsening confusion. Brain imaging identified 2 subdural hemorrhages. Because of a significant peripheral blast population and the development of these hemorrhages, palliative measures were pursued, and the patient was discharged to an inpatient hospice facility. A final NGS panel performed from peripheral blood detected mutations in IDH1, RUNX1, PTPN11, NRAS, BCOR-E1443, and SF3B1 genes.
Discussion
To our knowledge, this is the first reported case of a patient who sequentially received targeted treatments directed against both FLT3 and IDH1 mutations. Initial management with midostaurin and cytarabine resulted in sustained remission of his FLT3-TKD mutation. However, despite receiving prompt standard of care with combination induction chemotherapy and targeted therapy, the patient experienced unfavorable clonal evolution based upon his molecular and cytogenetic testing. Addition of ivosidenib as a second targeting agent for his IDH1 mutation did not achieve a second remission.
Clonal evolution is a well-described phenomenon in hematology. Indolent conditions, such as clonal hematopoiesis of intermediate potential, or malignancies, such as myelodysplastic syndromes and myeloproliferative neoplasms, could transform into acute leukemia through the accumulation of driver mutations and/or cytogenetic abnormalities. Clonal evolution often is viewed as the culprit in patients with AML whose disease relapses after remission with initial chemotherapy.7-10 With the increasing availability of commercial NGS panels designed to assess mutations among patients experiencing hematologic malignancies, patterns of relapse, and, models of clonal evolution could be observed closely in patients with AML.
We were able to monitor molecular changes within our patient’s predominant clonal populations by repeating peripheral comprehensive NGS panels after lines of targeted therapies. The repeated sequencing revealed that clones with FLT3-TKD mutations responded to midostaurin with first-line chemotherapy whereas it was unclear whether clones with IDH1 mutation responded to ivosidenib. Development of complex cytogenetic findings along with the clonal expansion of BCOR mutation-harboring cells likely contributed to our patient’s acutely worsening condition. Several studies have found that the presence of a BCOR mutation in adults with AML leads to lower overall survival and relapse-free survival.11,12 As of now, there are no treatments specifically targeting BCOR mutations.
Although there are novel targeting agents with proven efficacy for both FLT3 and IDH1 mutations (Figure), it is difficult to determine which pathogenic mutation drives disease onset. No evidence suggests that these drugs could be administered in tandem. At the present time, interest is directed towards targeting all AML subclones simultaneously, which could reduce the likelihood of evolution among founder clones.7,10,13 In their comparison between molecular profiles and outcomes of patients with AML, Papaemmanuil and colleagues observed that > 80% of patients with AML harbor ≥ 2 driver mutations concurrently.14 Moreover, FLT3-ITD and IDH1 mutations tend to co-occur in approximately 9 to 27% of AML cases.15-18 Available targeted agents for AML are relatively new and hematologists’ familiarity with these drugs is continuing to grow. As the number of novel agents increases, investigations directed toward assessing the safety profile and efficacy of combining targeted agents will be beneficial for patients with AML with ≥ 1 driver mutation.
Conclusions
For our patient with AML, sequential targeted management of FLT3-TKD and IDH1 mutations was not beneficial. Higher-risk disease features, such as the development of a complex karyotype, likely contributed to our patient’s poor response to second-line ivosidenib. The sequential NGS malignant hematology panels allowed us to closely monitor changes to the molecular structure of our patient’s AML after each line of targeted therapy. Future investigations of combining targeted agents for patients with AML with concurrent actionable mutations would provide insight into outcomes of treating multiple clonal populations simultaneously.
Nearly 20,000 patients are diagnosed with acute myeloid leukemia (AML) in the US annually.1 Despite the use of aggressive chemotherapeutic agents, the prognosis remains poor, with a mean 5-year survival of 28.3%.2 Fortunately, with the refinement of next-generation sequencing (NGS) hematology panels and development of systemic targeted therapies, the treatment landscape for eligible patients has improved, both in frontline and relapsed or refractory (R/R) patients.
Specifically, investigations into alterations within the FMS-like tyrosine kinase (FLT3) and isocitrate dehydrogenase (IDH) genes have led to the discovery of a number of targeted treatments. Midostaurin is US Food and Drug Administration (FDA)-approved for use in combination with induction chemotherapy for patients with internal tandem duplication of the FLT3 (FLT3-ITD) gene or mutations within the tyrosine kinase domain (FLT3-TKD).3 Ivosidenib is indicated for frontline treatment for those who are poor candidates for induction chemotherapy, and R/R patients who have an R132H mutation in IDH1.4,5 Enasidenib is FDA-approved for R/R patients with R140Q, R172S, and R172K mutations in IDH2.6
The optimal treatment for patients with AML with ≥ 2 clinically actionable mutations has not been established. In this article we describe a geriatric patient who initially was diagnosed with AML with concurrent FLT3-TKD and IDH1 mutations and received targeted, sequential management. We detail changes in disease phenotype and mutational status by repeating an NGS hematology panel and cytogenetic studies after each stage of therapy. Lastly, we discuss the clonal evolution apparent within leukemic cells with use of ≥ 1 or more targeted agents.
Case Presentation
A 68-year-old man presented to the Emergency Department at The Durham Veterans Affairs Medical Center in North Carolina with fatigue and light-headedness. Because of his symptoms and pancytopenia, a bone marrow aspiration and trephine biopsy were performed, which showed 57% myeloblasts, 12% promyelocytes/myelocytes, and 2% metamyelocytes in 20 to 30% cellular bone marrow. Flow cytometry confirmed a blast population consistent with AML. A LeukoVantage (Quest Diagnostics) hematologic NGS panel revealed the presence of FLT3-TKD, IDH1, RUNX1, BCOR-E1477, and SF3B1 mutations (Table). Initial fluorescence in situ hybridization (FISH) results showed a normal pattern of hybridization with no translocations. His disease was deemed to be intermediate-high risk because of the presence of FLT3-TKD and RUNX1 mutations, despite the normal cytogenetic profile and absence of additional clinical features.
