User login
Evolving strategies in sequencing for HER2+ MBC therapy
The landscape for therapies targeting HER2-positive metastatic breast cancer (MBC) has evolved rapidly in the past few years. In a 12-month window, the U.S. Food and Drug Administration approved four agents targeting human epidermal growth factor 2 (HER2)–positive MBC, starting with trastuzumab deruxtecan in December 2019, followed by neratinib and tucatinib a few months later, and margetuximab last December.
Although first-line therapy for the majority of patients continues to be the CLEOPATRA regimen — the monoclonal antibodies trastuzumab and pertuzumab plus a taxane, such as docetaxel or paclitaxel — .
“We have been really fortunate to see a number of highly effective new therapies approved for HER2-positive MBC in the past year, and this has given us even more options to offer our patients,” remarked Rita Nanda, MD, director of the Breast Oncology Program and associate professor of medicine at University of Chicago Medicine.
What considerations do experts weigh when sequencing HER2-positive MBC?
For Kelly McCann, MD, PhD, the order largely depends on balancing two factors: regimens that will provide the best efficacy in terms of patient survival and quality of life. “In the metastatic setting, I know I’m going to end up using all of the available medications one after the other, so the order that allows patients to continue living their best life for as long as possible is essential,” commented Dr. McCann, a hematologist/oncologist in the department of medicine at the David Geffen School of Medicine, University of California, Los Angeles.
A new second-line option?
Before the wave of drug approvals for metastatic HER2-positive disease last year, oncologists routinely looked to trastuzumab emtansine (T-DM1) as second-line therapy.
But tucatinib may also now be considered in the second-line setting, after results from the HER2CLIMB trial. The decision between tucatinib and T-DM1 largely comes down to the presence or absence of brain metastases.
“T-DM1 is well-tolerated, so it’s still my go-to in the second-line setting unless my patient has a brain metastasis, in which case I opt for tucatinib,” Dr. McCann noted, adding that the HER2-specific oral tyrosine kinase inhibitor (TKI) not only crosses the blood-brain barrier but is also effective in patients with untreated brain metastases.
In HER2CLIMB, tucatinib exhibited strong efficacy in patients with advanced HER2-positive disease, including those with previously treated or untreated brain metastases. The randomized controlled trial, which paired tucatinib with trastuzumab and capecitabine, showed median progression-free survival of 7.8 months in 410 patients with HER2-positive MBC compared with 5.6 months in the 202 patients receiving the placebo regimen. The tucatinib cohort showed an overall survival advantage compared with the placebo group (21.9 vs 17.4 months).
Perhaps the most notable finding occurred in patients with brain or central nervous system (CNS) involvement, which develops in as many as half of patients with HER-positive MBC and is associated with shorter survival. In the HER2CLIMB trial, median progression-free survival was 7.6 months in patients with brain metastases compared with 5.4 months in the placebo group.
A follow-up exploratory analysis, which focused on 291 patients with brain metastases, found that adding tucatinib reduced the risk for intracranial progression by two thirds and death by almost half. In patients with active brain metastases, median progression-free survival reached 9.5 months vs 4.1 months in the placebo group. Those with stable metastases also benefited from tucatinib, with median progression-free survival of 13.9 vs 5.6 months in the placebo group.
On the basis of the results, the authors concluded that this randomized trial was the first to demonstrate improvements in both CNS progression–free survival and overall survival in patients with HER2-positive MBC and brain metastases.
Evolving options in the third-line setting and after
For third-line therapy and beyond, oncologists have an array of newer agents to choose from alongside longer-standing options — which include trastuzumab plus lapatinib, trastuzumab or lapatinib plus capecitabine, as well as T-DM1, if not given as second-line therapy.
According to Dr. McCann, the antibody-drug conjugate trastuzumab deruxtecan has been a particularly exciting addition to third-line treatment. In the phase 2 DESTINY-01 trial, more than 60% of a heavily pretreated population showed an objective response to trastuzumab deruxtecan, with a median response duration of almost 15 months and a median progression-free survival of 16.4 months. Longer-term follow-up results, presented in December at the 2020 San Antonio Breast Cancer Symposium, revealed progression-free survival of 19.4 months and preliminary median overall survival of 24.6 months.
Neratinib, the second TKI to bridge the blood-brain barrier in HER2-positive disease, was also approved for third-line use; however, Sayeh Lavasani, MD, MS, said she is more likely to consider this agent later in the sequence, potentially in the fourth-line setting and beyond, given the more robust outcomes observed in the HER2CLIMB tucatinib trial.
“Neratinib improved progression-free survival and time to intervention for CNS metastasis but, unlike tucatinib, did not demonstrate an overall survival benefit,” remarked Dr. Lavasani, a medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County.
More specifically, the phase 3 NALA trial, which randomly assigned patients to receive neratinib plus capecitabine or lapatinib plus capecitabine, reported progression-free survival of 8.8 months in the neratinib group compared with 6.6 months in the control arm but no significant gains in overall survival (hazard ratio, 0.88; P = .2098).
The fourth recently approved drug, margetuximab, has not yet made a significant mark on sequencing decisions for Dr. McCann.
“Margetuximab could have been a potential game changer, but clinical trial results were underwhelming,” she said.
In the phase 3 randomized clinical SOPHIA trial, margetuximab plus chemotherapy prolonged median progression-free survival by just over 1 month compared with trastuzumab plus chemotherapy. Preliminary overall survival data showed a slight, but not significant, benefit in the margetuximab group (21.6 vs 19.8 months).
For Dr. Lavasani, the presence of brain metastases is the most important consideration when weighing sequencing options. “For some of my patients with HER2-positive MBC, it’s ultimately disease progression in the brain that takes their life,” she said.
Aside from CNS metastases, specific sequencing choices may vary on the basis of drug-related tolerance as well as patient preferences. “It is critical to get a patient’s input in treatment selection,” Dr. Nanda remarked. “Given the number of effective treatments for HER2-positive MBC and the lack of data to guide how to sequence these regimens, it is important to ask patients what their preferences are.”
Dr. McCann agreed, noting that “a patient with HER2-positive MBC typically has a life expectancy measured in years, which is also why sequencing should be influenced by quality of life considerations.”
Convenience, side-effect profile, and financial toxicity should factor into clinical decision-making, according to Dr. Nanda. Some patients may, for instance, prefer a combination of tucatinib, capecitabine, and trastuzumab over trastuzumab deruxtecan to avoid hair loss and the risk for interstitial lung disease, which has been reported in more than 13% of patients, whereas others may prefer trastuzumab deruxtecan to avoid the possibility of diarrhea.
Taxanes come with a high risk for infusion reactions — which occur in about 30% of patients — and can cause neuropathy as well as hair loss and severe gastrointestinal side effects. In first-line care, Dr. McCann typically stops the taxane at some point for toxicity reasons and continues with trastuzumab plus pertuzumab until disease progression.
Even with an array of new options for treating metastatic HER2-positive disease, ultimately drug resistance does occur, Dr. Lavasani cautioned. Several ongoing trials are exploring new combinations of existing drugs to see whether those variations move the needle on survival outcomes. The HER2CLIMB-04 trial, for instance, is pairing tucatinib with trastuzumab deruxtecan, whereas HER2CLIMB-02 is pairing tucatinib with T-DM1.
But given progress in drug development in just the past few years, Lisa A. Carey, MD, deputy director of Clinical Sciences at the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, sees a promising future for treating metastatic HER2-positive disease. “There is so much going on in the HER2-positive MBC therapeutics space that almost every 6 months, oncologists have to regroup and reevaluate treatment and sequencing, which is a great position to be in,” Dr. Carey noted.
A version of this article first appeared on Medscape.com .
The landscape for therapies targeting HER2-positive metastatic breast cancer (MBC) has evolved rapidly in the past few years. In a 12-month window, the U.S. Food and Drug Administration approved four agents targeting human epidermal growth factor 2 (HER2)–positive MBC, starting with trastuzumab deruxtecan in December 2019, followed by neratinib and tucatinib a few months later, and margetuximab last December.
Although first-line therapy for the majority of patients continues to be the CLEOPATRA regimen — the monoclonal antibodies trastuzumab and pertuzumab plus a taxane, such as docetaxel or paclitaxel — .
“We have been really fortunate to see a number of highly effective new therapies approved for HER2-positive MBC in the past year, and this has given us even more options to offer our patients,” remarked Rita Nanda, MD, director of the Breast Oncology Program and associate professor of medicine at University of Chicago Medicine.
What considerations do experts weigh when sequencing HER2-positive MBC?
For Kelly McCann, MD, PhD, the order largely depends on balancing two factors: regimens that will provide the best efficacy in terms of patient survival and quality of life. “In the metastatic setting, I know I’m going to end up using all of the available medications one after the other, so the order that allows patients to continue living their best life for as long as possible is essential,” commented Dr. McCann, a hematologist/oncologist in the department of medicine at the David Geffen School of Medicine, University of California, Los Angeles.
A new second-line option?
Before the wave of drug approvals for metastatic HER2-positive disease last year, oncologists routinely looked to trastuzumab emtansine (T-DM1) as second-line therapy.
But tucatinib may also now be considered in the second-line setting, after results from the HER2CLIMB trial. The decision between tucatinib and T-DM1 largely comes down to the presence or absence of brain metastases.
“T-DM1 is well-tolerated, so it’s still my go-to in the second-line setting unless my patient has a brain metastasis, in which case I opt for tucatinib,” Dr. McCann noted, adding that the HER2-specific oral tyrosine kinase inhibitor (TKI) not only crosses the blood-brain barrier but is also effective in patients with untreated brain metastases.
In HER2CLIMB, tucatinib exhibited strong efficacy in patients with advanced HER2-positive disease, including those with previously treated or untreated brain metastases. The randomized controlled trial, which paired tucatinib with trastuzumab and capecitabine, showed median progression-free survival of 7.8 months in 410 patients with HER2-positive MBC compared with 5.6 months in the 202 patients receiving the placebo regimen. The tucatinib cohort showed an overall survival advantage compared with the placebo group (21.9 vs 17.4 months).
Perhaps the most notable finding occurred in patients with brain or central nervous system (CNS) involvement, which develops in as many as half of patients with HER-positive MBC and is associated with shorter survival. In the HER2CLIMB trial, median progression-free survival was 7.6 months in patients with brain metastases compared with 5.4 months in the placebo group.
A follow-up exploratory analysis, which focused on 291 patients with brain metastases, found that adding tucatinib reduced the risk for intracranial progression by two thirds and death by almost half. In patients with active brain metastases, median progression-free survival reached 9.5 months vs 4.1 months in the placebo group. Those with stable metastases also benefited from tucatinib, with median progression-free survival of 13.9 vs 5.6 months in the placebo group.
On the basis of the results, the authors concluded that this randomized trial was the first to demonstrate improvements in both CNS progression–free survival and overall survival in patients with HER2-positive MBC and brain metastases.
Evolving options in the third-line setting and after
For third-line therapy and beyond, oncologists have an array of newer agents to choose from alongside longer-standing options — which include trastuzumab plus lapatinib, trastuzumab or lapatinib plus capecitabine, as well as T-DM1, if not given as second-line therapy.
According to Dr. McCann, the antibody-drug conjugate trastuzumab deruxtecan has been a particularly exciting addition to third-line treatment. In the phase 2 DESTINY-01 trial, more than 60% of a heavily pretreated population showed an objective response to trastuzumab deruxtecan, with a median response duration of almost 15 months and a median progression-free survival of 16.4 months. Longer-term follow-up results, presented in December at the 2020 San Antonio Breast Cancer Symposium, revealed progression-free survival of 19.4 months and preliminary median overall survival of 24.6 months.
Neratinib, the second TKI to bridge the blood-brain barrier in HER2-positive disease, was also approved for third-line use; however, Sayeh Lavasani, MD, MS, said she is more likely to consider this agent later in the sequence, potentially in the fourth-line setting and beyond, given the more robust outcomes observed in the HER2CLIMB tucatinib trial.
“Neratinib improved progression-free survival and time to intervention for CNS metastasis but, unlike tucatinib, did not demonstrate an overall survival benefit,” remarked Dr. Lavasani, a medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County.
More specifically, the phase 3 NALA trial, which randomly assigned patients to receive neratinib plus capecitabine or lapatinib plus capecitabine, reported progression-free survival of 8.8 months in the neratinib group compared with 6.6 months in the control arm but no significant gains in overall survival (hazard ratio, 0.88; P = .2098).
The fourth recently approved drug, margetuximab, has not yet made a significant mark on sequencing decisions for Dr. McCann.
“Margetuximab could have been a potential game changer, but clinical trial results were underwhelming,” she said.
In the phase 3 randomized clinical SOPHIA trial, margetuximab plus chemotherapy prolonged median progression-free survival by just over 1 month compared with trastuzumab plus chemotherapy. Preliminary overall survival data showed a slight, but not significant, benefit in the margetuximab group (21.6 vs 19.8 months).
For Dr. Lavasani, the presence of brain metastases is the most important consideration when weighing sequencing options. “For some of my patients with HER2-positive MBC, it’s ultimately disease progression in the brain that takes their life,” she said.
Aside from CNS metastases, specific sequencing choices may vary on the basis of drug-related tolerance as well as patient preferences. “It is critical to get a patient’s input in treatment selection,” Dr. Nanda remarked. “Given the number of effective treatments for HER2-positive MBC and the lack of data to guide how to sequence these regimens, it is important to ask patients what their preferences are.”
Dr. McCann agreed, noting that “a patient with HER2-positive MBC typically has a life expectancy measured in years, which is also why sequencing should be influenced by quality of life considerations.”
Convenience, side-effect profile, and financial toxicity should factor into clinical decision-making, according to Dr. Nanda. Some patients may, for instance, prefer a combination of tucatinib, capecitabine, and trastuzumab over trastuzumab deruxtecan to avoid hair loss and the risk for interstitial lung disease, which has been reported in more than 13% of patients, whereas others may prefer trastuzumab deruxtecan to avoid the possibility of diarrhea.
Taxanes come with a high risk for infusion reactions — which occur in about 30% of patients — and can cause neuropathy as well as hair loss and severe gastrointestinal side effects. In first-line care, Dr. McCann typically stops the taxane at some point for toxicity reasons and continues with trastuzumab plus pertuzumab until disease progression.
Even with an array of new options for treating metastatic HER2-positive disease, ultimately drug resistance does occur, Dr. Lavasani cautioned. Several ongoing trials are exploring new combinations of existing drugs to see whether those variations move the needle on survival outcomes. The HER2CLIMB-04 trial, for instance, is pairing tucatinib with trastuzumab deruxtecan, whereas HER2CLIMB-02 is pairing tucatinib with T-DM1.
But given progress in drug development in just the past few years, Lisa A. Carey, MD, deputy director of Clinical Sciences at the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, sees a promising future for treating metastatic HER2-positive disease. “There is so much going on in the HER2-positive MBC therapeutics space that almost every 6 months, oncologists have to regroup and reevaluate treatment and sequencing, which is a great position to be in,” Dr. Carey noted.
A version of this article first appeared on Medscape.com .
The landscape for therapies targeting HER2-positive metastatic breast cancer (MBC) has evolved rapidly in the past few years. In a 12-month window, the U.S. Food and Drug Administration approved four agents targeting human epidermal growth factor 2 (HER2)–positive MBC, starting with trastuzumab deruxtecan in December 2019, followed by neratinib and tucatinib a few months later, and margetuximab last December.
Although first-line therapy for the majority of patients continues to be the CLEOPATRA regimen — the monoclonal antibodies trastuzumab and pertuzumab plus a taxane, such as docetaxel or paclitaxel — .
“We have been really fortunate to see a number of highly effective new therapies approved for HER2-positive MBC in the past year, and this has given us even more options to offer our patients,” remarked Rita Nanda, MD, director of the Breast Oncology Program and associate professor of medicine at University of Chicago Medicine.
What considerations do experts weigh when sequencing HER2-positive MBC?
For Kelly McCann, MD, PhD, the order largely depends on balancing two factors: regimens that will provide the best efficacy in terms of patient survival and quality of life. “In the metastatic setting, I know I’m going to end up using all of the available medications one after the other, so the order that allows patients to continue living their best life for as long as possible is essential,” commented Dr. McCann, a hematologist/oncologist in the department of medicine at the David Geffen School of Medicine, University of California, Los Angeles.