Induction chemotherapy was started with idarubicin, 12 mg/m2, on days 1 to 3 and cytarabine, 200 mg/m2, on days 1 to 7. Because of the presence of a FLT3-TKD mutation, midostaurin was planned for days 8 to 21. After induction chemotherapy, a bone marrow biopsy on day 14 revealed an acellular marrow with no observed myeloblasts. A bone marrow biopsy conducted before initiating consolidation therapy, revealed 30% cellularity with morphologic remission. However, flow cytometry found 5% myeloblasts expressing CD34, CD117, CD13, CD38, and HLA-DR, consistent with measurable residual disease. He received 2 cycles of consolidation therapy with high-dose cytarabine combined with midostaurin. After the patient's second cycle of consolidation, he continued to experience transfusion-dependent cytopenias. Another bone marrow evaluation demonstrated 10% cellularity with nearly all cells appearing to be myeloblasts. A repeat LeukoVantage NGS panel demonstrated undetectable FLT3-TKD mutation and persistent IDH1-R123C mutation. FISH studies revealed a complex karyotype with monosomy of chromosomes 5 and 7 and trisomy of chromosome 8.
We discussed with the patient and his family the options available, which included initiating targeted therapy for his IDH1 mutation, administering hypomethylation therapy with or without venetoclax, or pursuing palliative measures. We collectively decided to pursue therapy with single-agent oral ivosidenib, 500 mg daily. After 1 month of treatment, our patient developed worsening fatigue. His white blood cell count had increased to > 43 k/cm2, raising concern for differentiation syndrome.
A review of the peripheral smear showed a wide-spectrum of maturing granulocytes, with a large percentage of blasts. Peripheral flow cytometry confirmed a blast population of 15%. After a short period of symptom improvement with steroids, the patient developed worsening confusion. Brain imaging identified 2 subdural hemorrhages. Because of a significant peripheral blast population and the development of these hemorrhages, palliative measures were pursued, and the patient was discharged to an inpatient hospice facility. A final NGS panel performed from peripheral blood detected mutations in IDH1, RUNX1, PTPN11, NRAS, BCOR-E1443, and SF3B1 genes.
Discussion
To our knowledge, this is the first reported case of a patient who sequentially received targeted treatments directed against both FLT3 and IDH1 mutations. Initial management with midostaurin and cytarabine resulted in sustained remission of his FLT3-TKD mutation. However, despite receiving prompt standard of care with combination induction chemotherapy and targeted therapy, the patient experienced unfavorable clonal evolution based upon his molecular and cytogenetic testing. Addition of ivosidenib as a second targeting agent for his IDH1 mutation did not achieve a second remission.
Clonal evolution is a well-described phenomenon in hematology. Indolent conditions, such as clonal hematopoiesis of intermediate potential, or malignancies, such as myelodysplastic syndromes and myeloproliferative neoplasms, could transform into acute leukemia through the accumulation of driver mutations and/or cytogenetic abnormalities. Clonal evolution often is viewed as the culprit in patients with AML whose disease relapses after remission with initial chemotherapy.7-10 With the increasing availability of commercial NGS panels designed to assess mutations among patients experiencing hematologic malignancies, patterns of relapse, and, models of clonal evolution could be observed closely in patients with AML.
We were able to monitor molecular changes within our patient’s predominant clonal populations by repeating peripheral comprehensive NGS panels after lines of targeted therapies. The repeated sequencing revealed that clones with FLT3-TKD mutations responded to midostaurin with first-line chemotherapy whereas it was unclear whether clones with IDH1 mutation responded to ivosidenib. Development of complex cytogenetic findings along with the clonal expansion of BCOR mutation-harboring cells likely contributed to our patient’s acutely worsening condition. Several studies have found that the presence of a BCOR mutation in adults with AML leads to lower overall survival and relapse-free survival.11,12 As of now, there are no treatments specifically targeting BCOR mutations.
Although there are novel targeting agents with proven efficacy for both FLT3 and IDH1 mutations (Figure), it is difficult to determine which pathogenic mutation drives disease onset. No evidence suggests that these drugs could be administered in tandem. At the present time, interest is directed towards targeting all AML subclones simultaneously, which could reduce the likelihood of evolution among founder clones.7,10,13 In their comparison between molecular profiles and outcomes of patients with AML, Papaemmanuil and colleagues observed that > 80% of patients with AML harbor ≥ 2 driver mutations concurrently.14 Moreover, FLT3-ITD and IDH1 mutations tend to co-occur in approximately 9 to 27% of AML cases.15-18 Available targeted agents for AML are relatively new and hematologists’ familiarity with these drugs is continuing to grow. As the number of novel agents increases, investigations directed toward assessing the safety profile and efficacy of combining targeted agents will be beneficial for patients with AML with ≥ 1 driver mutation.
Conclusions
For our patient with AML, sequential targeted management of FLT3-TKD and IDH1 mutations was not beneficial. Higher-risk disease features, such as the development of a complex karyotype, likely contributed to our patient’s poor response to second-line ivosidenib. The sequential NGS malignant hematology panels allowed us to closely monitor changes to the molecular structure of our patient’s AML after each line of targeted therapy. Future investigations of combining targeted agents for patients with AML with concurrent actionable mutations would provide insight into outcomes of treating multiple clonal populations simultaneously.
1. De Kouchkovsky I, Abdul-Hay M. Acute myeloid leukemia: a comprehensive review and 2016 update. Blood Cancer J. 2016;6(7):e441. doi:10.1038/bcj.2016.50.
2. National Cancer Institute. Cancer Stat Facts: Leukemia — acute myeloid leukemia (AML). Accessed November 4, 2020. https://seer.cancer.gov/statfacts/html/amyl.html
3. Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus chemotherapy for acute myeloid leukemia with a FLT3 mutation. N Engl J Med. 2017;377(5):454-464. doi:10.1056/NEJMoa1614359.
4. DiNardo CD, Stein EM, de Botton S, et al. Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med. 2018;378(25):2386-2398. doi:10.1056/NEJMoa1716984.
5. Roboz, GJ, DiNardo, CD, Stein, EM, et al. Ivosidenib induces deep durable remissions in patients with newly diagnosed IDH1-mutant acute myeloid leukemia. Blood. 2019;135(7), 463-471. doi: 10.1182/blood.2019002140
6. Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722-731. doi:10.1182/blood-2017-04-779405.
7. Jan M, Majeti R. Clonal evolution of acute leukemia genomes. Oncogene. 2013;32(2):135-140. doi:10.1038/onc.2012.48.
8. Grove CS, Vassiliou GS. Acute myeloid leukaemia: a paradigm for the clonal evolution of cancer? Dis Model Mech. 2014;7(8):941-951. doi:10.1242/dmm.015974.
9. Anderson K, Lutz C, van Delft FW, et al. Genetic variegation of clonal architecture and propagating cells in leukaemia. Nature. 2011;469(7330):356-561. doi: 10.1038/nature09650.
10. Ding L, Ley TJ, Larson DE, et al. Clonal evolution in relapsed acute myeloid leukaemia revealed by whole-genome sequencing. Nature. 2012;481(7382):506-510. doi:10.1038/nature10738.
11. Terada K, Yamaguchi H, Ueki T, et al. Usefulness of BCOR gene mutation as a prognostic factor in acute myeloid leukemia with intermediate cytogenetic prognosis. Genes Chromosomes Cancer. 2018;57(8):401-408. doi:10.1002/gcc.22542.
12. Grossmann V, Tiacci E, Holmes AB, et al. Whole-exome sequencing identifies somatic mutations of BCOR in acute myeloid leukemia with normal karyotype. Blood. 2011;118(23):6153-6163. doi:10.1182/blood-2011-07-365320.
13. Parkin B, Ouillette P, Li Y, et al. Clonal evolution and devolution after chemotherapy in adult acute myelogenous leukemia. Blood. 2013;121(2):369-377. doi:10.1182/blood-2012-04-427039.
14. Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic classification and prognosis in acute myeloid leukemia. N Engl J Med. 2016;374(23):2209-2221. doi:10.1056/NEJMoa1516192.
15. DiNardo CD, Ravandi F, Agresta S, et al. Characteristics, clinical outcome, and prognostic significance of IDH mutations in AML. Am J Hematol. 2015;90(8):732-736. doi:10.1002/ajh.24072.
16. Rakheja D, Konoplev S, Medeiros LJ, Chen W. IDH mutations in acute myeloid leukemia. Hum Pathol. 2012;43 (10):1541-1551. doi:10.1016/j.humpath.2012.05.003.
17. Lai C, Doucette K, Norsworthy K. Recent drug approvals for acute myeloid leukemia. J H Oncol. 2019;12(1):100. doi:10.1186/s13045-019-0774-x.
18. Boddu P, Takahashi K, Pemmaraju N, et al. Influence of IDH on FLT3-ITD status in newly diagnosed AML. Leukemia. 2017;31(11):2526-2529. doi:10.1038/leu.2017.244.
1. De Kouchkovsky I, Abdul-Hay M. Acute myeloid leukemia: a comprehensive review and 2016 update. Blood Cancer J. 2016;6(7):e441. doi:10.1038/bcj.2016.50.
2. National Cancer Institute. Cancer Stat Facts: Leukemia — acute myeloid leukemia (AML). Accessed November 4, 2020. https://seer.cancer.gov/statfacts/html/amyl.html
3. Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus chemotherapy for acute myeloid leukemia with a FLT3 mutation. N Engl J Med. 2017;377(5):454-464. doi:10.1056/NEJMoa1614359.
4. DiNardo CD, Stein EM, de Botton S, et al. Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med. 2018;378(25):2386-2398. doi:10.1056/NEJMoa1716984.
5. Roboz, GJ, DiNardo, CD, Stein, EM, et al. Ivosidenib induces deep durable remissions in patients with newly diagnosed IDH1-mutant acute myeloid leukemia. Blood. 2019;135(7), 463-471. doi: 10.1182/blood.2019002140
6. Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood. 2017;130(6):722-731. doi:10.1182/blood-2017-04-779405.
7. Jan M, Majeti R. Clonal evolution of acute leukemia genomes. Oncogene. 2013;32(2):135-140. doi:10.1038/onc.2012.48.
8. Grove CS, Vassiliou GS. Acute myeloid leukaemia: a paradigm for the clonal evolution of cancer? Dis Model Mech. 2014;7(8):941-951. doi:10.1242/dmm.015974.
9. Anderson K, Lutz C, van Delft FW, et al. Genetic variegation of clonal architecture and propagating cells in leukaemia. Nature. 2011;469(7330):356-561. doi: 10.1038/nature09650.
10. Ding L, Ley TJ, Larson DE, et al. Clonal evolution in relapsed acute myeloid leukaemia revealed by whole-genome sequencing. Nature. 2012;481(7382):506-510. doi:10.1038/nature10738.
11. Terada K, Yamaguchi H, Ueki T, et al. Usefulness of BCOR gene mutation as a prognostic factor in acute myeloid leukemia with intermediate cytogenetic prognosis. Genes Chromosomes Cancer. 2018;57(8):401-408. doi:10.1002/gcc.22542.
12. Grossmann V, Tiacci E, Holmes AB, et al. Whole-exome sequencing identifies somatic mutations of BCOR in acute myeloid leukemia with normal karyotype. Blood. 2011;118(23):6153-6163. doi:10.1182/blood-2011-07-365320.
13. Parkin B, Ouillette P, Li Y, et al. Clonal evolution and devolution after chemotherapy in adult acute myelogenous leukemia. Blood. 2013;121(2):369-377. doi:10.1182/blood-2012-04-427039.
14. Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic classification and prognosis in acute myeloid leukemia. N Engl J Med. 2016;374(23):2209-2221. doi:10.1056/NEJMoa1516192.
15. DiNardo CD, Ravandi F, Agresta S, et al. Characteristics, clinical outcome, and prognostic significance of IDH mutations in AML. Am J Hematol. 2015;90(8):732-736. doi:10.1002/ajh.24072.
16. Rakheja D, Konoplev S, Medeiros LJ, Chen W. IDH mutations in acute myeloid leukemia. Hum Pathol. 2012;43 (10):1541-1551. doi:10.1016/j.humpath.2012.05.003.
17. Lai C, Doucette K, Norsworthy K. Recent drug approvals for acute myeloid leukemia. J H Oncol. 2019;12(1):100. doi:10.1186/s13045-019-0774-x.
18. Boddu P, Takahashi K, Pemmaraju N, et al. Influence of IDH on FLT3-ITD status in newly diagnosed AML. Leukemia. 2017;31(11):2526-2529. doi:10.1038/leu.2017.244.