A new second-line option?
Before the wave of drug approvals for metastatic HER2-positive disease last year, oncologists routinely looked to trastuzumab emtansine (T-DM1) as second-line therapy.
But tucatinib may also now be considered in the second-line setting, after results from the HER2CLIMB trial. The decision between tucatinib and T-DM1 largely comes down to the presence or absence of brain metastases.
“T-DM1 is well-tolerated, so it’s still my go-to in the second-line setting unless my patient has a brain metastasis, in which case I opt for tucatinib,” Dr. McCann noted, adding that the HER2-specific oral tyrosine kinase inhibitor (TKI) not only crosses the blood-brain barrier but is also effective in patients with untreated brain metastases.
In HER2CLIMB, tucatinib exhibited strong efficacy in patients with advanced HER2-positive disease, including those with previously treated or untreated brain metastases. The randomized controlled trial, which paired tucatinib with trastuzumab and capecitabine, showed median progression-free survival of 7.8 months in 410 patients with HER2-positive MBC compared with 5.6 months in the 202 patients receiving the placebo regimen. The tucatinib cohort showed an overall survival advantage compared with the placebo group (21.9 vs 17.4 months).
Perhaps the most notable finding occurred in patients with brain or central nervous system (CNS) involvement, which develops in as many as half of patients with HER-positive MBC and is associated with shorter survival. In the HER2CLIMB trial, median progression-free survival was 7.6 months in patients with brain metastases compared with 5.4 months in the placebo group.
A follow-up exploratory analysis, which focused on 291 patients with brain metastases, found that adding tucatinib reduced the risk for intracranial progression by two thirds and death by almost half. In patients with active brain metastases, median progression-free survival reached 9.5 months vs 4.1 months in the placebo group. Those with stable metastases also benefited from tucatinib, with median progression-free survival of 13.9 vs 5.6 months in the placebo group.
On the basis of the results, the authors concluded that this randomized trial was the first to demonstrate improvements in both CNS progression–free survival and overall survival in patients with HER2-positive MBC and brain metastases.
Evolving options in the third-line setting and after
For third-line therapy and beyond, oncologists have an array of newer agents to choose from alongside longer-standing options — which include trastuzumab plus lapatinib, trastuzumab or lapatinib plus capecitabine, as well as T-DM1, if not given as second-line therapy.
According to Dr. McCann, the antibody-drug conjugate trastuzumab deruxtecan has been a particularly exciting addition to third-line treatment. In the phase 2 DESTINY-01 trial, more than 60% of a heavily pretreated population showed an objective response to trastuzumab deruxtecan, with a median response duration of almost 15 months and a median progression-free survival of 16.4 months. Longer-term follow-up results, presented in December at the 2020 San Antonio Breast Cancer Symposium, revealed progression-free survival of 19.4 months and preliminary median overall survival of 24.6 months.
Neratinib, the second TKI to bridge the blood-brain barrier in HER2-positive disease, was also approved for third-line use; however, Sayeh Lavasani, MD, MS, said she is more likely to consider this agent later in the sequence, potentially in the fourth-line setting and beyond, given the more robust outcomes observed in the HER2CLIMB tucatinib trial.
“Neratinib improved progression-free survival and time to intervention for CNS metastasis but, unlike tucatinib, did not demonstrate an overall survival benefit,” remarked Dr. Lavasani, a medical oncologist at City of Hope, a comprehensive cancer center in Los Angeles County.
More specifically, the phase 3 NALA trial, which randomly assigned patients to receive neratinib plus capecitabine or lapatinib plus capecitabine, reported progression-free survival of 8.8 months in the neratinib group compared with 6.6 months in the control arm but no significant gains in overall survival (hazard ratio, 0.88; P = .2098).
The fourth recently approved drug, margetuximab, has not yet made a significant mark on sequencing decisions for Dr. McCann.
“Margetuximab could have been a potential game changer, but clinical trial results were underwhelming,” she said.
In the phase 3 randomized clinical SOPHIA trial, margetuximab plus chemotherapy prolonged median progression-free survival by just over 1 month compared with trastuzumab plus chemotherapy. Preliminary overall survival data showed a slight, but not significant, benefit in the margetuximab group (21.6 vs 19.8 months).
For Dr. Lavasani, the presence of brain metastases is the most important consideration when weighing sequencing options. “For some of my patients with HER2-positive MBC, it’s ultimately disease progression in the brain that takes their life,” she said.
Aside from CNS metastases, specific sequencing choices may vary on the basis of drug-related tolerance as well as patient preferences. “It is critical to get a patient’s input in treatment selection,” Dr. Nanda remarked. “Given the number of effective treatments for HER2-positive MBC and the lack of data to guide how to sequence these regimens, it is important to ask patients what their preferences are.”
Dr. McCann agreed, noting that “a patient with HER2-positive MBC typically has a life expectancy measured in years, which is also why sequencing should be influenced by quality of life considerations.”
Convenience, side-effect profile, and financial toxicity should factor into clinical decision-making, according to Dr. Nanda. Some patients may, for instance, prefer a combination of tucatinib, capecitabine, and trastuzumab over trastuzumab deruxtecan to avoid hair loss and the risk for interstitial lung disease, which has been reported in more than 13% of patients, whereas others may prefer trastuzumab deruxtecan to avoid the possibility of diarrhea.
Taxanes come with a high risk for infusion reactions — which occur in about 30% of patients — and can cause neuropathy as well as hair loss and severe gastrointestinal side effects. In first-line care, Dr. McCann typically stops the taxane at some point for toxicity reasons and continues with trastuzumab plus pertuzumab until disease progression.
Even with an array of new options for treating metastatic HER2-positive disease, ultimately drug resistance does occur, Dr. Lavasani cautioned. Several ongoing trials are exploring new combinations of existing drugs to see whether those variations move the needle on survival outcomes. The HER2CLIMB-04 trial, for instance, is pairing tucatinib with trastuzumab deruxtecan, whereas HER2CLIMB-02 is pairing tucatinib with T-DM1.
But given progress in drug development in just the past few years, Lisa A. Carey, MD, deputy director of Clinical Sciences at the University of North Carolina Lineberger Comprehensive Cancer Center in Chapel Hill, sees a promising future for treating metastatic HER2-positive disease. “There is so much going on in the HER2-positive MBC therapeutics space that almost every 6 months, oncologists have to regroup and reevaluate treatment and sequencing, which is a great position to be in,” Dr. Carey noted.
A version of this article first appeared on Medscape.com .
Medication overuse headache: Preventive treatment with or without detoxification?

The goal of treating medication overuse headache is obvious: ceasing overuse of the medication in question in an effort to return to a headache pattern that is episodic and better managed. Although guidelines suggest withdrawal of the overused medication and initiating preventive treatment, there is debate about this approach versus withdrawal alone or preventive treatment without ceasing the overused medication. A recently published randomized trial from Carlsen and colleagues evaluated 3 treatment methods: 1) withdrawal plus preventive treatment; 2) preventive treatment only; and 3) withdrawal followed by optional preventive treatment 2 months after withdrawal. Investigators found all 3 approaches effective, but participants who underwent withdrawal plus preventive care saw their headache days reduced by 12.3 days, versus 9.9 days in the preventive-only group and 8.5 days in the withdrawal/optional preventive follow-up treatment contingent. No statistically significant differences were seen between the groups in terms of migraine days, days with short-term medication use, and headache pain intensity.
Particularly noteworthy was the finding that individuals treated with withdrawal plus preventive treatment were significantly more likely to achieve remission. Specifically, nearly 75% returned to experiencing episodic headache, compared with 60% in the preventive group and 42% in the withdrawal contingent. Nearly all (97%) of those on the withdrawal plus preventive regimen were cured of medication overuse headache, versus 90% (withdrawal) and 74% (preventive).
The bottom line: Individuals undergoing withdrawal plus preventive treatment were 30% more likely to be cured of medication overuse headache. Thus, it appears that detoxification is key.
Or is it?
On the one hand…
In studies, withdrawal from the offending medication is linked with substantial improvement in headache days. Additionally, individuals who previously responded poorly to preventive treatment fared better with such treatment after detoxification.
When treating medication overuse headache using the detoxification and preventive care approach, Sun-Edelstein and colleagues outline these important steps:
- Educate your patients and their family/caregivers about the detoxification process
- Wean patient off the offending medication with a goal of complete detoxification
- Initiate preventive medical therapy or behavioral/non-drug strategies
- Establish clear limits on acute medication intake
- Arrange for regular follow-up to minimize or prevent relapse
While on the other hand…
Even though guidelines recommend detoxification, there is data supporting the concept of initiating preventive treatment without detoxification. A randomized, double-blind, placebo-controlled trial by Mei and colleagues found that 100 mg per day of topiramate led to a significant reduction in headache days and average amount of acute medication intake, versus placebo. However, treatment completion rates were low, leading Sun-Edelstein and colleagues to surmise that topiramate without detoxification would probably not have had a high success rate in practice.
Meanwhile, onabotulinumtoxin A was found in the PREEMPT trials conducted by Dodick and colleagues to reduce the number of headache days, migraine days, and moderate/severe headache days, compared with placebo, at week 24. Disappointingly, researchers found that acute medication frequency was not reduced in the overall treatment group, but they did note a significant reduction in the subgroup that was taking triptans. Moreover, a follow-up analysis by Aurora and colleagues involving 32 weeks of open-label treatment with onabotulinumtoxin A following the 24-week randomized study revealed significant reductions in acute headache days at 56 weeks.
Using anti-CGRPs without acute medication withdrawal
More recently, strong evidence is emerging about the value of using anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies without acute medication withdrawal. The findings involve 4 anti-CGRP medications.
Erenumab: A subgroup analysis of a randomized, double-blind, placebo-controlled parallel-group trial by Tepper and colleagues showed that erenumab reduced frequency of migraine at 3 months in participants with chronic migraine and medication overuse. Patients receiving either 70 or 140 mg of erenumab saw their migraine frequency reduced by an average of 6.6 days, versus 3.5 days in the placebo group.
Additionally, a significantly greater number of patients in the treatment groups stopped overusing medication, and did so early, which led to improved patient-reported outcomes. Acute migraine-specific medication treatment days were reduced by an average of 5.4 days in the 70 mg group, 4.9 days in the 140 mg contingent, and 2.9 days in those who received placebo.
Overall, consistent improvement in measures of impact, disability and health-related quality of life were seen in individuals’ treatment with erenumab.
Galcanezumab: A post-hoc analysis of pooled data from the phase 3 EVOLVE-1 and EVOLVE-2 studies, as well as the phase 3 REGAIN trial found that in participants with medication overuse, 120 mg and 240 mg doses of galcanezumab cut the number of average migraine days and decreased medication overuse. Average migraine days were lowered in EVOLVE participants by 6.26 days in the 120 mg group, 5.77 days in the 240 mg contingent, and 2.71 in those who received placebo. In REGAIN, these numbers were 4.78, 4.51, and 2.25, respectively. Average monthly medication use rates in EVOLVE were 6.2%, 7.9%, and 15.9%, respectively; in REGAIN they were 24.3%, 23.1%, and 40.6%, respectively.
Notably, though the study demonstrated galcanezumab’s efficacy in those with and without medication overuse, improvement was more pronounced in patients with medication overuse.
Fremanezumab: In an analysis by Silberstein and colleagues, significantly more patients who received quarterly or monthly injections of fremanezumab reported no medication overuse during the 3-month study, versus placebo. Specifically, 61% of participants who received monthly injections of fremanezumab and 55% of those who took quarterly injections reported no medication overuse. Among those receiving placebo, only 46% reverted to no overuse. The effect was seen as early as week 4. Additionally, among patients with medication overuse at baseline, the number of days with acute medication use was significantly lower in the treatment groups versus placebo—1.8 days lower in the quarterly group and 2.8 days in the monthly contingent.
A subsequent post-hoc analysis presented at the 2019 American Headache Society (AHS) Annual Scientific Meeting showed that the benefits were sustained over time and the medication was effective in difficult cases. Continued treatment with either quarterly or monthly dosing resulted in a reduced number of headache days, acute medication overuse headache, and headache-related disability, compared with baseline measures. Notably, about 6 in every 10 individuals with medication overuse at baseline who received fremanezumab reverted to no acute medication overuse at 6 months. This effect was maintained through 1 year of treatment.
Eptinezumab: In PROMISE-2, a post-hoc analysis of the phase 3 trials evaluating quarterly IV infusions of eptinezumab 100 mg and 300 mg, Lipton and colleagues reported that participants with chronic migraine and medication overuse experienced greater reductions in monthly migraine days during weeks 1 through 12, versus placebo (100 mg, 7.7 days; 300 mg, 8.2 days; placebo, 5.6 days). Benefits, seen as early as the day after dosing, were generally maintained or improved over 24 weeks.
Acute care medication use was reduced by about 50% in the treatment group versus roughly 25% in the placebo contingent. Most encouraging was the finding that about one-third of individuals in the treatment cohort experienced 6 months without medication overuse and below the chronic migraine diagnostic threshold; only 10% of patients who received placebo resolved in this way. Consistent improvement across patient-reported outcomes was also observed in the treatment group versus placebo.
While the studies involving topiramate, onabotulinumtoxin A, and the anti-CGRP monoclonal antibodies suggest that preventive treatment alone may effectively treat acute medical overuse and medication overuse headache, it is the data behind the anti-CGRP treatments that seem to be most compelling and causing conventional thinking to be challenged. These medications appear to be able to convert individuals with chronic migraine and medication overuse, out of overuse and back to episodic migraine. Moreover, results show they may be able to reduce acute medication use in episodic migraine, which reduces the risk of the headache sufferer transforming to chronic migraine. It is worth considering this approach in patients’ overuse acute care medication, as well as those in whom discontinuation may otherwise prove difficult without concurrent preventive treatment.
The emerging role of gepants
Availability of the so-called “gepants”—small molecule CGRP receptor agonists—is shedding additional light on management of medication overuse headache and pointing to the future. Gepants—which include ubrogepant, rimegepant, and atogepant—have been shown in early data to have a preventive effect when used regularly. Thus, it is much less likely that their use will lead to excess use and medication overuse headache.
Preclinical data demonstrated that continued use of ubrogepant does not appear to produce early or latent trigeminal sensory sensitization. Meanwhile, rimegepant, when used every other day, and as needed for acute treatment of migraine in individuals suffering from moderate-to-high frequency episodic migraine, resulted in reductions in monthly migraine days. The preventive effects appear to be rapid and sustained. And in a phase 3 trial, atogepant demonstrated efficacy at doses of 10 mg, 30 mg, and 60 mg twice a day, compared with placebo over 12 weeks.
It is important to note that the link between the gepants and medication overuse and medication overuse headache have not yet been studied. Still, it is encouraging to see that migraine frequency improves and medication use days are reduced when gepants are taken preventively. Thus, gepants could emerge as a preferred approach for acute or preventive treatment in individuals who have or are at risk of developing medication overuse headache.
The goal of treating medication overuse headache is obvious: ceasing overuse of the medication in question in an effort to return to a headache pattern that is episodic and better managed. Although guidelines suggest withdrawal of the overused medication and initiating preventive treatment, there is debate about this approach versus withdrawal alone or preventive treatment without ceasing the overused medication. A recently published randomized trial from Carlsen and colleagues evaluated 3 treatment methods: 1) withdrawal plus preventive treatment; 2) preventive treatment only; and 3) withdrawal followed by optional preventive treatment 2 months after withdrawal. Investigators found all 3 approaches effective, but participants who underwent withdrawal plus preventive care saw their headache days reduced by 12.3 days, versus 9.9 days in the preventive-only group and 8.5 days in the withdrawal/optional preventive follow-up treatment contingent. No statistically significant differences were seen between the groups in terms of migraine days, days with short-term medication use, and headache pain intensity.
Particularly noteworthy was the finding that individuals treated with withdrawal plus preventive treatment were significantly more likely to achieve remission. Specifically, nearly 75% returned to experiencing episodic headache, compared with 60% in the preventive group and 42% in the withdrawal contingent. Nearly all (97%) of those on the withdrawal plus preventive regimen were cured of medication overuse headache, versus 90% (withdrawal) and 74% (preventive).
The bottom line: Individuals undergoing withdrawal plus preventive treatment were 30% more likely to be cured of medication overuse headache. Thus, it appears that detoxification is key.