U.S. mothers underestimate role breastfeeding plays in curbing breast cancer
The majority of women in the United States remain unaware of the benefits breastfeeding offers in reducing the risk of breast cancer, reported Adrienne Hoyt-Austin, DO, and colleagues at University of California, Davis.

Using nationally representative data collected from the 2015-2017 National Survey of Family Growth, Dr. Hoyt-Austin and colleagues analyzed responses to the question: “Do you think that breastfeeding decreases a woman’s chances of getting breast cancer a lot, a little, or not at all, no opinion, or don’t know?” A total of 5,554 female respondents aged 15-49 years participated. The response rate was 66.7%.
Multiparous status and education play a role in decreased awareness
Those who had given birth more than once, who had no more than a high school education, or who were U.S.-born Hispanic had the lowest level of awareness, believing that breastfeeding offers only “a little” protection. Of those who were aware of the link, 44% reported that breastfeeding provides “a lot” of protection, and foreign-born participants as well as those who breastfed for more than a year were more likely to conclude that breastfeeding offers “a lot” of protection. The researchers found that neither mammogram or personal family history of breast cancer had any bearing on awareness.
Although multiple studies have found breastfeeding to confer a lower rate of cancer risk, morbidity and mortality, with a 26% lower lifetime risk for those mothers who breastfeed for 12 months or longer, only 36% of women in the United States actually breastfeed.
Limited data indicate whether respondents were breastfed themselves
“Public health initiatives must consider the complex roots of disparities in breastfeeding,” noted Dr. Hoyt-Austin and colleagues. They acknowledged the subjectivity of perceptions of “a lot” versus “a little” and noted that the study was limited by a lack of data on whether participants were breastfed themselves.
Clinicians have an opportunity to play a key role in better educating families concerning the benefits of breastfeeding, both for mother and child, they advised. According to one recent study, just 5 minutes of counseling on the benefits of breastfeeding “significantly strengthened women’s intentions to breastfeed.
In a separate interview, Amy E. Cyr, MD, FACS, section of surgical oncology at Washington University, St. Louis, noted that “many breast cancer risk factors – age, sex, family history, and age of menopause – are nonmodifiable.” And while other risk factors, including alcohol use, diet, and exercise are controllable, “pregnancies and breastfeeding don’t always go as planned,” Dr. Cyr added.
“Although Dr. Hoyt-Austin et al. observed that many women aren’t aware that breastfeeding decreases breast cancer risk – or to what extent (they cite a 26% cancer risk reduction after 12 or more months of breastfeeding) – most studies haven’t shown that large a drop in breast cancer risk,“ she pointed out, adding that “I think it’s an overstatement to suggest that breastfeeding reduces cancer risk by ‘a lot,’ as one of the survey choices offered in the study suggests.”
Whether or not a woman breastfeeds depends not only on desire but on social and economic support and biology; for some, breastfeeding simply isn’t an option. “I agree that we should educate women about the benefits of breastfeeding so they can make an informed decision for themselves and their infants, but we also need to acknowledge the complexity of this issue,” she cautioned.
One coauthor reported a travel stipend by the Human Milk Banking Association of North America; Dr. Hoyt-Austin and the other authors had no conflicts of interest to report. Dr. Cyr had no conflicts of interest to report.
SOURCE: Hoyt-Austin A et al. Obstet Gynecol. 2020 Dec. doi: 10.1097/AOG.0000000000004162.
The majority of women in the United States remain unaware of the benefits breastfeeding offers in reducing the risk of breast cancer, reported Adrienne Hoyt-Austin, DO, and colleagues at University of California, Davis.
Using nationally representative data collected from the 2015-2017 National Survey of Family Growth, Dr. Hoyt-Austin and colleagues analyzed responses to the question: “Do you think that breastfeeding decreases a woman’s chances of getting breast cancer a lot, a little, or not at all, no opinion, or don’t know?” A total of 5,554 female respondents aged 15-49 years participated. The response rate was 66.7%.
Multiparous status and education play a role in decreased awareness
Those who had given birth more than once, who had no more than a high school education, or who were U.S.-born Hispanic had the lowest level of awareness, believing that breastfeeding offers only “a little” protection. Of those who were aware of the link, 44% reported that breastfeeding provides “a lot” of protection, and foreign-born participants as well as those who breastfed for more than a year were more likely to conclude that breastfeeding offers “a lot” of protection. The researchers found that neither mammogram or personal family history of breast cancer had any bearing on awareness.
Although multiple studies have found breastfeeding to confer a lower rate of cancer risk, morbidity and mortality, with a 26% lower lifetime risk for those mothers who breastfeed for 12 months or longer, only 36% of women in the United States actually breastfeed.
Limited data indicate whether respondents were breastfed themselves
“Public health initiatives must consider the complex roots of disparities in breastfeeding,” noted Dr. Hoyt-Austin and colleagues. They acknowledged the subjectivity of perceptions of “a lot” versus “a little” and noted that the study was limited by a lack of data on whether participants were breastfed themselves.
Clinicians have an opportunity to play a key role in better educating families concerning the benefits of breastfeeding, both for mother and child, they advised. According to one recent study, just 5 minutes of counseling on the benefits of breastfeeding “significantly strengthened women’s intentions to breastfeed.
In a separate interview, Amy E. Cyr, MD, FACS, section of surgical oncology at Washington University, St. Louis, noted that “many breast cancer risk factors – age, sex, family history, and age of menopause – are nonmodifiable.” And while other risk factors, including alcohol use, diet, and exercise are controllable, “pregnancies and breastfeeding don’t always go as planned,” Dr. Cyr added.
“Although Dr. Hoyt-Austin et al. observed that many women aren’t aware that breastfeeding decreases breast cancer risk – or to what extent (they cite a 26% cancer risk reduction after 12 or more months of breastfeeding) – most studies haven’t shown that large a drop in breast cancer risk,“ she pointed out, adding that “I think it’s an overstatement to suggest that breastfeeding reduces cancer risk by ‘a lot,’ as one of the survey choices offered in the study suggests.”
Whether or not a woman breastfeeds depends not only on desire but on social and economic support and biology; for some, breastfeeding simply isn’t an option. “I agree that we should educate women about the benefits of breastfeeding so they can make an informed decision for themselves and their infants, but we also need to acknowledge the complexity of this issue,” she cautioned.