Or is it?
On the one hand…
In studies, withdrawal from the offending medication is linked with substantial improvement in headache days. Additionally, individuals who previously responded poorly to preventive treatment fared better with such treatment after detoxification.
When treating medication overuse headache using the detoxification and preventive care approach, Sun-Edelstein and colleagues outline these important steps:
- Educate your patients and their family/caregivers about the detoxification process
- Wean patient off the offending medication with a goal of complete detoxification
- Initiate preventive medical therapy or behavioral/non-drug strategies
- Establish clear limits on acute medication intake
- Arrange for regular follow-up to minimize or prevent relapse
While on the other hand…
Even though guidelines recommend detoxification, there is data supporting the concept of initiating preventive treatment without detoxification. A randomized, double-blind, placebo-controlled trial by Mei and colleagues found that 100 mg per day of topiramate led to a significant reduction in headache days and average amount of acute medication intake, versus placebo. However, treatment completion rates were low, leading Sun-Edelstein and colleagues to surmise that topiramate without detoxification would probably not have had a high success rate in practice.
Meanwhile, onabotulinumtoxin A was found in the PREEMPT trials conducted by Dodick and colleagues to reduce the number of headache days, migraine days, and moderate/severe headache days, compared with placebo, at week 24. Disappointingly, researchers found that acute medication frequency was not reduced in the overall treatment group, but they did note a significant reduction in the subgroup that was taking triptans. Moreover, a follow-up analysis by Aurora and colleagues involving 32 weeks of open-label treatment with onabotulinumtoxin A following the 24-week randomized study revealed significant reductions in acute headache days at 56 weeks.
Using anti-CGRPs without acute medication withdrawal
More recently, strong evidence is emerging about the value of using anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies without acute medication withdrawal. The findings involve 4 anti-CGRP medications.
Erenumab: A subgroup analysis of a randomized, double-blind, placebo-controlled parallel-group trial by Tepper and colleagues showed that erenumab reduced frequency of migraine at 3 months in participants with chronic migraine and medication overuse. Patients receiving either 70 or 140 mg of erenumab saw their migraine frequency reduced by an average of 6.6 days, versus 3.5 days in the placebo group.
Additionally, a significantly greater number of patients in the treatment groups stopped overusing medication, and did so early, which led to improved patient-reported outcomes. Acute migraine-specific medication treatment days were reduced by an average of 5.4 days in the 70 mg group, 4.9 days in the 140 mg contingent, and 2.9 days in those who received placebo.
Overall, consistent improvement in measures of impact, disability and health-related quality of life were seen in individuals’ treatment with erenumab.
Galcanezumab: A post-hoc analysis of pooled data from the phase 3 EVOLVE-1 and EVOLVE-2 studies, as well as the phase 3 REGAIN trial found that in participants with medication overuse, 120 mg and 240 mg doses of galcanezumab cut the number of average migraine days and decreased medication overuse. Average migraine days were lowered in EVOLVE participants by 6.26 days in the 120 mg group, 5.77 days in the 240 mg contingent, and 2.71 in those who received placebo. In REGAIN, these numbers were 4.78, 4.51, and 2.25, respectively. Average monthly medication use rates in EVOLVE were 6.2%, 7.9%, and 15.9%, respectively; in REGAIN they were 24.3%, 23.1%, and 40.6%, respectively.
Notably, though the study demonstrated galcanezumab’s efficacy in those with and without medication overuse, improvement was more pronounced in patients with medication overuse.
Fremanezumab: In an analysis by Silberstein and colleagues, significantly more patients who received quarterly or monthly injections of fremanezumab reported no medication overuse during the 3-month study, versus placebo. Specifically, 61% of participants who received monthly injections of fremanezumab and 55% of those who took quarterly injections reported no medication overuse. Among those receiving placebo, only 46% reverted to no overuse. The effect was seen as early as week 4. Additionally, among patients with medication overuse at baseline, the number of days with acute medication use was significantly lower in the treatment groups versus placebo—1.8 days lower in the quarterly group and 2.8 days in the monthly contingent.
A subsequent post-hoc analysis presented at the 2019 American Headache Society (AHS) Annual Scientific Meeting showed that the benefits were sustained over time and the medication was effective in difficult cases. Continued treatment with either quarterly or monthly dosing resulted in a reduced number of headache days, acute medication overuse headache, and headache-related disability, compared with baseline measures. Notably, about 6 in every 10 individuals with medication overuse at baseline who received fremanezumab reverted to no acute medication overuse at 6 months. This effect was maintained through 1 year of treatment.
Eptinezumab: In PROMISE-2, a post-hoc analysis of the phase 3 trials evaluating quarterly IV infusions of eptinezumab 100 mg and 300 mg, Lipton and colleagues reported that participants with chronic migraine and medication overuse experienced greater reductions in monthly migraine days during weeks 1 through 12, versus placebo (100 mg, 7.7 days; 300 mg, 8.2 days; placebo, 5.6 days). Benefits, seen as early as the day after dosing, were generally maintained or improved over 24 weeks.
Acute care medication use was reduced by about 50% in the treatment group versus roughly 25% in the placebo contingent. Most encouraging was the finding that about one-third of individuals in the treatment cohort experienced 6 months without medication overuse and below the chronic migraine diagnostic threshold; only 10% of patients who received placebo resolved in this way. Consistent improvement across patient-reported outcomes was also observed in the treatment group versus placebo.
While the studies involving topiramate, onabotulinumtoxin A, and the anti-CGRP monoclonal antibodies suggest that preventive treatment alone may effectively treat acute medical overuse and medication overuse headache, it is the data behind the anti-CGRP treatments that seem to be most compelling and causing conventional thinking to be challenged. These medications appear to be able to convert individuals with chronic migraine and medication overuse, out of overuse and back to episodic migraine. Moreover, results show they may be able to reduce acute medication use in episodic migraine, which reduces the risk of the headache sufferer transforming to chronic migraine. It is worth considering this approach in patients’ overuse acute care medication, as well as those in whom discontinuation may otherwise prove difficult without concurrent preventive treatment.
The emerging role of gepants
Availability of the so-called “gepants”—small molecule CGRP receptor agonists—is shedding additional light on management of medication overuse headache and pointing to the future. Gepants—which include ubrogepant, rimegepant, and atogepant—have been shown in early data to have a preventive effect when used regularly. Thus, it is much less likely that their use will lead to excess use and medication overuse headache.
Preclinical data demonstrated that continued use of ubrogepant does not appear to produce early or latent trigeminal sensory sensitization. Meanwhile, rimegepant, when used every other day, and as needed for acute treatment of migraine in individuals suffering from moderate-to-high frequency episodic migraine, resulted in reductions in monthly migraine days. The preventive effects appear to be rapid and sustained. And in a phase 3 trial, atogepant demonstrated efficacy at doses of 10 mg, 30 mg, and 60 mg twice a day, compared with placebo over 12 weeks.
It is important to note that the link between the gepants and medication overuse and medication overuse headache have not yet been studied. Still, it is encouraging to see that migraine frequency improves and medication use days are reduced when gepants are taken preventively. Thus, gepants could emerge as a preferred approach for acute or preventive treatment in individuals who have or are at risk of developing medication overuse headache.
The goal of treating medication overuse headache is obvious: ceasing overuse of the medication in question in an effort to return to a headache pattern that is episodic and better managed. Although guidelines suggest withdrawal of the overused medication and initiating preventive treatment, there is debate about this approach versus withdrawal alone or preventive treatment without ceasing the overused medication. A recently published randomized trial from Carlsen and colleagues evaluated 3 treatment methods: 1) withdrawal plus preventive treatment; 2) preventive treatment only; and 3) withdrawal followed by optional preventive treatment 2 months after withdrawal. Investigators found all 3 approaches effective, but participants who underwent withdrawal plus preventive care saw their headache days reduced by 12.3 days, versus 9.9 days in the preventive-only group and 8.5 days in the withdrawal/optional preventive follow-up treatment contingent. No statistically significant differences were seen between the groups in terms of migraine days, days with short-term medication use, and headache pain intensity.
Particularly noteworthy was the finding that individuals treated with withdrawal plus preventive treatment were significantly more likely to achieve remission. Specifically, nearly 75% returned to experiencing episodic headache, compared with 60% in the preventive group and 42% in the withdrawal contingent. Nearly all (97%) of those on the withdrawal plus preventive regimen were cured of medication overuse headache, versus 90% (withdrawal) and 74% (preventive).
The bottom line: Individuals undergoing withdrawal plus preventive treatment were 30% more likely to be cured of medication overuse headache. Thus, it appears that detoxification is key.
Or is it?
On the one hand…
In studies, withdrawal from the offending medication is linked with substantial improvement in headache days. Additionally, individuals who previously responded poorly to preventive treatment fared better with such treatment after detoxification.
When treating medication overuse headache using the detoxification and preventive care approach, Sun-Edelstein and colleagues outline these important steps:
- Educate your patients and their family/caregivers about the detoxification process
- Wean patient off the offending medication with a goal of complete detoxification
- Initiate preventive medical therapy or behavioral/non-drug strategies
- Establish clear limits on acute medication intake
- Arrange for regular follow-up to minimize or prevent relapse
While on the other hand…
Even though guidelines recommend detoxification, there is data supporting the concept of initiating preventive treatment without detoxification. A randomized, double-blind, placebo-controlled trial by Mei and colleagues found that 100 mg per day of topiramate led to a significant reduction in headache days and average amount of acute medication intake, versus placebo. However, treatment completion rates were low, leading Sun-Edelstein and colleagues to surmise that topiramate without detoxification would probably not have had a high success rate in practice.
Meanwhile, onabotulinumtoxin A was found in the PREEMPT trials conducted by Dodick and colleagues to reduce the number of headache days, migraine days, and moderate/severe headache days, compared with placebo, at week 24. Disappointingly, researchers found that acute medication frequency was not reduced in the overall treatment group, but they did note a significant reduction in the subgroup that was taking triptans. Moreover, a follow-up analysis by Aurora and colleagues involving 32 weeks of open-label treatment with onabotulinumtoxin A following the 24-week randomized study revealed significant reductions in acute headache days at 56 weeks.
Using anti-CGRPs without acute medication withdrawal
More recently, strong evidence is emerging about the value of using anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies without acute medication withdrawal. The findings involve 4 anti-CGRP medications.
Erenumab: A subgroup analysis of a randomized, double-blind, placebo-controlled parallel-group trial by Tepper and colleagues showed that erenumab reduced frequency of migraine at 3 months in participants with chronic migraine and medication overuse. Patients receiving either 70 or 140 mg of erenumab saw their migraine frequency reduced by an average of 6.6 days, versus 3.5 days in the placebo group.
Additionally, a significantly greater number of patients in the treatment groups stopped overusing medication, and did so early, which led to improved patient-reported outcomes. Acute migraine-specific medication treatment days were reduced by an average of 5.4 days in the 70 mg group, 4.9 days in the 140 mg contingent, and 2.9 days in those who received placebo.
Overall, consistent improvement in measures of impact, disability and health-related quality of life were seen in individuals’ treatment with erenumab.
Galcanezumab: A post-hoc analysis of pooled data from the phase 3 EVOLVE-1 and EVOLVE-2 studies, as well as the phase 3 REGAIN trial found that in participants with medication overuse, 120 mg and 240 mg doses of galcanezumab cut the number of average migraine days and decreased medication overuse. Average migraine days were lowered in EVOLVE participants by 6.26 days in the 120 mg group, 5.77 days in the 240 mg contingent, and 2.71 in those who received placebo. In REGAIN, these numbers were 4.78, 4.51, and 2.25, respectively. Average monthly medication use rates in EVOLVE were 6.2%, 7.9%, and 15.9%, respectively; in REGAIN they were 24.3%, 23.1%, and 40.6%, respectively.
Notably, though the study demonstrated galcanezumab’s efficacy in those with and without medication overuse, improvement was more pronounced in patients with medication overuse.
Fremanezumab: In an analysis by Silberstein and colleagues, significantly more patients who received quarterly or monthly injections of fremanezumab reported no medication overuse during the 3-month study, versus placebo. Specifically, 61% of participants who received monthly injections of fremanezumab and 55% of those who took quarterly injections reported no medication overuse. Among those receiving placebo, only 46% reverted to no overuse. The effect was seen as early as week 4. Additionally, among patients with medication overuse at baseline, the number of days with acute medication use was significantly lower in the treatment groups versus placebo—1.8 days lower in the quarterly group and 2.8 days in the monthly contingent.
A subsequent post-hoc analysis presented at the 2019 American Headache Society (AHS) Annual Scientific Meeting showed that the benefits were sustained over time and the medication was effective in difficult cases. Continued treatment with either quarterly or monthly dosing resulted in a reduced number of headache days, acute medication overuse headache, and headache-related disability, compared with baseline measures. Notably, about 6 in every 10 individuals with medication overuse at baseline who received fremanezumab reverted to no acute medication overuse at 6 months. This effect was maintained through 1 year of treatment.
Eptinezumab: In PROMISE-2, a post-hoc analysis of the phase 3 trials evaluating quarterly IV infusions of eptinezumab 100 mg and 300 mg, Lipton and colleagues reported that participants with chronic migraine and medication overuse experienced greater reductions in monthly migraine days during weeks 1 through 12, versus placebo (100 mg, 7.7 days; 300 mg, 8.2 days; placebo, 5.6 days). Benefits, seen as early as the day after dosing, were generally maintained or improved over 24 weeks.
Acute care medication use was reduced by about 50% in the treatment group versus roughly 25% in the placebo contingent. Most encouraging was the finding that about one-third of individuals in the treatment cohort experienced 6 months without medication overuse and below the chronic migraine diagnostic threshold; only 10% of patients who received placebo resolved in this way. Consistent improvement across patient-reported outcomes was also observed in the treatment group versus placebo.
While the studies involving topiramate, onabotulinumtoxin A, and the anti-CGRP monoclonal antibodies suggest that preventive treatment alone may effectively treat acute medical overuse and medication overuse headache, it is the data behind the anti-CGRP treatments that seem to be most compelling and causing conventional thinking to be challenged. These medications appear to be able to convert individuals with chronic migraine and medication overuse, out of overuse and back to episodic migraine. Moreover, results show they may be able to reduce acute medication use in episodic migraine, which reduces the risk of the headache sufferer transforming to chronic migraine. It is worth considering this approach in patients’ overuse acute care medication, as well as those in whom discontinuation may otherwise prove difficult without concurrent preventive treatment.
The emerging role of gepants
Availability of the so-called “gepants”—small molecule CGRP receptor agonists—is shedding additional light on management of medication overuse headache and pointing to the future. Gepants—which include ubrogepant, rimegepant, and atogepant—have been shown in early data to have a preventive effect when used regularly. Thus, it is much less likely that their use will lead to excess use and medication overuse headache.
Preclinical data demonstrated that continued use of ubrogepant does not appear to produce early or latent trigeminal sensory sensitization. Meanwhile, rimegepant, when used every other day, and as needed for acute treatment of migraine in individuals suffering from moderate-to-high frequency episodic migraine, resulted in reductions in monthly migraine days. The preventive effects appear to be rapid and sustained. And in a phase 3 trial, atogepant demonstrated efficacy at doses of 10 mg, 30 mg, and 60 mg twice a day, compared with placebo over 12 weeks.
It is important to note that the link between the gepants and medication overuse and medication overuse headache have not yet been studied. Still, it is encouraging to see that migraine frequency improves and medication use days are reduced when gepants are taken preventively. Thus, gepants could emerge as a preferred approach for acute or preventive treatment in individuals who have or are at risk of developing medication overuse headache.
New targeted treatments are major advances for HER2-positive breast cancer
Before 2001, HER2/neu-positive breast cancer (HER2+) was one of the most dreaded diagnoses a woman could face, as treatment was largely ineffective. The discovery of trastuzumab changed that dramatically.

Over the next 20 years, two additional HER2-targeted therapies – lapatinib and trastuzumab emtansine (TDM-1) – earned approval from the Food and Drug Administration for selected patients with early and late HER2+ breast cancer.
Since 2019, four additional HER2-targeted therapies have been approved by the FDA for HER2+ metastatic breast cancer (MBC), changing the treatment paradigm for those patients substantially.
The new agents are especially useful in certain patient populations. The agents offer the promise of improved survival for patients with recurrent metastatic disease and the potential for further reductions in relapse rates in earlier settings.
Trastuzumab deruxtecan
Trastuzumab deruxtecan is an antibody-drug conjugate that links three components: an anti-HER2 monoclonal antibody, a highly potent topoisomerase I inhibitor payload, and a tetrapeptide-based cleavable linker.
Trastuzumab deruxtecan has a high drug-to-antibody ratio. A membrane-permeable payload offers the potential for activity against adjacent HER2-negative cells in heterogeneous tumors. It has a long half-life (6 days).
Trastuzumab deruxtecan received accelerated approval from the FDA in December 2019 to treat patients with HER2+ MBC who have received two or more prior HER2-targeted regimens, based on the results of the DESTINY-Breast 01 trial.
DESTINY-Breast 01 trial
In the phase 2 DESTINY-Breast 01 trial, 184 patients with a median of six previous treatments received trastuzumab deruxtecan (5.4 mg/kg) intravenously every 21 days. There were 24 patients with treated, asymptomatic brain metastases who participated. Patients with untreated or symptomatic brain metastases were excluded.
Overall, a response to therapy was reported in 112 patients (60.9%), with 6.0% complete and 54.9% partial responses. Most of the patients for whom both baseline and postbaseline data were available had a reduction in tumor size.
The median time until response was 1.6 months, an interval that corresponded to the time until the first scheduled imaging. Three patients (1.6%) had progressive disease, and two patients (1.1%) could not be evaluated.
The median duration of follow-up was 11.1 months, and the median response duration was 14.8 months.
The median progression-free survival (PFS) was 16.4 months, and the median overall survival (OS) was not reached. The median PFS in the patients with brain involvement was 18.1 months.
The most common adverse events of grade 3 or higher were a decreased neutrophil count (20.7%), anemia (8.7%), and nausea (7.6%). Most concerning was that trastuzumab deruxtecan was associated with interstitial lung disease in 13.6% of patients.
Tucatinib
Tucatinib is an oral, highly selective HER2 tyrosine kinase inhibitor (TKI). In April 2020, it was approved by the FDA, in combination with trastuzumab and capecitabine, for adult patients with advanced unresectable or metastatic HER2+ breast cancer who have received one or more prior anti-HER2–based regimens for MBC. The approval included patients with brain metastases.
The recommended tucatinib dose is 300 mg orally twice a day in combination with trastuzumab (at the standard dose) and capecitabine (1,000 mg/m2 given orally twice daily on days 1-14) on a 21-day cycle, until disease progression or unacceptable toxicity.
HER2CLIMB trial
The study that led to the approval of tucatinib was the HER2CLIMB trial. The trial enrolled 612 HER2+ MBC patients who had prior treatment with trastuzumab, pertuzumab, and T-DM1. Patients had received a median of 4 (range, 2-17) prior lines of HER2-targeted therapy.
The patients were randomized 2:1 to receive trastuzumab plus capecitabine and either tucatinib or an identical placebo twice daily.
The primary endpoint was PFS, evaluated in the initial 480 randomized patients. The median PFS was 7.8 months in the tucatinib arm and 5.6 months in the control arm (hazard ratio, 0.54; 95% confidence interval, 0.42-0.71; P < .001).
The confirmed overall response rate for patients with measurable disease was 40.6% in the tucatinib arm and 22.8% in the control arm (P = .001). The proportion of patients still in response at 12 months was 33.1% and 12.3%, respectively.
The median OS was 21.9 months in the tucatinib arm and 17.4 months in the placebo arm (HR, 0.66; 95% CI, 0.50-0.88; P = .005). At 24 months, 44.9% and 26.6% of patients, respectively, were still alive.
The most common grade 3 or higher adverse events (in the tucatinib and placebo arms, respectively) were palmar-plantar erythrodysesthesia syndrome (13.1% vs. 9.1%), diarrhea (12.9% vs. 8.6%), elevations in ALT and AST (approximately 5% vs. 0.5% for each), and fatigue (4.7% vs. 4.1%).
Tucatinib in patients with brain involvement
A unique feature of the HER2CLIMB study was that patients with MBC and untreated, symptomatic brain metastases were eligible. Patients with active, untreated central nervous system disease are excluded from virtually all other trials, especially drug-approval trials.
There were 291 patients with brain metastases in HER2CLIMB, 198 (48%) in the tucatinib arm and 93 (46%) in the control arm.
The risk of intracranial progression or death was reduced by 68% in the tucatinib arm (HR, 0.32; 95% CI, 0.22 to 0.48; P < .0001).
The 1-year CNS-PFS rate was 40.2% in the tucatinib arm and 0% in the placebo arm. The median duration of CNS-PFS was 9.9 months and 4.2 months, respectively.
The risk of death was reduced by 42% in the tucatinib arm (HR, 0.58; 95% CI, 0.40-0.85; P = .005). The median OS was 18.1 months and 12.0 months, respectively.
There were more objective responses in the brain with tucatinib (47.3%) than with placebo (20.0%; P = .03). The median duration of response was 6.8 months and 3.0 months, respectively.
Particularly because of its CNS activity and lack of serious, long-term toxicity, tucatinib combination therapy represents an attractive new option for patients with HER2+ MBC.
Neratinib
Neratinib is an irreversible pan-HER TKI that was approved by the FDA in July 2017 for extended adjuvant therapy in patients with early-stage HER2+ breast cancer, following the use of trastuzumab-based therapy.
Long-term results of the ExteNet study led to the approval for use as extended adjuvant therapy.
In February 2020, neratinib was FDA approved in combination with capecitabine for patients with HER2+ MBC after two or more prior anti-HER2–based regimens. The more recent FDA approval was based on results of the NALA trial.
NALA trial
The phase 3 NALA trial included 621 patients with HER2+ MBC who had received at least two prior anti-HER2 based regimens.
Patients were randomized 1:1 to receive neratinib at 240 mg orally once daily on days 1-21 with capecitabine at 750 mg/m2 orally twice daily on days 1-14 or lapatinib at 1,250 mg orally once daily on days 1-21 with capecitabine at 1,000 mg/m2 orally twice daily on days 1-14 for each 21-day cycle. Patients were treated until disease progression or unacceptable toxicity.
The primary endpoints were PFS and OS by blinded, independent, central review.
The median PFS was 5.6 months in the neratinib arm and 5.5 months in the lapatinib arm (HR, 0.76; 95% CI, 0.63-0.93; P = .0059). The PFS rate at 12 months was 28.8% and 14.8%, respectively.
The median OS was 21.0 months in the neratinib arm and 18.7 months in the lapatinib arm (HR, 0.88; 95% CI, 0.72-1.07; P = .2086). The ORR was 32.8% and 26.7%, respectively. The median response duration was 8.5 months and 5.6 months, respectively.
Fewer interventions for CNS disease were required in the neratinib arm than in the lapatinib arm (cumulative incidence, 22.8% vs. 29.2%; P = .043).
The most frequently reported grade 3-4 adverse reactions for the neratinib combination were diarrhea, nausea, vomiting, fatigue, and decreased appetite.
Grade 3 diarrhea occurred in 24.4% of those in the neratinib arm and 12.5% of those in the lapatinib arm. Antidiarrheal medication was used by 98.3% of patients receiving neratinib and 62.1% of patients receiving lapatinib.
Margetuximab-cmkb
Margetuximab is a chimeric Fc-engineered anti-HER2 monoclonal antibody that targets the same epitope as trastuzumab and exerts similar antiproliferative effects.
Compared with trastuzumab, margetuximab has higher affinity for both 158V (high-binding) and 158F (low-binding) alleles of the activating Fc receptor, CD16A. As a result, margetuximab enhances innate immunity, including CD16A-mediated antibody-dependent cellular cytotoxicity, more effectively than trastuzumab. Margetuximab also potentiates adaptive immunity, including enhanced clonality of the T-cell repertoire and induction of HER2-specific T- and B-cell responses.
In December 2020, margetuximab, in combination with chemotherapy, was approved by the FDA for patients with HER2+ MBC after two or more prior anti-HER2 regimens, at least one of which was for metastatic disease. The approved dose is 15 mg/kg IV every 3 weeks.
The study that led to margetuximab’s approval was the phase 3 SOPHIA trial.
SOPHIA trial
SOPHIA was a randomized trial of 536 patients with HER2+ MBC who had received prior treatment with other anti-HER2 therapies, including one to three lines of therapy for MBC.
Patients were randomly assigned 1:1 to receive margetuximab plus chemotherapy or trastuzumab plus chemotherapy. Assignment was stratified by chemotherapy choice (capecitabine, eribulin, gemcitabine, or vinorelbine), the number of previous lines of therapy for MBC, and disease extent.
Co–primary outcome measures were PFS by blinded, independent, central review and OS.
At the second interim analysis, the median PFS was 5.8 months in the margetuximab arm and 4.9 months in the trastuzumab arm (HR, 0.76; 95% CI, 0.59-0.98; P = .033). Results were more impressive in patients with CD16A genotypes containing a 158F allele. In this group, the median PFS was 6.9 months with margetuximab and 5.1 months with trastuzumab (HR, 0.68, 95% CI, 0.52-0.90; P = .005).
At the second interim analysis, the median OS was 21.6 months in the margetuximab arm and 19.8 months in the trastuzumab arm (HR, 0.89; 95% CI, 0.69-1.13; P = .33).
Subgroup data showed no differences in OS between the two arms for any subgroup except HER2+ MBC patients with an IHC score of 2 or higher. This is consistent with the postulated mechanism of action of margetuximab.
The confirmed ORR was 25% in the margetuximab arm and 14% in the trastuzumab arm, with similar durations of response between the study arms.
The most common adverse events in both arms (≥20%), regardless of causality, were fatigue, nausea, diarrhea, and neutropenia. Vomiting was common in the margetuximab arm, and anemia was common in the trastuzumab arm.
Grade 3 or higher adverse events occurred in 53.8% of patients receiving margetuximab and 52.6% of those receiving trastuzumab.
In view of margetuximab’s modest benefits in the SOPHIA trial, the ultimate role for margetuximab in HER2+ MBC may be restricted to patients with the CD16A-158F allele. A neoadjuvant trial is planned in that population.
Take-home messages
There are legitimate arguments regarding whether curing MBC is within reach for certain patient subsets, but there is no argument about whether the outlook for patients with HER2+ MBC has improved dramatically in recent years; it has.
The approval of four unique, new agents for the treatment of women with HER2+ MBC in relapse provides further improvements in outcome for these patients and distinctly different opportunities for tailoring treatment to the special circumstances of each patient (e.g., whether brain metastases are present, desire for oral therapy, comorbidities, experience with prior chemotherapy, etc).
When considered along with the potential for incorporating these drugs in earlier settings in well-designed clinical trials, these new drugs offer great promise to a group of patients who faced a dismal outcome just 2 decades ago.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Before 2001, HER2/neu-positive breast cancer (HER2+) was one of the most dreaded diagnoses a woman could face, as treatment was largely ineffective. The discovery of trastuzumab changed that dramatically.
Over the next 20 years, two additional HER2-targeted therapies – lapatinib and trastuzumab emtansine (TDM-1) – earned approval from the Food and Drug Administration for selected patients with early and late HER2+ breast cancer.
Since 2019, four additional HER2-targeted therapies have been approved by the FDA for HER2+ metastatic breast cancer (MBC), changing the treatment paradigm for those patients substantially.
The new agents are especially useful in certain patient populations. The agents offer the promise of improved survival for patients with recurrent metastatic disease and the potential for further reductions in relapse rates in earlier settings.
Trastuzumab deruxtecan
Trastuzumab deruxtecan is an antibody-drug conjugate that links three components: an anti-HER2 monoclonal antibody, a highly potent topoisomerase I inhibitor payload, and a tetrapeptide-based cleavable linker.
Trastuzumab deruxtecan has a high drug-to-antibody ratio. A membrane-permeable payload offers the potential for activity against adjacent HER2-negative cells in heterogeneous tumors. It has a long half-life (6 days).
Trastuzumab deruxtecan received accelerated approval from the FDA in December 2019 to treat patients with HER2+ MBC who have received two or more prior HER2-targeted regimens, based on the results of the DESTINY-Breast 01 trial.
DESTINY-Breast 01 trial
In the phase 2 DESTINY-Breast 01 trial, 184 patients with a median of six previous treatments received trastuzumab deruxtecan (5.4 mg/kg) intravenously every 21 days. There were 24 patients with treated, asymptomatic brain metastases who participated. Patients with untreated or symptomatic brain metastases were excluded.
Overall, a response to therapy was reported in 112 patients (60.9%), with 6.0% complete and 54.9% partial responses. Most of the patients for whom both baseline and postbaseline data were available had a reduction in tumor size.
The median time until response was 1.6 months, an interval that corresponded to the time until the first scheduled imaging. Three patients (1.6%) had progressive disease, and two patients (1.1%) could not be evaluated.
The median duration of follow-up was 11.1 months, and the median response duration was 14.8 months.
The median progression-free survival (PFS) was 16.4 months, and the median overall survival (OS) was not reached. The median PFS in the patients with brain involvement was 18.1 months.
The most common adverse events of grade 3 or higher were a decreased neutrophil count (20.7%), anemia (8.7%), and nausea (7.6%). Most concerning was that trastuzumab deruxtecan was associated with interstitial lung disease in 13.6% of patients.
Tucatinib
Tucatinib is an oral, highly selective HER2 tyrosine kinase inhibitor (TKI). In April 2020, it was approved by the FDA, in combination with trastuzumab and capecitabine, for adult patients with advanced unresectable or metastatic HER2+ breast cancer who have received one or more prior anti-HER2–based regimens for MBC. The approval included patients with brain metastases.
The recommended tucatinib dose is 300 mg orally twice a day in combination with trastuzumab (at the standard dose) and capecitabine (1,000 mg/m2 given orally twice daily on days 1-14) on a 21-day cycle, until disease progression or unacceptable toxicity.
HER2CLIMB trial
The study that led to the approval of tucatinib was the HER2CLIMB trial. The trial enrolled 612 HER2+ MBC patients who had prior treatment with trastuzumab, pertuzumab, and T-DM1. Patients had received a median of 4 (range, 2-17) prior lines of HER2-targeted therapy.
The patients were randomized 2:1 to receive trastuzumab plus capecitabine and either tucatinib or an identical placebo twice daily.
The primary endpoint was PFS, evaluated in the initial 480 randomized patients. The median PFS was 7.8 months in the tucatinib arm and 5.6 months in the control arm (hazard ratio, 0.54; 95% confidence interval, 0.42-0.71; P < .001).
The confirmed overall response rate for patients with measurable disease was 40.6% in the tucatinib arm and 22.8% in the control arm (P = .001). The proportion of patients still in response at 12 months was 33.1% and 12.3%, respectively.
The median OS was 21.9 months in the tucatinib arm and 17.4 months in the placebo arm (HR, 0.66; 95% CI, 0.50-0.88; P = .005). At 24 months, 44.9% and 26.6% of patients, respectively, were still alive.
The most common grade 3 or higher adverse events (in the tucatinib and placebo arms, respectively) were palmar-plantar erythrodysesthesia syndrome (13.1% vs. 9.1%), diarrhea (12.9% vs. 8.6%), elevations in ALT and AST (approximately 5% vs. 0.5% for each), and fatigue (4.7% vs. 4.1%).
Tucatinib in patients with brain involvement
A unique feature of the HER2CLIMB study was that patients with MBC and untreated, symptomatic brain metastases were eligible. Patients with active, untreated central nervous system disease are excluded from virtually all other trials, especially drug-approval trials.
There were 291 patients with brain metastases in HER2CLIMB, 198 (48%) in the tucatinib arm and 93 (46%) in the control arm.
The risk of intracranial progression or death was reduced by 68% in the tucatinib arm (HR, 0.32; 95% CI, 0.22 to 0.48; P < .0001).
The 1-year CNS-PFS rate was 40.2% in the tucatinib arm and 0% in the placebo arm. The median duration of CNS-PFS was 9.9 months and 4.2 months, respectively.
The risk of death was reduced by 42% in the tucatinib arm (HR, 0.58; 95% CI, 0.40-0.85; P = .005). The median OS was 18.1 months and 12.0 months, respectively.
There were more objective responses in the brain with tucatinib (47.3%) than with placebo (20.0%; P = .03). The median duration of response was 6.8 months and 3.0 months, respectively.