One coauthor reported a travel stipend by the Human Milk Banking Association of North America; Dr. Hoyt-Austin and the other authors had no conflicts of interest to report. Dr. Cyr had no conflicts of interest to report.
SOURCE: Hoyt-Austin A et al. Obstet Gynecol. 2020 Dec. doi: 10.1097/AOG.0000000000004162.
The majority of women in the United States remain unaware of the benefits breastfeeding offers in reducing the risk of breast cancer, reported Adrienne Hoyt-Austin, DO, and colleagues at University of California, Davis.
Using nationally representative data collected from the 2015-2017 National Survey of Family Growth, Dr. Hoyt-Austin and colleagues analyzed responses to the question: “Do you think that breastfeeding decreases a woman’s chances of getting breast cancer a lot, a little, or not at all, no opinion, or don’t know?” A total of 5,554 female respondents aged 15-49 years participated. The response rate was 66.7%.
Multiparous status and education play a role in decreased awareness
Those who had given birth more than once, who had no more than a high school education, or who were U.S.-born Hispanic had the lowest level of awareness, believing that breastfeeding offers only “a little” protection. Of those who were aware of the link, 44% reported that breastfeeding provides “a lot” of protection, and foreign-born participants as well as those who breastfed for more than a year were more likely to conclude that breastfeeding offers “a lot” of protection. The researchers found that neither mammogram or personal family history of breast cancer had any bearing on awareness.
Although multiple studies have found breastfeeding to confer a lower rate of cancer risk, morbidity and mortality, with a 26% lower lifetime risk for those mothers who breastfeed for 12 months or longer, only 36% of women in the United States actually breastfeed.
Limited data indicate whether respondents were breastfed themselves
“Public health initiatives must consider the complex roots of disparities in breastfeeding,” noted Dr. Hoyt-Austin and colleagues. They acknowledged the subjectivity of perceptions of “a lot” versus “a little” and noted that the study was limited by a lack of data on whether participants were breastfed themselves.
Clinicians have an opportunity to play a key role in better educating families concerning the benefits of breastfeeding, both for mother and child, they advised. According to one recent study, just 5 minutes of counseling on the benefits of breastfeeding “significantly strengthened women’s intentions to breastfeed.
In a separate interview, Amy E. Cyr, MD, FACS, section of surgical oncology at Washington University, St. Louis, noted that “many breast cancer risk factors – age, sex, family history, and age of menopause – are nonmodifiable.” And while other risk factors, including alcohol use, diet, and exercise are controllable, “pregnancies and breastfeeding don’t always go as planned,” Dr. Cyr added.
“Although Dr. Hoyt-Austin et al. observed that many women aren’t aware that breastfeeding decreases breast cancer risk – or to what extent (they cite a 26% cancer risk reduction after 12 or more months of breastfeeding) – most studies haven’t shown that large a drop in breast cancer risk,“ she pointed out, adding that “I think it’s an overstatement to suggest that breastfeeding reduces cancer risk by ‘a lot,’ as one of the survey choices offered in the study suggests.”
Whether or not a woman breastfeeds depends not only on desire but on social and economic support and biology; for some, breastfeeding simply isn’t an option. “I agree that we should educate women about the benefits of breastfeeding so they can make an informed decision for themselves and their infants, but we also need to acknowledge the complexity of this issue,” she cautioned.
One coauthor reported a travel stipend by the Human Milk Banking Association of North America; Dr. Hoyt-Austin and the other authors had no conflicts of interest to report. Dr. Cyr had no conflicts of interest to report.
SOURCE: Hoyt-Austin A et al. Obstet Gynecol. 2020 Dec. doi: 10.1097/AOG.0000000000004162.
FROM OBSTETRICS & GYNECOLOGY
Which imaging criteria identify progressive forms of MS?
The role of imaging in diagnosing progressive multiple sclerosis (MS) and in assessing prognosis is the subject of a new review.
MRI is central in the diagnostic work-up of patients suspected of having MS, given its high sensitivity in detecting disease dissemination in space and over time and its notable ability to exclude mimics of MS, the authors noted. However, diagnosis of primary progressive MS remains challenging and is only possible retrospectively on the basis of clinical assessment.
they wrote.
Diagnosis of progressive MS is limited by difficulties in distinguishing accumulating disability caused by inflammatory disease activity from that attributable to degenerative processes associated with secondary progressive MS. Moreover, there are no accepted clinical criteria for diagnosing secondary progressive MS, the authors explained.
This need has promoted extensive research in the field of imaging, facilitated by definition of novel MRI sequences, to identify imaging features reflecting pathophysiological mechanisms relevant to the pathobiology of progressive MS, the authors said.
The current review reports the conclusions of a workshop held in Milan in November 2019, at which an expert panel of neurologists and neuroradiologists addressed the role of MRI in progressive MS.
Massimo Filippi, MD, IRCCS San Raffaele Scientific Institute, Milan, was the lead author of the review, which was published online Dec. 14, 2020, in JAMA Neurology.
The authors concluded that no definitive, qualitative clinical, immunologic, histopathologic, or neuroimaging features differentiate primary progressive and secondary progressive forms of MS; both are characterized by neurodegenerative phenomena and a gradual and irreversible accumulation of clinical disability, which is also affected by aging and comorbidities.
A definitive diagnosis of primary progressive MS is more difficult than a diagnosis of relapsing remitting MS; in part, primary progressive MS is a diagnosis of exclusion because it can be mimicked by other conditions clinically and radiologically, the authors noted.
The writers did report that, although nonspecific, some spinal cord imaging features are typical of primary progressive MS. These include diffuse abnormalities and lesions involving gray matter and two or more white-matter columns, but confirmation of this is required.
In patients with primary progressive MS and those with relapse-onset MS, MRI features at disease onset predict long-term disability and a progressive disease course. These features include lesions in critical central nervous system regions (i.e., spinal cord, infratentorial regions, and gray matter) and high inflammatory activity in the first years after disease onset. These measures are evaluable in clinical practice, the authors said.
In patients with established MS, gray-matter involvement and neurodegeneration are associated with accelerated clinical worsening; however, detection validation and standardization need to be implemented at the individual patient level, they commented.