Particularly because of its CNS activity and lack of serious, long-term toxicity, tucatinib combination therapy represents an attractive new option for patients with HER2+ MBC.
Neratinib
Neratinib is an irreversible pan-HER TKI that was approved by the FDA in July 2017 for extended adjuvant therapy in patients with early-stage HER2+ breast cancer, following the use of trastuzumab-based therapy.
Long-term results of the ExteNet study led to the approval for use as extended adjuvant therapy.
In February 2020, neratinib was FDA approved in combination with capecitabine for patients with HER2+ MBC after two or more prior anti-HER2–based regimens. The more recent FDA approval was based on results of the NALA trial.
NALA trial
The phase 3 NALA trial included 621 patients with HER2+ MBC who had received at least two prior anti-HER2 based regimens.
Patients were randomized 1:1 to receive neratinib at 240 mg orally once daily on days 1-21 with capecitabine at 750 mg/m2 orally twice daily on days 1-14 or lapatinib at 1,250 mg orally once daily on days 1-21 with capecitabine at 1,000 mg/m2 orally twice daily on days 1-14 for each 21-day cycle. Patients were treated until disease progression or unacceptable toxicity.
The primary endpoints were PFS and OS by blinded, independent, central review.
The median PFS was 5.6 months in the neratinib arm and 5.5 months in the lapatinib arm (HR, 0.76; 95% CI, 0.63-0.93; P = .0059). The PFS rate at 12 months was 28.8% and 14.8%, respectively.
The median OS was 21.0 months in the neratinib arm and 18.7 months in the lapatinib arm (HR, 0.88; 95% CI, 0.72-1.07; P = .2086). The ORR was 32.8% and 26.7%, respectively. The median response duration was 8.5 months and 5.6 months, respectively.
Fewer interventions for CNS disease were required in the neratinib arm than in the lapatinib arm (cumulative incidence, 22.8% vs. 29.2%; P = .043).
The most frequently reported grade 3-4 adverse reactions for the neratinib combination were diarrhea, nausea, vomiting, fatigue, and decreased appetite.
Grade 3 diarrhea occurred in 24.4% of those in the neratinib arm and 12.5% of those in the lapatinib arm. Antidiarrheal medication was used by 98.3% of patients receiving neratinib and 62.1% of patients receiving lapatinib.
Margetuximab-cmkb
Margetuximab is a chimeric Fc-engineered anti-HER2 monoclonal antibody that targets the same epitope as trastuzumab and exerts similar antiproliferative effects.
Compared with trastuzumab, margetuximab has higher affinity for both 158V (high-binding) and 158F (low-binding) alleles of the activating Fc receptor, CD16A. As a result, margetuximab enhances innate immunity, including CD16A-mediated antibody-dependent cellular cytotoxicity, more effectively than trastuzumab. Margetuximab also potentiates adaptive immunity, including enhanced clonality of the T-cell repertoire and induction of HER2-specific T- and B-cell responses.
In December 2020, margetuximab, in combination with chemotherapy, was approved by the FDA for patients with HER2+ MBC after two or more prior anti-HER2 regimens, at least one of which was for metastatic disease. The approved dose is 15 mg/kg IV every 3 weeks.
The study that led to margetuximab’s approval was the phase 3 SOPHIA trial.
SOPHIA trial
SOPHIA was a randomized trial of 536 patients with HER2+ MBC who had received prior treatment with other anti-HER2 therapies, including one to three lines of therapy for MBC.
Patients were randomly assigned 1:1 to receive margetuximab plus chemotherapy or trastuzumab plus chemotherapy. Assignment was stratified by chemotherapy choice (capecitabine, eribulin, gemcitabine, or vinorelbine), the number of previous lines of therapy for MBC, and disease extent.
Co–primary outcome measures were PFS by blinded, independent, central review and OS.
At the second interim analysis, the median PFS was 5.8 months in the margetuximab arm and 4.9 months in the trastuzumab arm (HR, 0.76; 95% CI, 0.59-0.98; P = .033). Results were more impressive in patients with CD16A genotypes containing a 158F allele. In this group, the median PFS was 6.9 months with margetuximab and 5.1 months with trastuzumab (HR, 0.68, 95% CI, 0.52-0.90; P = .005).
At the second interim analysis, the median OS was 21.6 months in the margetuximab arm and 19.8 months in the trastuzumab arm (HR, 0.89; 95% CI, 0.69-1.13; P = .33).
Subgroup data showed no differences in OS between the two arms for any subgroup except HER2+ MBC patients with an IHC score of 2 or higher. This is consistent with the postulated mechanism of action of margetuximab.
The confirmed ORR was 25% in the margetuximab arm and 14% in the trastuzumab arm, with similar durations of response between the study arms.
The most common adverse events in both arms (≥20%), regardless of causality, were fatigue, nausea, diarrhea, and neutropenia. Vomiting was common in the margetuximab arm, and anemia was common in the trastuzumab arm.
Grade 3 or higher adverse events occurred in 53.8% of patients receiving margetuximab and 52.6% of those receiving trastuzumab.
In view of margetuximab’s modest benefits in the SOPHIA trial, the ultimate role for margetuximab in HER2+ MBC may be restricted to patients with the CD16A-158F allele. A neoadjuvant trial is planned in that population.
Take-home messages
There are legitimate arguments regarding whether curing MBC is within reach for certain patient subsets, but there is no argument about whether the outlook for patients with HER2+ MBC has improved dramatically in recent years; it has.
The approval of four unique, new agents for the treatment of women with HER2+ MBC in relapse provides further improvements in outcome for these patients and distinctly different opportunities for tailoring treatment to the special circumstances of each patient (e.g., whether brain metastases are present, desire for oral therapy, comorbidities, experience with prior chemotherapy, etc).
When considered along with the potential for incorporating these drugs in earlier settings in well-designed clinical trials, these new drugs offer great promise to a group of patients who faced a dismal outcome just 2 decades ago.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Before 2001, HER2/neu-positive breast cancer (HER2+) was one of the most dreaded diagnoses a woman could face, as treatment was largely ineffective. The discovery of trastuzumab changed that dramatically.
Over the next 20 years, two additional HER2-targeted therapies – lapatinib and trastuzumab emtansine (TDM-1) – earned approval from the Food and Drug Administration for selected patients with early and late HER2+ breast cancer.
Since 2019, four additional HER2-targeted therapies have been approved by the FDA for HER2+ metastatic breast cancer (MBC), changing the treatment paradigm for those patients substantially.
The new agents are especially useful in certain patient populations. The agents offer the promise of improved survival for patients with recurrent metastatic disease and the potential for further reductions in relapse rates in earlier settings.
Trastuzumab deruxtecan
Trastuzumab deruxtecan is an antibody-drug conjugate that links three components: an anti-HER2 monoclonal antibody, a highly potent topoisomerase I inhibitor payload, and a tetrapeptide-based cleavable linker.
Trastuzumab deruxtecan has a high drug-to-antibody ratio. A membrane-permeable payload offers the potential for activity against adjacent HER2-negative cells in heterogeneous tumors. It has a long half-life (6 days).
Trastuzumab deruxtecan received accelerated approval from the FDA in December 2019 to treat patients with HER2+ MBC who have received two or more prior HER2-targeted regimens, based on the results of the DESTINY-Breast 01 trial.
DESTINY-Breast 01 trial
In the phase 2 DESTINY-Breast 01 trial, 184 patients with a median of six previous treatments received trastuzumab deruxtecan (5.4 mg/kg) intravenously every 21 days. There were 24 patients with treated, asymptomatic brain metastases who participated. Patients with untreated or symptomatic brain metastases were excluded.
Overall, a response to therapy was reported in 112 patients (60.9%), with 6.0% complete and 54.9% partial responses. Most of the patients for whom both baseline and postbaseline data were available had a reduction in tumor size.
The median time until response was 1.6 months, an interval that corresponded to the time until the first scheduled imaging. Three patients (1.6%) had progressive disease, and two patients (1.1%) could not be evaluated.
The median duration of follow-up was 11.1 months, and the median response duration was 14.8 months.
The median progression-free survival (PFS) was 16.4 months, and the median overall survival (OS) was not reached. The median PFS in the patients with brain involvement was 18.1 months.
The most common adverse events of grade 3 or higher were a decreased neutrophil count (20.7%), anemia (8.7%), and nausea (7.6%). Most concerning was that trastuzumab deruxtecan was associated with interstitial lung disease in 13.6% of patients.
Tucatinib
Tucatinib is an oral, highly selective HER2 tyrosine kinase inhibitor (TKI). In April 2020, it was approved by the FDA, in combination with trastuzumab and capecitabine, for adult patients with advanced unresectable or metastatic HER2+ breast cancer who have received one or more prior anti-HER2–based regimens for MBC. The approval included patients with brain metastases.
The recommended tucatinib dose is 300 mg orally twice a day in combination with trastuzumab (at the standard dose) and capecitabine (1,000 mg/m2 given orally twice daily on days 1-14) on a 21-day cycle, until disease progression or unacceptable toxicity.
HER2CLIMB trial
The study that led to the approval of tucatinib was the HER2CLIMB trial. The trial enrolled 612 HER2+ MBC patients who had prior treatment with trastuzumab, pertuzumab, and T-DM1. Patients had received a median of 4 (range, 2-17) prior lines of HER2-targeted therapy.
The patients were randomized 2:1 to receive trastuzumab plus capecitabine and either tucatinib or an identical placebo twice daily.
The primary endpoint was PFS, evaluated in the initial 480 randomized patients. The median PFS was 7.8 months in the tucatinib arm and 5.6 months in the control arm (hazard ratio, 0.54; 95% confidence interval, 0.42-0.71; P < .001).
The confirmed overall response rate for patients with measurable disease was 40.6% in the tucatinib arm and 22.8% in the control arm (P = .001). The proportion of patients still in response at 12 months was 33.1% and 12.3%, respectively.
The median OS was 21.9 months in the tucatinib arm and 17.4 months in the placebo arm (HR, 0.66; 95% CI, 0.50-0.88; P = .005). At 24 months, 44.9% and 26.6% of patients, respectively, were still alive.
The most common grade 3 or higher adverse events (in the tucatinib and placebo arms, respectively) were palmar-plantar erythrodysesthesia syndrome (13.1% vs. 9.1%), diarrhea (12.9% vs. 8.6%), elevations in ALT and AST (approximately 5% vs. 0.5% for each), and fatigue (4.7% vs. 4.1%).
Tucatinib in patients with brain involvement
A unique feature of the HER2CLIMB study was that patients with MBC and untreated, symptomatic brain metastases were eligible. Patients with active, untreated central nervous system disease are excluded from virtually all other trials, especially drug-approval trials.
There were 291 patients with brain metastases in HER2CLIMB, 198 (48%) in the tucatinib arm and 93 (46%) in the control arm.
The risk of intracranial progression or death was reduced by 68% in the tucatinib arm (HR, 0.32; 95% CI, 0.22 to 0.48; P < .0001).
The 1-year CNS-PFS rate was 40.2% in the tucatinib arm and 0% in the placebo arm. The median duration of CNS-PFS was 9.9 months and 4.2 months, respectively.
The risk of death was reduced by 42% in the tucatinib arm (HR, 0.58; 95% CI, 0.40-0.85; P = .005). The median OS was 18.1 months and 12.0 months, respectively.
There were more objective responses in the brain with tucatinib (47.3%) than with placebo (20.0%; P = .03). The median duration of response was 6.8 months and 3.0 months, respectively.
Particularly because of its CNS activity and lack of serious, long-term toxicity, tucatinib combination therapy represents an attractive new option for patients with HER2+ MBC.
Neratinib
Neratinib is an irreversible pan-HER TKI that was approved by the FDA in July 2017 for extended adjuvant therapy in patients with early-stage HER2+ breast cancer, following the use of trastuzumab-based therapy.
Long-term results of the ExteNet study led to the approval for use as extended adjuvant therapy.
In February 2020, neratinib was FDA approved in combination with capecitabine for patients with HER2+ MBC after two or more prior anti-HER2–based regimens. The more recent FDA approval was based on results of the NALA trial.
NALA trial
The phase 3 NALA trial included 621 patients with HER2+ MBC who had received at least two prior anti-HER2 based regimens.
Patients were randomized 1:1 to receive neratinib at 240 mg orally once daily on days 1-21 with capecitabine at 750 mg/m2 orally twice daily on days 1-14 or lapatinib at 1,250 mg orally once daily on days 1-21 with capecitabine at 1,000 mg/m2 orally twice daily on days 1-14 for each 21-day cycle. Patients were treated until disease progression or unacceptable toxicity.
The primary endpoints were PFS and OS by blinded, independent, central review.
The median PFS was 5.6 months in the neratinib arm and 5.5 months in the lapatinib arm (HR, 0.76; 95% CI, 0.63-0.93; P = .0059). The PFS rate at 12 months was 28.8% and 14.8%, respectively.
The median OS was 21.0 months in the neratinib arm and 18.7 months in the lapatinib arm (HR, 0.88; 95% CI, 0.72-1.07; P = .2086). The ORR was 32.8% and 26.7%, respectively. The median response duration was 8.5 months and 5.6 months, respectively.
Fewer interventions for CNS disease were required in the neratinib arm than in the lapatinib arm (cumulative incidence, 22.8% vs. 29.2%; P = .043).
The most frequently reported grade 3-4 adverse reactions for the neratinib combination were diarrhea, nausea, vomiting, fatigue, and decreased appetite.
Grade 3 diarrhea occurred in 24.4% of those in the neratinib arm and 12.5% of those in the lapatinib arm. Antidiarrheal medication was used by 98.3% of patients receiving neratinib and 62.1% of patients receiving lapatinib.
Margetuximab-cmkb
Margetuximab is a chimeric Fc-engineered anti-HER2 monoclonal antibody that targets the same epitope as trastuzumab and exerts similar antiproliferative effects.
Compared with trastuzumab, margetuximab has higher affinity for both 158V (high-binding) and 158F (low-binding) alleles of the activating Fc receptor, CD16A. As a result, margetuximab enhances innate immunity, including CD16A-mediated antibody-dependent cellular cytotoxicity, more effectively than trastuzumab. Margetuximab also potentiates adaptive immunity, including enhanced clonality of the T-cell repertoire and induction of HER2-specific T- and B-cell responses.
In December 2020, margetuximab, in combination with chemotherapy, was approved by the FDA for patients with HER2+ MBC after two or more prior anti-HER2 regimens, at least one of which was for metastatic disease. The approved dose is 15 mg/kg IV every 3 weeks.
The study that led to margetuximab’s approval was the phase 3 SOPHIA trial.
SOPHIA trial
SOPHIA was a randomized trial of 536 patients with HER2+ MBC who had received prior treatment with other anti-HER2 therapies, including one to three lines of therapy for MBC.
Patients were randomly assigned 1:1 to receive margetuximab plus chemotherapy or trastuzumab plus chemotherapy. Assignment was stratified by chemotherapy choice (capecitabine, eribulin, gemcitabine, or vinorelbine), the number of previous lines of therapy for MBC, and disease extent.
Co–primary outcome measures were PFS by blinded, independent, central review and OS.
At the second interim analysis, the median PFS was 5.8 months in the margetuximab arm and 4.9 months in the trastuzumab arm (HR, 0.76; 95% CI, 0.59-0.98; P = .033). Results were more impressive in patients with CD16A genotypes containing a 158F allele. In this group, the median PFS was 6.9 months with margetuximab and 5.1 months with trastuzumab (HR, 0.68, 95% CI, 0.52-0.90; P = .005).
At the second interim analysis, the median OS was 21.6 months in the margetuximab arm and 19.8 months in the trastuzumab arm (HR, 0.89; 95% CI, 0.69-1.13; P = .33).
Subgroup data showed no differences in OS between the two arms for any subgroup except HER2+ MBC patients with an IHC score of 2 or higher. This is consistent with the postulated mechanism of action of margetuximab.
The confirmed ORR was 25% in the margetuximab arm and 14% in the trastuzumab arm, with similar durations of response between the study arms.
The most common adverse events in both arms (≥20%), regardless of causality, were fatigue, nausea, diarrhea, and neutropenia. Vomiting was common in the margetuximab arm, and anemia was common in the trastuzumab arm.
Grade 3 or higher adverse events occurred in 53.8% of patients receiving margetuximab and 52.6% of those receiving trastuzumab.