Novel candidate imaging biomarkers, such as subpial demyelination, and the presence of slowly expanding lesions or paramagnetic rim lesions may identify progressive MS but should be further investigated, they added.
Discovery of MRI markers capable of detecting evolution from relapsing-remitting to secondary progressive MS remains an unmet need that will probably require multiparametric MRI studies, because it is unlikely that a single MRI method will be able to allow clinicians to optimally distinguish among these stages, the authors said.
The contribution of these promising MRI measures combined with other biomarkers, such as quantification of serum neurofilament light chain levels or optical coherence tomography assessment, should be explored to improve the identification of patients with progressive MS, they concluded.
‘A comprehensive review’
In a comment, Jeffrey A. Cohen, MD, director of the Cleveland Clinic’s Mellen Center for MS Treatment and Research, said the article is a comprehensive review of the pathologic mechanisms that underlie progression in MS and the proxy measures of those processes (brain and spinal cord MRI, PET, optical coherence tomography, and biomarkers).
“The paper reports there is no qualitative difference between relapsing remitting and progressive MS; rather, the difference is quantitative,” Dr. Cohen noted. “In other words, the processes that underlie progression are present from the earliest stages of MS, becoming more prominent over time.”
The apparent transition to progressive MS, he added, “rather than representing a ‘transition,’ instead results from the accumulation of pathology over time, a shift from focal lesions to diffuse inflammation and damage, and unmasking of the damage due to decreased resiliency due to aging and failure of compensatory mechanisms (neuroplasticity and remyelination).”
Also commenting, Edward Fox, MD, director, MS Clinic of Central Texas and clinical associate professor, University of Texas, Austin, explained that loss of tissue is the main driver of progressive MS.
“We all look at imaging to confirm that the progressive symptoms expressed by the patient are related to demyelinating disease,” he said. “When I see MRI of the spinal cord showing multifocal lesions, especially if localized atrophy is seen in a region of the cord, I expect to hear a history of progressive deficits in gait and other signs of disability.”
Dr. Fox noted that, on MRI of the brain, gray matter atrophy both cortically and in the deep gray structures usually manifests as cognitive slowing and poorer performance in work and social situations.
“We hope that other biomarkers, such as neurofilament light chain, will add to this body of knowledge and give us a better grasp of the definition of neurodegeneration to confirm the clinical and radiographic findings,” he added.
Dr. Filippi has received compensation for consulting services and/or speaking activities from Bayer, Biogen Idec, Merck Serono, Novartis, Roche, Sanofi, Genzyme, Takeda, and Teva Pharmaceutical Industries; and research support from ARiSLA, Biogen Idec, Fondazione Italiana Sclerosi Multipla, Italian Ministry of Health, Merck Serono, Novartis, Roche, and Teva.
A version of this article first appeared on Medscape.com.
The role of imaging in diagnosing progressive multiple sclerosis (MS) and in assessing prognosis is the subject of a new review.
MRI is central in the diagnostic work-up of patients suspected of having MS, given its high sensitivity in detecting disease dissemination in space and over time and its notable ability to exclude mimics of MS, the authors noted. However, diagnosis of primary progressive MS remains challenging and is only possible retrospectively on the basis of clinical assessment.
they wrote.
Diagnosis of progressive MS is limited by difficulties in distinguishing accumulating disability caused by inflammatory disease activity from that attributable to degenerative processes associated with secondary progressive MS. Moreover, there are no accepted clinical criteria for diagnosing secondary progressive MS, the authors explained.
This need has promoted extensive research in the field of imaging, facilitated by definition of novel MRI sequences, to identify imaging features reflecting pathophysiological mechanisms relevant to the pathobiology of progressive MS, the authors said.
The current review reports the conclusions of a workshop held in Milan in November 2019, at which an expert panel of neurologists and neuroradiologists addressed the role of MRI in progressive MS.
Massimo Filippi, MD, IRCCS San Raffaele Scientific Institute, Milan, was the lead author of the review, which was published online Dec. 14, 2020, in JAMA Neurology.
The authors concluded that no definitive, qualitative clinical, immunologic, histopathologic, or neuroimaging features differentiate primary progressive and secondary progressive forms of MS; both are characterized by neurodegenerative phenomena and a gradual and irreversible accumulation of clinical disability, which is also affected by aging and comorbidities.
A definitive diagnosis of primary progressive MS is more difficult than a diagnosis of relapsing remitting MS; in part, primary progressive MS is a diagnosis of exclusion because it can be mimicked by other conditions clinically and radiologically, the authors noted.
The writers did report that, although nonspecific, some spinal cord imaging features are typical of primary progressive MS. These include diffuse abnormalities and lesions involving gray matter and two or more white-matter columns, but confirmation of this is required.
In patients with primary progressive MS and those with relapse-onset MS, MRI features at disease onset predict long-term disability and a progressive disease course. These features include lesions in critical central nervous system regions (i.e., spinal cord, infratentorial regions, and gray matter) and high inflammatory activity in the first years after disease onset. These measures are evaluable in clinical practice, the authors said.
In patients with established MS, gray-matter involvement and neurodegeneration are associated with accelerated clinical worsening; however, detection validation and standardization need to be implemented at the individual patient level, they commented.
Novel candidate imaging biomarkers, such as subpial demyelination, and the presence of slowly expanding lesions or paramagnetic rim lesions may identify progressive MS but should be further investigated, they added.
Discovery of MRI markers capable of detecting evolution from relapsing-remitting to secondary progressive MS remains an unmet need that will probably require multiparametric MRI studies, because it is unlikely that a single MRI method will be able to allow clinicians to optimally distinguish among these stages, the authors said.
The contribution of these promising MRI measures combined with other biomarkers, such as quantification of serum neurofilament light chain levels or optical coherence tomography assessment, should be explored to improve the identification of patients with progressive MS, they concluded.
‘A comprehensive review’
In a comment, Jeffrey A. Cohen, MD, director of the Cleveland Clinic’s Mellen Center for MS Treatment and Research, said the article is a comprehensive review of the pathologic mechanisms that underlie progression in MS and the proxy measures of those processes (brain and spinal cord MRI, PET, optical coherence tomography, and biomarkers).