In view of margetuximab’s modest benefits in the SOPHIA trial, the ultimate role for margetuximab in HER2+ MBC may be restricted to patients with the CD16A-158F allele. A neoadjuvant trial is planned in that population.
Take-home messages
There are legitimate arguments regarding whether curing MBC is within reach for certain patient subsets, but there is no argument about whether the outlook for patients with HER2+ MBC has improved dramatically in recent years; it has.
The approval of four unique, new agents for the treatment of women with HER2+ MBC in relapse provides further improvements in outcome for these patients and distinctly different opportunities for tailoring treatment to the special circumstances of each patient (e.g., whether brain metastases are present, desire for oral therapy, comorbidities, experience with prior chemotherapy, etc).
When considered along with the potential for incorporating these drugs in earlier settings in well-designed clinical trials, these new drugs offer great promise to a group of patients who faced a dismal outcome just 2 decades ago.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Risk factors identified for late seizure relapse after epilepsy surgery
according to a new study on the factors most associated with seizure recurrence in drug-resistant epilepsy.
“As our study analyzed late seizure relapse, our results are not applicable for short‐term seizure control. Vice versa, results for short‐term outcomes should not be transferred to long‐term outcomes,” Stephan Petrik of the Epilepsy Center at the University of Freiburg (Germany) and colleagues wrote. The study was published in the May 2021 issue of Epilepsia.
To assess the variables that increase risk of late seizure recurrence following surgery, the researchers retrospectively studied the medical records of patients who underwent resective epilepsy surgery at the University Hospital Freiburg (Germany) between 1999 and 2015. Of the 1,278 initial patients, a group of 99 participants (7.7%) with seizure relapses after at least 2 years of complete seizure freedom were matched with controls experiencing long-term seizure freedom. The two groups had similar mean durations of epilepsy from onset to surgery: 13.9 years in the relapse group and 13.0 years in the control group.
The mean follow-up was 9.7 years (standard deviation, 4.0; range, 2.9-18.5) in the relapse group and 8.2 years (SD, 3.5; range, 2.2-18.3) in the control group. The mean time to late seizure recurrence was 56.6 months, and two-thirds of patients relapsed in the 5 years after surgery. Twenty of the relapse patients only experienced a single seizure, and 41% of the patients who reported more than one seizure had a frequency of less than one per month.
The type of resection had no discernible impact on outcomes, although anterior temporal lobe resection did trend toward being associated with recurrence (odds ratio, 2.7; 95% confidence interval, 0.93-8.89; P = .06). Incomplete resection was significantly associated with late relapse but did not seem to affect timing: the mean duration of seizure freedom was 56.5 months with complete resection and 58.5 months with incomplete resection (P = .62). Additional preoperative PET scans were performed on 45% of patients in the relapse group, compared with 29% in the control group.
After multivariate analysis, predictors for late relapse included incomplete resection (OR, 3.81; 95% CI, 1.79-8.53; P < .001); the existence of additional, potentially epileptogenic lesions in the contralateral hemisphere on presurgical MRI (OR, 3.36; 95% CI, 1.18-10.62; P = .03); epilepsy onset during the first year of life (OR, 4.24; 95% CI, 1.4-15.89; P = .02); and preoperative PET scans being performed (OR, 2.47; 95% CI, 1.25-4.97; P = .01). Though use of preoperative and postoperative antiepileptic drugs (AEDs) was higher in the relapse group, along with complete withdrawal being more common in the control group (68%, compared with 51%), neither was deemed significant in multivariate analysis.
What to do about seizure relapse risk factors
“This is one of the best analyses of the factors that contribute to late seizure relapse,” Gregory K. Bergey, MD, director of the Johns Hopkins Epilepsy Center in Baltimore, said in an interview. “Am I surprised by their results? Not necessarily.”
What did jump out, he said, was AED use not being a predictor of recurrence, as well as all the patients with late relapse having lesional epilepsy. “As they point out, you can have relapse with nonlesional epilepsy, but very often it happens in the first year or 2. If someone is 2 years out and doesn’t have a lesion, they’re probably more likely to remain seizure free.”
Despite the researchers’ comprehensive review of risk factors, the question remains: What to do with this information?
“They’ve done a very good job of identifying that 7.7% of 1,200 who are at risk of a late relapse,” he said. “Now, take those patients with high-risk factors and launch a trial where you keep medicines the same or do something that would alter that outcome.”
“The problem is,” he added, “that’s a 10-year study. It’s easy for me to sit here and call for one of those. But still, as valuable as this was, it’s a retrospective study. Now you have to say, what are the implications of this? What can we do in the prospective fashion?”
The authors acknowledged their study’s other limitations, including a lack of information on the reasons for an incomplete resection, a notable decrease in follow-up visits more than 5 years after surgery, and potential selection bias. They added, however, that “matching by age at surgery, gender, and time to relapse/last follow‐up” should have helped reduce any significant bias.
No potential conflicts of interest were disclosed.
according to a new study on the factors most associated with seizure recurrence in drug-resistant epilepsy.
“As our study analyzed late seizure relapse, our results are not applicable for short‐term seizure control. Vice versa, results for short‐term outcomes should not be transferred to long‐term outcomes,” Stephan Petrik of the Epilepsy Center at the University of Freiburg (Germany) and colleagues wrote. The study was published in the May 2021 issue of Epilepsia.
To assess the variables that increase risk of late seizure recurrence following surgery, the researchers retrospectively studied the medical records of patients who underwent resective epilepsy surgery at the University Hospital Freiburg (Germany) between 1999 and 2015. Of the 1,278 initial patients, a group of 99 participants (7.7%) with seizure relapses after at least 2 years of complete seizure freedom were matched with controls experiencing long-term seizure freedom. The two groups had similar mean durations of epilepsy from onset to surgery: 13.9 years in the relapse group and 13.0 years in the control group.
The mean follow-up was 9.7 years (standard deviation, 4.0; range, 2.9-18.5) in the relapse group and 8.2 years (SD, 3.5; range, 2.2-18.3) in the control group. The mean time to late seizure recurrence was 56.6 months, and two-thirds of patients relapsed in the 5 years after surgery. Twenty of the relapse patients only experienced a single seizure, and 41% of the patients who reported more than one seizure had a frequency of less than one per month.
The type of resection had no discernible impact on outcomes, although anterior temporal lobe resection did trend toward being associated with recurrence (odds ratio, 2.7; 95% confidence interval, 0.93-8.89; P = .06). Incomplete resection was significantly associated with late relapse but did not seem to affect timing: the mean duration of seizure freedom was 56.5 months with complete resection and 58.5 months with incomplete resection (P = .62). Additional preoperative PET scans were performed on 45% of patients in the relapse group, compared with 29% in the control group.
After multivariate analysis, predictors for late relapse included incomplete resection (OR, 3.81; 95% CI, 1.79-8.53; P < .001); the existence of additional, potentially epileptogenic lesions in the contralateral hemisphere on presurgical MRI (OR, 3.36; 95% CI, 1.18-10.62; P = .03); epilepsy onset during the first year of life (OR, 4.24; 95% CI, 1.4-15.89; P = .02); and preoperative PET scans being performed (OR, 2.47; 95% CI, 1.25-4.97; P = .01). Though use of preoperative and postoperative antiepileptic drugs (AEDs) was higher in the relapse group, along with complete withdrawal being more common in the control group (68%, compared with 51%), neither was deemed significant in multivariate analysis.
What to do about seizure relapse risk factors
“This is one of the best analyses of the factors that contribute to late seizure relapse,” Gregory K. Bergey, MD, director of the Johns Hopkins Epilepsy Center in Baltimore, said in an interview. “Am I surprised by their results? Not necessarily.”
What did jump out, he said, was AED use not being a predictor of recurrence, as well as all the patients with late relapse having lesional epilepsy. “As they point out, you can have relapse with nonlesional epilepsy, but very often it happens in the first year or 2. If someone is 2 years out and doesn’t have a lesion, they’re probably more likely to remain seizure free.”
Despite the researchers’ comprehensive review of risk factors, the question remains: What to do with this information?
“They’ve done a very good job of identifying that 7.7% of 1,200 who are at risk of a late relapse,” he said. “Now, take those patients with high-risk factors and launch a trial where you keep medicines the same or do something that would alter that outcome.”
“The problem is,” he added, “that’s a 10-year study. It’s easy for me to sit here and call for one of those. But still, as valuable as this was, it’s a retrospective study. Now you have to say, what are the implications of this? What can we do in the prospective fashion?”
The authors acknowledged their study’s other limitations, including a lack of information on the reasons for an incomplete resection, a notable decrease in follow-up visits more than 5 years after surgery, and potential selection bias. They added, however, that “matching by age at surgery, gender, and time to relapse/last follow‐up” should have helped reduce any significant bias.
No potential conflicts of interest were disclosed.
according to a new study on the factors most associated with seizure recurrence in drug-resistant epilepsy.
“As our study analyzed late seizure relapse, our results are not applicable for short‐term seizure control. Vice versa, results for short‐term outcomes should not be transferred to long‐term outcomes,” Stephan Petrik of the Epilepsy Center at the University of Freiburg (Germany) and colleagues wrote. The study was published in the May 2021 issue of Epilepsia.
To assess the variables that increase risk of late seizure recurrence following surgery, the researchers retrospectively studied the medical records of patients who underwent resective epilepsy surgery at the University Hospital Freiburg (Germany) between 1999 and 2015. Of the 1,278 initial patients, a group of 99 participants (7.7%) with seizure relapses after at least 2 years of complete seizure freedom were matched with controls experiencing long-term seizure freedom. The two groups had similar mean durations of epilepsy from onset to surgery: 13.9 years in the relapse group and 13.0 years in the control group.
The mean follow-up was 9.7 years (standard deviation, 4.0; range, 2.9-18.5) in the relapse group and 8.2 years (SD, 3.5; range, 2.2-18.3) in the control group. The mean time to late seizure recurrence was 56.6 months, and two-thirds of patients relapsed in the 5 years after surgery. Twenty of the relapse patients only experienced a single seizure, and 41% of the patients who reported more than one seizure had a frequency of less than one per month.
The type of resection had no discernible impact on outcomes, although anterior temporal lobe resection did trend toward being associated with recurrence (odds ratio, 2.7; 95% confidence interval, 0.93-8.89; P = .06). Incomplete resection was significantly associated with late relapse but did not seem to affect timing: the mean duration of seizure freedom was 56.5 months with complete resection and 58.5 months with incomplete resection (P = .62). Additional preoperative PET scans were performed on 45% of patients in the relapse group, compared with 29% in the control group.
After multivariate analysis, predictors for late relapse included incomplete resection (OR, 3.81; 95% CI, 1.79-8.53; P < .001); the existence of additional, potentially epileptogenic lesions in the contralateral hemisphere on presurgical MRI (OR, 3.36; 95% CI, 1.18-10.62; P = .03); epilepsy onset during the first year of life (OR, 4.24; 95% CI, 1.4-15.89; P = .02); and preoperative PET scans being performed (OR, 2.47; 95% CI, 1.25-4.97; P = .01). Though use of preoperative and postoperative antiepileptic drugs (AEDs) was higher in the relapse group, along with complete withdrawal being more common in the control group (68%, compared with 51%), neither was deemed significant in multivariate analysis.
What to do about seizure relapse risk factors
“This is one of the best analyses of the factors that contribute to late seizure relapse,” Gregory K. Bergey, MD, director of the Johns Hopkins Epilepsy Center in Baltimore, said in an interview. “Am I surprised by their results? Not necessarily.”
What did jump out, he said, was AED use not being a predictor of recurrence, as well as all the patients with late relapse having lesional epilepsy. “As they point out, you can have relapse with nonlesional epilepsy, but very often it happens in the first year or 2. If someone is 2 years out and doesn’t have a lesion, they’re probably more likely to remain seizure free.”
Despite the researchers’ comprehensive review of risk factors, the question remains: What to do with this information?
“They’ve done a very good job of identifying that 7.7% of 1,200 who are at risk of a late relapse,” he said. “Now, take those patients with high-risk factors and launch a trial where you keep medicines the same or do something that would alter that outcome.”
“The problem is,” he added, “that’s a 10-year study. It’s easy for me to sit here and call for one of those. But still, as valuable as this was, it’s a retrospective study. Now you have to say, what are the implications of this? What can we do in the prospective fashion?”
The authors acknowledged their study’s other limitations, including a lack of information on the reasons for an incomplete resection, a notable decrease in follow-up visits more than 5 years after surgery, and potential selection bias. They added, however, that “matching by age at surgery, gender, and time to relapse/last follow‐up” should have helped reduce any significant bias.
No potential conflicts of interest were disclosed.
FROM EPILEPSIA
GELATO trial: Chemoimmunotherapy may help in metastatic invasive lobular breast cancer
The PD-L1 inhibitor atezolizumab (Tecentriq) combined with carboplatin has shown signs of clinical activity in women with metastatic invasive lobular breast cancer (ILC) according to the first results to come from the ongoing GELATO trial.
The 6-month objective response rate was 19%, based on 4 of 21 patients who could be evaluated exhibiting a partial response to the chemoimmunotherapy. A further two (10%) patients had stable disease, meaning that clinical benefit rate was 29%.
GELATO (AssessinG Efficacy of Carboplatin and ATezOlizumab in Metastatic Lobular Breast Cancer) is a phase 2 trial being conducted at four Dutch centers. The primary premise of the study is that “there’s an immune-related subtype of ILC,” researcher Leonie Voorwerk, BSc, reported at the European Society for Medical Oncology: Breast Cancer virtual meeting (Abstract LBA3).
This ILC subtype is “characterized by high expression of immune-related genes and high levels of TILs [tumor-infiltrating lymphocytes] and PDL-1,” said Ms. Voorwerk, a PhD student working with medical oncologist Marleen Kok, MD, PhD, at the Netherlands Cancer Institute in Amsterdam.
Furthermore, she added, in vitro data suggest sensitivity of immune-related-ILCs to platinum and there is preclinical work showing that there is synergy between platinum-based chemotherapy and checkpoint blockade.
First chemoimmunotherapy trial in lobular cancer setting
GELATO is a significant trial as it is “the first chemoimmunotherapy trial in metastatic lobular breast cancer,” said Sylvia Adams, MD, professor of medicine and director of the Breast Cancer Center at NYU Langone Health in New York City.
“Of note, the further research should include the immune-related genes and TMB [tumor mutational burden],” proposed Dr. Adams, who was not involved in the trial.
“We should look to tumor mutational burden because while it is not typically high in early disease, metastatic lesions can have higher TMB,” she explained. “Also, metastatic ILC is known to have higher tumor mutational burden compared to IDC [invasive ductal carcinoma], so this is an important thing along with the clinical factors as described in looking at outcomes.”
Trial design and patient characteristics
GELATO is a single-arm, nonrandomized trial in which 37 patients with metastatic ILC were screened for inclusion between November 2017 and January 2021. A total of 26 of these patients were registered for the trial, and 23 have so far received at least one cycle of atezolizumab.
Prerequisites for entry into the trial were that patients had to have negative or aberrant E-cadherin, a characteristic feature of ILC. Patients with estrogen receptor (ER)-positive (ER+) disease could be included, but they had to be proven to be resistant to endocrine therapies. No more than two prior lines of palliative chemotherapy were allowed, and all participants had to have lactose dehydrogenase levels of less than 2 times the upper limit of normal.
Patients were then treated with up to 12 cycles of weekly carboplatin (AUC = 1.5 mg/mL/min), with atezolizumab (1,200 mg) added in from cycle 3 onward. Treatment was continued until disease progression or unacceptable toxicity occurred.
“Baseline characteristics were mainly as expected for this patient population,” Ms. Voorwerk stated. Patients were aged 45-89 years, with a median of 60 years. Around half each had a WHO performance status of 0 or 1, and around half each had one to two or three or more metastatic sites; 78% had liver metastases.
“But I want to highlight that we included five patients with the triple-negative ILC,” said Ms. Voorwerk, also highlighting that approximately 50% of patients had received prior palliative chemotherapy. Later in her presentation she noted that four out of the six patients that showed any clinical benefit had triple negative disease.
Key findings and next steps
The primary endpoint was progression-free survival (PFS) at 6 months, with secondary endpoints of the best overall response rate, PFS at 1 year, overall survival, and safety.
While details of the latter three endpoints are yet to be reported, Ms. Voorwerk noted that there was a median duration of response of 12 weeks and the median PFS was 15 weeks. The primary endpoint of PFS was met as four patients were free of progression at 6 months and the statistical method used called for patients to be progression free at this time point.
“We observed that stromal TILs and CD8+ cells were not associated with clinical benefits,” said Ms. Voorwerk. There was, however, “a slight trend” toward higher PD-L1 expression in responding patients.
“Further translational research is needed to provide the rationale for new strategies to improve checkpoint blockade in patients with lobular breast cancer,” she concluded.
Dr. Adams concurred, adding that a future research question was whether either atezolizumab or carboplatin was contributing to the response. This is “difficult to tell as the study was a single arm trial.”
Another question, said Dr. Adams, is are “anti-CDK 4/6 inhibitors helpful in improving response rates and durability?” In the trial, 70% of patients had prior exposure to CDK 4/6 inhibitors.
The GELATO trial was sponsored by the Netherlands Cancer Institute with funding from Roche Pharma AG. Ms. Voorwerk had nothing to disclose. Dr. Adams disclosed uncompensated consulting or advisory roles with Bristol-Myers Squibb, Genentech, and Merck from whom she has received research funding. Dr. Adams also disclosed research funding from Amgen, Celgene, and Novartis.
The PD-L1 inhibitor atezolizumab (Tecentriq) combined with carboplatin has shown signs of clinical activity in women with metastatic invasive lobular breast cancer (ILC) according to the first results to come from the ongoing GELATO trial.
The 6-month objective response rate was 19%, based on 4 of 21 patients who could be evaluated exhibiting a partial response to the chemoimmunotherapy. A further two (10%) patients had stable disease, meaning that clinical benefit rate was 29%.
GELATO (AssessinG Efficacy of Carboplatin and ATezOlizumab in Metastatic Lobular Breast Cancer) is a phase 2 trial being conducted at four Dutch centers. The primary premise of the study is that “there’s an immune-related subtype of ILC,” researcher Leonie Voorwerk, BSc, reported at the European Society for Medical Oncology: Breast Cancer virtual meeting (Abstract LBA3).
This ILC subtype is “characterized by high expression of immune-related genes and high levels of TILs [tumor-infiltrating lymphocytes] and PDL-1,” said Ms. Voorwerk, a PhD student working with medical oncologist Marleen Kok, MD, PhD, at the Netherlands Cancer Institute in Amsterdam.
Furthermore, she added, in vitro data suggest sensitivity of immune-related-ILCs to platinum and there is preclinical work showing that there is synergy between platinum-based chemotherapy and checkpoint blockade.
First chemoimmunotherapy trial in lobular cancer setting
GELATO is a significant trial as it is “the first chemoimmunotherapy trial in metastatic lobular breast cancer,” said Sylvia Adams, MD, professor of medicine and director of the Breast Cancer Center at NYU Langone Health in New York City.
“Of note, the further research should include the immune-related genes and TMB [tumor mutational burden],” proposed Dr. Adams, who was not involved in the trial.
“We should look to tumor mutational burden because while it is not typically high in early disease, metastatic lesions can have higher TMB,” she explained. “Also, metastatic ILC is known to have higher tumor mutational burden compared to IDC [invasive ductal carcinoma], so this is an important thing along with the clinical factors as described in looking at outcomes.”
Trial design and patient characteristics
GELATO is a single-arm, nonrandomized trial in which 37 patients with metastatic ILC were screened for inclusion between November 2017 and January 2021. A total of 26 of these patients were registered for the trial, and 23 have so far received at least one cycle of atezolizumab.
Prerequisites for entry into the trial were that patients had to have negative or aberrant E-cadherin, a characteristic feature of ILC. Patients with estrogen receptor (ER)-positive (ER+) disease could be included, but they had to be proven to be resistant to endocrine therapies. No more than two prior lines of palliative chemotherapy were allowed, and all participants had to have lactose dehydrogenase levels of less than 2 times the upper limit of normal.
Patients were then treated with up to 12 cycles of weekly carboplatin (AUC = 1.5 mg/mL/min), with atezolizumab (1,200 mg) added in from cycle 3 onward. Treatment was continued until disease progression or unacceptable toxicity occurred.
“Baseline characteristics were mainly as expected for this patient population,” Ms. Voorwerk stated. Patients were aged 45-89 years, with a median of 60 years. Around half each had a WHO performance status of 0 or 1, and around half each had one to two or three or more metastatic sites; 78% had liver metastases.
“But I want to highlight that we included five patients with the triple-negative ILC,” said Ms. Voorwerk, also highlighting that approximately 50% of patients had received prior palliative chemotherapy. Later in her presentation she noted that four out of the six patients that showed any clinical benefit had triple negative disease.
Key findings and next steps
The primary endpoint was progression-free survival (PFS) at 6 months, with secondary endpoints of the best overall response rate, PFS at 1 year, overall survival, and safety.
While details of the latter three endpoints are yet to be reported, Ms. Voorwerk noted that there was a median duration of response of 12 weeks and the median PFS was 15 weeks. The primary endpoint of PFS was met as four patients were free of progression at 6 months and the statistical method used called for patients to be progression free at this time point.
“We observed that stromal TILs and CD8+ cells were not associated with clinical benefits,” said Ms. Voorwerk. There was, however, “a slight trend” toward higher PD-L1 expression in responding patients.
“Further translational research is needed to provide the rationale for new strategies to improve checkpoint blockade in patients with lobular breast cancer,” she concluded.
Dr. Adams concurred, adding that a future research question was whether either atezolizumab or carboplatin was contributing to the response. This is “difficult to tell as the study was a single arm trial.”
Another question, said Dr. Adams, is are “anti-CDK 4/6 inhibitors helpful in improving response rates and durability?” In the trial, 70% of patients had prior exposure to CDK 4/6 inhibitors.
The GELATO trial was sponsored by the Netherlands Cancer Institute with funding from Roche Pharma AG. Ms. Voorwerk had nothing to disclose. Dr. Adams disclosed uncompensated consulting or advisory roles with Bristol-Myers Squibb, Genentech, and Merck from whom she has received research funding. Dr. Adams also disclosed research funding from Amgen, Celgene, and Novartis.
The PD-L1 inhibitor atezolizumab (Tecentriq) combined with carboplatin has shown signs of clinical activity in women with metastatic invasive lobular breast cancer (ILC) according to the first results to come from the ongoing GELATO trial.
The 6-month objective response rate was 19%, based on 4 of 21 patients who could be evaluated exhibiting a partial response to the chemoimmunotherapy. A further two (10%) patients had stable disease, meaning that clinical benefit rate was 29%.
GELATO (AssessinG Efficacy of Carboplatin and ATezOlizumab in Metastatic Lobular Breast Cancer) is a phase 2 trial being conducted at four Dutch centers. The primary premise of the study is that “there’s an immune-related subtype of ILC,” researcher Leonie Voorwerk, BSc, reported at the European Society for Medical Oncology: Breast Cancer virtual meeting (Abstract LBA3).
This ILC subtype is “characterized by high expression of immune-related genes and high levels of TILs [tumor-infiltrating lymphocytes] and PDL-1,” said Ms. Voorwerk, a PhD student working with medical oncologist Marleen Kok, MD, PhD, at the Netherlands Cancer Institute in Amsterdam.
Furthermore, she added, in vitro data suggest sensitivity of immune-related-ILCs to platinum and there is preclinical work showing that there is synergy between platinum-based chemotherapy and checkpoint blockade.
First chemoimmunotherapy trial in lobular cancer setting
GELATO is a significant trial as it is “the first chemoimmunotherapy trial in metastatic lobular breast cancer,” said Sylvia Adams, MD, professor of medicine and director of the Breast Cancer Center at NYU Langone Health in New York City.
“Of note, the further research should include the immune-related genes and TMB [tumor mutational burden],” proposed Dr. Adams, who was not involved in the trial.
“We should look to tumor mutational burden because while it is not typically high in early disease, metastatic lesions can have higher TMB,” she explained. “Also, metastatic ILC is known to have higher tumor mutational burden compared to IDC [invasive ductal carcinoma], so this is an important thing along with the clinical factors as described in looking at outcomes.”
Trial design and patient characteristics
GELATO is a single-arm, nonrandomized trial in which 37 patients with metastatic ILC were screened for inclusion between November 2017 and January 2021. A total of 26 of these patients were registered for the trial, and 23 have so far received at least one cycle of atezolizumab.
Prerequisites for entry into the trial were that patients had to have negative or aberrant E-cadherin, a characteristic feature of ILC. Patients with estrogen receptor (ER)-positive (ER+) disease could be included, but they had to be proven to be resistant to endocrine therapies. No more than two prior lines of palliative chemotherapy were allowed, and all participants had to have lactose dehydrogenase levels of less than 2 times the upper limit of normal.
Patients were then treated with up to 12 cycles of weekly carboplatin (AUC = 1.5 mg/mL/min), with atezolizumab (1,200 mg) added in from cycle 3 onward. Treatment was continued until disease progression or unacceptable toxicity occurred.
“Baseline characteristics were mainly as expected for this patient population,” Ms. Voorwerk stated. Patients were aged 45-89 years, with a median of 60 years. Around half each had a WHO performance status of 0 or 1, and around half each had one to two or three or more metastatic sites; 78% had liver metastases.
“But I want to highlight that we included five patients with the triple-negative ILC,” said Ms. Voorwerk, also highlighting that approximately 50% of patients had received prior palliative chemotherapy. Later in her presentation she noted that four out of the six patients that showed any clinical benefit had triple negative disease.
Key findings and next steps
The primary endpoint was progression-free survival (PFS) at 6 months, with secondary endpoints of the best overall response rate, PFS at 1 year, overall survival, and safety.
While details of the latter three endpoints are yet to be reported, Ms. Voorwerk noted that there was a median duration of response of 12 weeks and the median PFS was 15 weeks. The primary endpoint of PFS was met as four patients were free of progression at 6 months and the statistical method used called for patients to be progression free at this time point.
“We observed that stromal TILs and CD8+ cells were not associated with clinical benefits,” said Ms. Voorwerk. There was, however, “a slight trend” toward higher PD-L1 expression in responding patients.
“Further translational research is needed to provide the rationale for new strategies to improve checkpoint blockade in patients with lobular breast cancer,” she concluded.
Dr. Adams concurred, adding that a future research question was whether either atezolizumab or carboplatin was contributing to the response. This is “difficult to tell as the study was a single arm trial.”
Another question, said Dr. Adams, is are “anti-CDK 4/6 inhibitors helpful in improving response rates and durability?” In the trial, 70% of patients had prior exposure to CDK 4/6 inhibitors.
The GELATO trial was sponsored by the Netherlands Cancer Institute with funding from Roche Pharma AG. Ms. Voorwerk had nothing to disclose. Dr. Adams disclosed uncompensated consulting or advisory roles with Bristol-Myers Squibb, Genentech, and Merck from whom she has received research funding. Dr. Adams also disclosed research funding from Amgen, Celgene, and Novartis.
FROM ESMO BREAST CANCER 2021
No survival dip with neoadjuvant letrozole-palbociclib in NeoPAL study
Three-year survival rates were similarly high among postmenopausal women with high-risk early luminal breast cancer who were treated with either the neoadjuvant combination of letrozole and palbociclib (Ibrance) or standard neoadjuvant chemotherapy in the phase 2 NeoPAL study.
Progression-free survival (PFS) was a respective 86.7% and 87.2%, with a hazard ratio (HR) of 1.01 (P = .98) comparing the endocrine therapy and cyclin-dependent kinase (CDK) 4/6 inhibitor combination versus FEC/taxane chemotherapy.
There were also no differences between the two treatment arms in terms of invasive disease-free survival (iDFS, HR = 0.83, P = .71) or breast cancer–specific survival (BCSS), although the latter was an exploratory endpoint alongside overall survival (OS).
“The lack of difference is impressive,” said Hope S. Rugo, MD, FASCO, who commented independently on the study’s findings after their presentation at the European Society for Medical Oncology: Breast Cancer virtual meeting.
“Overall survival in patients who received chemotherapy appears to be better, but the very small numbers here make interpretation of this difference impossible,” observed Dr. Rugo, professor of medicine at the University of California San Francisco’s Helen Diller Family Comprehensive Cancer Center.
“Unfortunately, this study is underpowered for definitive conclusions,” acknowledged study investigator Suzette Delaloge, MD, associate professor of medical oncology at Institut Gustave Roussy in Villejuif, France.
However, “it shows that the nonchemotherapy, preoperative letrozole/palbociclib approach deserves further exploration and could be an option for a chemotherapy-free regimen in some specific cases.”
Primary data already reported
The NeoPAL study was an open-label, randomized study conducted in 27 centers throughout France that compared the preoperative use of letrozole plus palbociclib to neoadjuvant chemotherapy in 106 postmenopausal patients with either luminal A or B node-positive disease.
Patients were considered for inclusion in the trial if they had been newly diagnosed with estrogen receptor (ER)-positive, HER2-negative stage I-III breast cancer and were not candidates for breast conservation. Genetic testing was used to confirm that only those with luminal B, or luminal A and who were node positive were recruited.
Neoadjuvant treatment consisted of either letrozole (2.5 mg/day) and palbociclib (125 mg daily for 3 weeks out of 4 weeks) for 19 weeks or three 21-day cycles of 5-fluorouracil (500 mg/m2), epirubicin (100 mg/m2), and cyclophosphamide (500 mg/m2), followed by three 21-day cycles of docetaxel (100 mg/m2).
The primary endpoint was the pathological complete response (pCR), defined as a residual cancer burden (RCB) of 0 to 1. Results, which have already been reported, showed equivalent, but perhaps disappointingly low, pathological responses in both the letrozole/palbociclib and chemotherapy arms (3.8% and 5.9%, respectively).
There were, however, identical clinical responses (at around 75%) and “encouraging biomarker responses in the Prosigna-defined high risk luminal breast cancer population,” Dr. Delaloge said.
The NeoPAL findings were on par with those of the CORALLEEN study, Dr. Delaloge suggested. That trial, as Dr. Rugo has also pointed out, was conducted in 106 patients with luminal B early breast cancer and used a combination of letrozole and the CDK 4/6 inhibitor ribociclib (Kisquali).
Future studies needed
NeoPAL “is a small study with relatively short follow-up even for hormone receptor-positive, high-risk disease,” Dr. Rugo observed. However, she qualified “this short follow-up can be very meaningful in high-risk disease.” as shown by other CDK 4/6 inhibitor trials.
Dr. Rugo also noted: “Short-term biologic endpoints are clearly more informative following and during neoadjuvant endocrine therapy than pCR and this trial, as well as the data from previous studies, indicates that this is the case.”
Further, Dr. Rugo said: “Antiproliferative response is enhanced with CDK 4/6 inhibitors, but this doesn’t seem to translate into a difference in pCR. The lack of impact on longer term, outcome to date, provides support for ongoing trials.”
Two such trials are already underway. The 200-patient CARABELA trial started recruitment in March last year and is comparing endocrine therapy with letrozole plus the CDK 4/6 inhibitor abemaciclib (Verzenio) to standard chemotherapy in patients with hormone receptor–positive, high-risk Ki67 disease.
Then there is the ADAPTcycle trial, a large open-label, phase 3 trial that is randomizing patients based on Ki67 and recurrence score after a short preoperative induction with endocrine therapy to postoperative chemotherapy or to 2 years of endocrine therapy plus ribociclib, with both arms receiving a standard course of 5 years of endocrine therapy.
“These two studies have provided interesting information that will help us design studies in the future,” said Dr. Rugo.
Not only that, but they will also help “investigate the subgroups of patients that benefit the most from CDK 4/6 inhibitors and better study neoadjuvant endocrine therapy which is an important option for patients that can be evaluated in terms of its efficacy by short term measures of antiproliferative response.”
NeoPAL was sponsored by UNICANCER with funding from Pfizer and NanoString Technologies. Dr. Delaloge disclosed receiving research grants or funding via her institution from Pfizer, AstraZeneca, Roche, Merck, Sanofi, Lilly, Novartis, BMS, Orion, Daiichi, Puma, and Pierre Fabre. Dr. Rugo reported receipt of grants via her institution to perform clinical trials from Pfizer and multiple other companies. She disclosed receiving honoraria from PUMA, Samsung, and Mylan.