“The paper reports there is no qualitative difference between relapsing remitting and progressive MS; rather, the difference is quantitative,” Dr. Cohen noted. “In other words, the processes that underlie progression are present from the earliest stages of MS, becoming more prominent over time.”
The apparent transition to progressive MS, he added, “rather than representing a ‘transition,’ instead results from the accumulation of pathology over time, a shift from focal lesions to diffuse inflammation and damage, and unmasking of the damage due to decreased resiliency due to aging and failure of compensatory mechanisms (neuroplasticity and remyelination).”
Also commenting, Edward Fox, MD, director, MS Clinic of Central Texas and clinical associate professor, University of Texas, Austin, explained that loss of tissue is the main driver of progressive MS.
“We all look at imaging to confirm that the progressive symptoms expressed by the patient are related to demyelinating disease,” he said. “When I see MRI of the spinal cord showing multifocal lesions, especially if localized atrophy is seen in a region of the cord, I expect to hear a history of progressive deficits in gait and other signs of disability.”
Dr. Fox noted that, on MRI of the brain, gray matter atrophy both cortically and in the deep gray structures usually manifests as cognitive slowing and poorer performance in work and social situations.
“We hope that other biomarkers, such as neurofilament light chain, will add to this body of knowledge and give us a better grasp of the definition of neurodegeneration to confirm the clinical and radiographic findings,” he added.
Dr. Filippi has received compensation for consulting services and/or speaking activities from Bayer, Biogen Idec, Merck Serono, Novartis, Roche, Sanofi, Genzyme, Takeda, and Teva Pharmaceutical Industries; and research support from ARiSLA, Biogen Idec, Fondazione Italiana Sclerosi Multipla, Italian Ministry of Health, Merck Serono, Novartis, Roche, and Teva.
A version of this article first appeared on Medscape.com.
The role of imaging in diagnosing progressive multiple sclerosis (MS) and in assessing prognosis is the subject of a new review.
MRI is central in the diagnostic work-up of patients suspected of having MS, given its high sensitivity in detecting disease dissemination in space and over time and its notable ability to exclude mimics of MS, the authors noted. However, diagnosis of primary progressive MS remains challenging and is only possible retrospectively on the basis of clinical assessment.
they wrote.
Diagnosis of progressive MS is limited by difficulties in distinguishing accumulating disability caused by inflammatory disease activity from that attributable to degenerative processes associated with secondary progressive MS. Moreover, there are no accepted clinical criteria for diagnosing secondary progressive MS, the authors explained.
This need has promoted extensive research in the field of imaging, facilitated by definition of novel MRI sequences, to identify imaging features reflecting pathophysiological mechanisms relevant to the pathobiology of progressive MS, the authors said.
The current review reports the conclusions of a workshop held in Milan in November 2019, at which an expert panel of neurologists and neuroradiologists addressed the role of MRI in progressive MS.
Massimo Filippi, MD, IRCCS San Raffaele Scientific Institute, Milan, was the lead author of the review, which was published online Dec. 14, 2020, in JAMA Neurology.
The authors concluded that no definitive, qualitative clinical, immunologic, histopathologic, or neuroimaging features differentiate primary progressive and secondary progressive forms of MS; both are characterized by neurodegenerative phenomena and a gradual and irreversible accumulation of clinical disability, which is also affected by aging and comorbidities.
A definitive diagnosis of primary progressive MS is more difficult than a diagnosis of relapsing remitting MS; in part, primary progressive MS is a diagnosis of exclusion because it can be mimicked by other conditions clinically and radiologically, the authors noted.
The writers did report that, although nonspecific, some spinal cord imaging features are typical of primary progressive MS. These include diffuse abnormalities and lesions involving gray matter and two or more white-matter columns, but confirmation of this is required.
In patients with primary progressive MS and those with relapse-onset MS, MRI features at disease onset predict long-term disability and a progressive disease course. These features include lesions in critical central nervous system regions (i.e., spinal cord, infratentorial regions, and gray matter) and high inflammatory activity in the first years after disease onset. These measures are evaluable in clinical practice, the authors said.
In patients with established MS, gray-matter involvement and neurodegeneration are associated with accelerated clinical worsening; however, detection validation and standardization need to be implemented at the individual patient level, they commented.
Novel candidate imaging biomarkers, such as subpial demyelination, and the presence of slowly expanding lesions or paramagnetic rim lesions may identify progressive MS but should be further investigated, they added.
Discovery of MRI markers capable of detecting evolution from relapsing-remitting to secondary progressive MS remains an unmet need that will probably require multiparametric MRI studies, because it is unlikely that a single MRI method will be able to allow clinicians to optimally distinguish among these stages, the authors said.
The contribution of these promising MRI measures combined with other biomarkers, such as quantification of serum neurofilament light chain levels or optical coherence tomography assessment, should be explored to improve the identification of patients with progressive MS, they concluded.
‘A comprehensive review’
In a comment, Jeffrey A. Cohen, MD, director of the Cleveland Clinic’s Mellen Center for MS Treatment and Research, said the article is a comprehensive review of the pathologic mechanisms that underlie progression in MS and the proxy measures of those processes (brain and spinal cord MRI, PET, optical coherence tomography, and biomarkers).
“The paper reports there is no qualitative difference between relapsing remitting and progressive MS; rather, the difference is quantitative,” Dr. Cohen noted. “In other words, the processes that underlie progression are present from the earliest stages of MS, becoming more prominent over time.”
The apparent transition to progressive MS, he added, “rather than representing a ‘transition,’ instead results from the accumulation of pathology over time, a shift from focal lesions to diffuse inflammation and damage, and unmasking of the damage due to decreased resiliency due to aging and failure of compensatory mechanisms (neuroplasticity and remyelination).”
Also commenting, Edward Fox, MD, director, MS Clinic of Central Texas and clinical associate professor, University of Texas, Austin, explained that loss of tissue is the main driver of progressive MS.
“We all look at imaging to confirm that the progressive symptoms expressed by the patient are related to demyelinating disease,” he said. “When I see MRI of the spinal cord showing multifocal lesions, especially if localized atrophy is seen in a region of the cord, I expect to hear a history of progressive deficits in gait and other signs of disability.”
Dr. Fox noted that, on MRI of the brain, gray matter atrophy both cortically and in the deep gray structures usually manifests as cognitive slowing and poorer performance in work and social situations.
“We hope that other biomarkers, such as neurofilament light chain, will add to this body of knowledge and give us a better grasp of the definition of neurodegeneration to confirm the clinical and radiographic findings,” he added.
Dr. Filippi has received compensation for consulting services and/or speaking activities from Bayer, Biogen Idec, Merck Serono, Novartis, Roche, Sanofi, Genzyme, Takeda, and Teva Pharmaceutical Industries; and research support from ARiSLA, Biogen Idec, Fondazione Italiana Sclerosi Multipla, Italian Ministry of Health, Merck Serono, Novartis, Roche, and Teva.
A version of this article first appeared on Medscape.com.
Updates in HER2-positive Metastatic Breast Cancer Clinical Trials from SABCS 2020
Dr. Sara Hurvitz, Director of the Breast Cancer Clinical Trials Program at UCLA, reviews key updates in HER2-positive metastatic breast cancer studies presented during the 2020 San Antonio Breast Cancer Symposium (SABCS), which was held virtually in December.
A sub-analysis of patients who had central nervous system disease at baseline demonstrated improved outcomes with neratinib plus capecitabine compared with those receiving lapatinib plus capecitabine in the NALA trial.
Updated results from the DESTINY-breast01 study of trastuzumab deruxtecan show encouraging results in progression-free survival and early overall survival and high rates of durable responses in a heavily pretreated group of patients with metastatic breast cancer, consistent with early results.
In the HER2CLIMB study, patients treated with tucatinib in combination with trastuzumab and capecitabine had clinically meaningful improvement in progression-free survival, overall survival, and objective response rate independent of HR status compared with placebo, and patients with HR+ and HR- breast cancer with brain metastases experienced similar benefits.
--
Sara A. Hurvitz, MD, FACP, Professor of Medicine. Director, Breast Cancer Clinical Trials Program, Division of Hematology-Oncology David Geffen School of Medicine at UCLA
Medical Director, Clinical Research Unit, UCLA Jonsson Comprehensive Cancer Center.
Dr. Hurvitz has received research grants from: Ambrx; Amgen Inc.; Bayer HealthCare Pharmaceuticals; Daiichi Sankyo, Inc.; Dignitana AB; Eli Lilly and Company; Genentech, Inc.; GlaxoSmithKline; Immunomedics; MacroGenics, Inc.; Novartis Pharmaceuticals Corporation; OBI Pharma, Inc.; Pfizer Inc; Pieris Pharmaceuticals Inc; Puma Biotechnology; Radius Health; Roche Pharma; sanofi-aventis; Seattle Genetics, Inc.
Dr. Sara Hurvitz, Director of the Breast Cancer Clinical Trials Program at UCLA, reviews key updates in HER2-positive metastatic breast cancer studies presented during the 2020 San Antonio Breast Cancer Symposium (SABCS), which was held virtually in December.
A sub-analysis of patients who had central nervous system disease at baseline demonstrated improved outcomes with neratinib plus capecitabine compared with those receiving lapatinib plus capecitabine in the NALA trial.
Updated results from the DESTINY-breast01 study of trastuzumab deruxtecan show encouraging results in progression-free survival and early overall survival and high rates of durable responses in a heavily pretreated group of patients with metastatic breast cancer, consistent with early results.
In the HER2CLIMB study, patients treated with tucatinib in combination with trastuzumab and capecitabine had clinically meaningful improvement in progression-free survival, overall survival, and objective response rate independent of HR status compared with placebo, and patients with HR+ and HR- breast cancer with brain metastases experienced similar benefits.
--
Sara A. Hurvitz, MD, FACP, Professor of Medicine. Director, Breast Cancer Clinical Trials Program, Division of Hematology-Oncology David Geffen School of Medicine at UCLA
Medical Director, Clinical Research Unit, UCLA Jonsson Comprehensive Cancer Center.
Dr. Hurvitz has received research grants from: Ambrx; Amgen Inc.; Bayer HealthCare Pharmaceuticals; Daiichi Sankyo, Inc.; Dignitana AB; Eli Lilly and Company; Genentech, Inc.; GlaxoSmithKline; Immunomedics; MacroGenics, Inc.; Novartis Pharmaceuticals Corporation; OBI Pharma, Inc.; Pfizer Inc; Pieris Pharmaceuticals Inc; Puma Biotechnology; Radius Health; Roche Pharma; sanofi-aventis; Seattle Genetics, Inc.
Dr. Sara Hurvitz, Director of the Breast Cancer Clinical Trials Program at UCLA, reviews key updates in HER2-positive metastatic breast cancer studies presented during the 2020 San Antonio Breast Cancer Symposium (SABCS), which was held virtually in December.
A sub-analysis of patients who had central nervous system disease at baseline demonstrated improved outcomes with neratinib plus capecitabine compared with those receiving lapatinib plus capecitabine in the NALA trial.
Updated results from the DESTINY-breast01 study of trastuzumab deruxtecan show encouraging results in progression-free survival and early overall survival and high rates of durable responses in a heavily pretreated group of patients with metastatic breast cancer, consistent with early results.
In the HER2CLIMB study, patients treated with tucatinib in combination with trastuzumab and capecitabine had clinically meaningful improvement in progression-free survival, overall survival, and objective response rate independent of HR status compared with placebo, and patients with HR+ and HR- breast cancer with brain metastases experienced similar benefits.
--
Sara A. Hurvitz, MD, FACP, Professor of Medicine. Director, Breast Cancer Clinical Trials Program, Division of Hematology-Oncology David Geffen School of Medicine at UCLA
Medical Director, Clinical Research Unit, UCLA Jonsson Comprehensive Cancer Center.
Dr. Hurvitz has received research grants from: Ambrx; Amgen Inc.; Bayer HealthCare Pharmaceuticals; Daiichi Sankyo, Inc.; Dignitana AB; Eli Lilly and Company; Genentech, Inc.; GlaxoSmithKline; Immunomedics; MacroGenics, Inc.; Novartis Pharmaceuticals Corporation; OBI Pharma, Inc.; Pfizer Inc; Pieris Pharmaceuticals Inc; Puma Biotechnology; Radius Health; Roche Pharma; sanofi-aventis; Seattle Genetics, Inc.