Three-year survival rates were similarly high among postmenopausal women with high-risk early luminal breast cancer who were treated with either the neoadjuvant combination of letrozole and palbociclib (Ibrance) or standard neoadjuvant chemotherapy in the phase 2 NeoPAL study.
Progression-free survival (PFS) was a respective 86.7% and 87.2%, with a hazard ratio (HR) of 1.01 (P = .98) comparing the endocrine therapy and cyclin-dependent kinase (CDK) 4/6 inhibitor combination versus FEC/taxane chemotherapy.
There were also no differences between the two treatment arms in terms of invasive disease-free survival (iDFS, HR = 0.83, P = .71) or breast cancer–specific survival (BCSS), although the latter was an exploratory endpoint alongside overall survival (OS).
“The lack of difference is impressive,” said Hope S. Rugo, MD, FASCO, who commented independently on the study’s findings after their presentation at the European Society for Medical Oncology: Breast Cancer virtual meeting.
“Overall survival in patients who received chemotherapy appears to be better, but the very small numbers here make interpretation of this difference impossible,” observed Dr. Rugo, professor of medicine at the University of California San Francisco’s Helen Diller Family Comprehensive Cancer Center.
“Unfortunately, this study is underpowered for definitive conclusions,” acknowledged study investigator Suzette Delaloge, MD, associate professor of medical oncology at Institut Gustave Roussy in Villejuif, France.
However, “it shows that the nonchemotherapy, preoperative letrozole/palbociclib approach deserves further exploration and could be an option for a chemotherapy-free regimen in some specific cases.”
Primary data already reported
The NeoPAL study was an open-label, randomized study conducted in 27 centers throughout France that compared the preoperative use of letrozole plus palbociclib to neoadjuvant chemotherapy in 106 postmenopausal patients with either luminal A or B node-positive disease.
Patients were considered for inclusion in the trial if they had been newly diagnosed with estrogen receptor (ER)-positive, HER2-negative stage I-III breast cancer and were not candidates for breast conservation. Genetic testing was used to confirm that only those with luminal B, or luminal A and who were node positive were recruited.
Neoadjuvant treatment consisted of either letrozole (2.5 mg/day) and palbociclib (125 mg daily for 3 weeks out of 4 weeks) for 19 weeks or three 21-day cycles of 5-fluorouracil (500 mg/m2), epirubicin (100 mg/m2), and cyclophosphamide (500 mg/m2), followed by three 21-day cycles of docetaxel (100 mg/m2).
The primary endpoint was the pathological complete response (pCR), defined as a residual cancer burden (RCB) of 0 to 1. Results, which have already been reported, showed equivalent, but perhaps disappointingly low, pathological responses in both the letrozole/palbociclib and chemotherapy arms (3.8% and 5.9%, respectively).
There were, however, identical clinical responses (at around 75%) and “encouraging biomarker responses in the Prosigna-defined high risk luminal breast cancer population,” Dr. Delaloge said.
The NeoPAL findings were on par with those of the CORALLEEN study, Dr. Delaloge suggested. That trial, as Dr. Rugo has also pointed out, was conducted in 106 patients with luminal B early breast cancer and used a combination of letrozole and the CDK 4/6 inhibitor ribociclib (Kisquali).
Future studies needed
NeoPAL “is a small study with relatively short follow-up even for hormone receptor-positive, high-risk disease,” Dr. Rugo observed. However, she qualified “this short follow-up can be very meaningful in high-risk disease.” as shown by other CDK 4/6 inhibitor trials.
Dr. Rugo also noted: “Short-term biologic endpoints are clearly more informative following and during neoadjuvant endocrine therapy than pCR and this trial, as well as the data from previous studies, indicates that this is the case.”
Further, Dr. Rugo said: “Antiproliferative response is enhanced with CDK 4/6 inhibitors, but this doesn’t seem to translate into a difference in pCR. The lack of impact on longer term, outcome to date, provides support for ongoing trials.”
Two such trials are already underway. The 200-patient CARABELA trial started recruitment in March last year and is comparing endocrine therapy with letrozole plus the CDK 4/6 inhibitor abemaciclib (Verzenio) to standard chemotherapy in patients with hormone receptor–positive, high-risk Ki67 disease.
Then there is the ADAPTcycle trial, a large open-label, phase 3 trial that is randomizing patients based on Ki67 and recurrence score after a short preoperative induction with endocrine therapy to postoperative chemotherapy or to 2 years of endocrine therapy plus ribociclib, with both arms receiving a standard course of 5 years of endocrine therapy.
“These two studies have provided interesting information that will help us design studies in the future,” said Dr. Rugo.
Not only that, but they will also help “investigate the subgroups of patients that benefit the most from CDK 4/6 inhibitors and better study neoadjuvant endocrine therapy which is an important option for patients that can be evaluated in terms of its efficacy by short term measures of antiproliferative response.”
NeoPAL was sponsored by UNICANCER with funding from Pfizer and NanoString Technologies. Dr. Delaloge disclosed receiving research grants or funding via her institution from Pfizer, AstraZeneca, Roche, Merck, Sanofi, Lilly, Novartis, BMS, Orion, Daiichi, Puma, and Pierre Fabre. Dr. Rugo reported receipt of grants via her institution to perform clinical trials from Pfizer and multiple other companies. She disclosed receiving honoraria from PUMA, Samsung, and Mylan.
Three-year survival rates were similarly high among postmenopausal women with high-risk early luminal breast cancer who were treated with either the neoadjuvant combination of letrozole and palbociclib (Ibrance) or standard neoadjuvant chemotherapy in the phase 2 NeoPAL study.
Progression-free survival (PFS) was a respective 86.7% and 87.2%, with a hazard ratio (HR) of 1.01 (P = .98) comparing the endocrine therapy and cyclin-dependent kinase (CDK) 4/6 inhibitor combination versus FEC/taxane chemotherapy.
There were also no differences between the two treatment arms in terms of invasive disease-free survival (iDFS, HR = 0.83, P = .71) or breast cancer–specific survival (BCSS), although the latter was an exploratory endpoint alongside overall survival (OS).
“The lack of difference is impressive,” said Hope S. Rugo, MD, FASCO, who commented independently on the study’s findings after their presentation at the European Society for Medical Oncology: Breast Cancer virtual meeting.
“Overall survival in patients who received chemotherapy appears to be better, but the very small numbers here make interpretation of this difference impossible,” observed Dr. Rugo, professor of medicine at the University of California San Francisco’s Helen Diller Family Comprehensive Cancer Center.
“Unfortunately, this study is underpowered for definitive conclusions,” acknowledged study investigator Suzette Delaloge, MD, associate professor of medical oncology at Institut Gustave Roussy in Villejuif, France.
However, “it shows that the nonchemotherapy, preoperative letrozole/palbociclib approach deserves further exploration and could be an option for a chemotherapy-free regimen in some specific cases.”
Primary data already reported
The NeoPAL study was an open-label, randomized study conducted in 27 centers throughout France that compared the preoperative use of letrozole plus palbociclib to neoadjuvant chemotherapy in 106 postmenopausal patients with either luminal A or B node-positive disease.
Patients were considered for inclusion in the trial if they had been newly diagnosed with estrogen receptor (ER)-positive, HER2-negative stage I-III breast cancer and were not candidates for breast conservation. Genetic testing was used to confirm that only those with luminal B, or luminal A and who were node positive were recruited.
Neoadjuvant treatment consisted of either letrozole (2.5 mg/day) and palbociclib (125 mg daily for 3 weeks out of 4 weeks) for 19 weeks or three 21-day cycles of 5-fluorouracil (500 mg/m2), epirubicin (100 mg/m2), and cyclophosphamide (500 mg/m2), followed by three 21-day cycles of docetaxel (100 mg/m2).
The primary endpoint was the pathological complete response (pCR), defined as a residual cancer burden (RCB) of 0 to 1. Results, which have already been reported, showed equivalent, but perhaps disappointingly low, pathological responses in both the letrozole/palbociclib and chemotherapy arms (3.8% and 5.9%, respectively).
There were, however, identical clinical responses (at around 75%) and “encouraging biomarker responses in the Prosigna-defined high risk luminal breast cancer population,” Dr. Delaloge said.
The NeoPAL findings were on par with those of the CORALLEEN study, Dr. Delaloge suggested. That trial, as Dr. Rugo has also pointed out, was conducted in 106 patients with luminal B early breast cancer and used a combination of letrozole and the CDK 4/6 inhibitor ribociclib (Kisquali).
Future studies needed
NeoPAL “is a small study with relatively short follow-up even for hormone receptor-positive, high-risk disease,” Dr. Rugo observed. However, she qualified “this short follow-up can be very meaningful in high-risk disease.” as shown by other CDK 4/6 inhibitor trials.
Dr. Rugo also noted: “Short-term biologic endpoints are clearly more informative following and during neoadjuvant endocrine therapy than pCR and this trial, as well as the data from previous studies, indicates that this is the case.”
Further, Dr. Rugo said: “Antiproliferative response is enhanced with CDK 4/6 inhibitors, but this doesn’t seem to translate into a difference in pCR. The lack of impact on longer term, outcome to date, provides support for ongoing trials.”
Two such trials are already underway. The 200-patient CARABELA trial started recruitment in March last year and is comparing endocrine therapy with letrozole plus the CDK 4/6 inhibitor abemaciclib (Verzenio) to standard chemotherapy in patients with hormone receptor–positive, high-risk Ki67 disease.
Then there is the ADAPTcycle trial, a large open-label, phase 3 trial that is randomizing patients based on Ki67 and recurrence score after a short preoperative induction with endocrine therapy to postoperative chemotherapy or to 2 years of endocrine therapy plus ribociclib, with both arms receiving a standard course of 5 years of endocrine therapy.
“These two studies have provided interesting information that will help us design studies in the future,” said Dr. Rugo.
Not only that, but they will also help “investigate the subgroups of patients that benefit the most from CDK 4/6 inhibitors and better study neoadjuvant endocrine therapy which is an important option for patients that can be evaluated in terms of its efficacy by short term measures of antiproliferative response.”
NeoPAL was sponsored by UNICANCER with funding from Pfizer and NanoString Technologies. Dr. Delaloge disclosed receiving research grants or funding via her institution from Pfizer, AstraZeneca, Roche, Merck, Sanofi, Lilly, Novartis, BMS, Orion, Daiichi, Puma, and Pierre Fabre. Dr. Rugo reported receipt of grants via her institution to perform clinical trials from Pfizer and multiple other companies. She disclosed receiving honoraria from PUMA, Samsung, and Mylan.
FROM ESMO BREAST CANCER 2021
Race, ethnicity, and socioeconomics are often barriers to migraine care
, according to a study published in the April issue of Headache. People of African descent and Latinx ethnicity tend to fare worse than other people of color and their White counterparts.
“It should be shocking to neurologists and other clinicians who care for migraine patients how few are able to successfully traverse the barriers to achieve an accurate diagnosis and proper, evidence-based, acute and preventative treatment,” commented Peter McAllister, MD, medical director at the New England Institute for Neurology and Headache and chief medical officer for clinical research at Ki Clinical Research in Stamford, Conn. Dr. McAllister was not involved in this study.
Assessing barriers to care
Researchers designed the study with the primary objective of estimating the number of patients with migraines with unmet clinical needs and who were impacted by four preidentified barriers to care. To evaluate their objective, researchers conducted a longitudinal, Internet-based survey known as the Chronic Migraine Epidemiology and Outcomes (CaMEO) study. They collected data over 1 year examining a cohort of patients that mimicked the diverse demographics of the U.S. population. Researchers conducted longitudinal assessments every 3 months for 15 months, incorporating cross-sectional analyses that surveyed health care use, family burden, and comorbidities or endophenotypes.
Eligible enrollees were 18 years of age or older.
Researchers identified four barriers that hindered patient outcomes, and they served as the primary outcomes of the studies. They were:
- Health care provider consultations. Investigators used study participants’ responses to the following question during their interactions with their health care providers to help evaluate the quality of their consultation experience: “What type of doctor is currently managing your headaches?” Researchers included data from patients whose practitioners fit the description of those they deemed best suited to address ongoing headache challenges. These medical professionals included general practitioners, family physicians, internal medicine doctors, nurse practitioners, physician assistants, neurologists, pain specialists, headache specialists, and obstetrician-gynecologists.
- Diagnosis. Carefully evaluating patients’ responses to a series of questions helped researchers gauge the accuracy of diagnosis. Questions included: “Have you ever been diagnosed by a doctor or other health professional with any of the following types of headaches?” Respondents were also given a list of options that provided additional context around their headaches and were encouraged to select all appropriate responses. The list included a fictional response option of “citrene headache” to determine incorrect responses. For this study, researchers deemed it necessary to recognize a chronic migraine diagnosis to ensure that patients received appropriate treatment.
- Minimally appropriate pharmacologic treatment. Researchers used the following question to determine whether patients’ chronic migraine and episodic migraine were being managed with the least amount of pharmacological treatment necessary. “Which of these medications (if any) are you currently using (or typically keep on hand) to treat your headaches when you have them?” Researchers defined “minimally appropriate acute pharmacologic treatment” as the use of any prescription nonsteroidal anti-inflammatory drug (NSAID), triptan, ergotamine derivative, or isometheptene.
- Avoidance of medication overuse. The study authors pointed out the sometimes nebulous process of characterizing the appropriate use of preventative medication in patients with episodic migraines as “not straightforward” for some patients because not all patients require preventive treatment. Study participants were required to report having received any form of preventative therapy, defined as pharmacological therapies approved by guidelines and supported by data. Such therapies included various antiseizure medication, antidepressants (for example, doxepin, venlafaxine, duloxetine, amitriptyline, imipramine, nortriptyline, and desvenlafaxine), antihypertensives, and toxin injections. Treatments such as behavioral and neuromodulatory therapies were excluded from the list.
According to lead author Dawn C. Buse, PhD, of the department of neurology at Albert Einstein College of Medicine, New York, acute medication overuse provides an important modifiable target for intervention and recommends that clinicians use the opportunity to optimize migraine care by reducing the patients’ reliance on acute therapies. Taking such initiatives to decrease medication overuse is especially important in communities of color, who are more likely to overuse medications for migraines.
Patients with higher income levels were more likely to overcome each barrier. People of African, African American, or multiracial descent were more prone to overuse of medications to manage their migraines.
Of the 489,537 respondents invited to participate in the CaMEO study, 16,879 qualified for inclusion. Slightly more than half of the respondents (n = 9,184 [54.7%]) had a migraine-related disability (MIDAS) score of 6 or greater – an indicator of disability that is least mild in nature. Most patients who had episodic migraines or chronic migraines (86.2%) had some form of health insurance coverage (n = 9.184; 84.1%; P = .048). Of those patients who were insured, 7,930 patients experienced episodic migraine (86.3%) and the remainder had chronic migraine (n = 1,254; 13.7%). Higher-income patients were more likely to traverse barriers to care. While patients of African descent had higher consultation rates, they also had higher rates of acute medication overuse.
Patients with chronic migraine were more likely to be older than patients with episodic migraine (41.0 vs. 39.6 years; P = .0001) and female (83.0% vs. 79.0%; P = .001), and White (84.5% vs. 79.1%; P < .001). Similarly, patients with chronic migraine were more likely to have a higher mean body mass index (29.8 kg/m2 vs. 28.9 kg/m2; P < .001) and lower rates of full- or part-time employment (56.8% vs. 67.1%; P < .001), and were less likely to have a 4-year degree (64.8 vs. 55.6; P < .001) and annual household incomes below $75,000 (72.6% vs. 64.6%; P < .001). Approximately three-quarters of the patients with episodic migraine (75.7%; 1655/2187) and one-third of patients with chronic migraine (32.8%; 168/512) received accurate diagnoses.
The data uncovered an association with acute medication overuse. Among current consulters who had received an accurate diagnosis and minimally adequate treatment, medication overuse rates were highest among those reporting two or more races (53%) and Blacks and African Americans (45%) and lowest among Whites (33%) and those categorized as “other” race (32%). Ethnic and cultural differences in headache literacy may contribute to differences in medication overuse.
Strategies to improve outcomes
Both Dr. Buse and Dr. McAllister see the value advocacy and education offer in helping to improve outcomes in marginalized communities and other groups negatively impacted by various barriers.
“Patient advocacy and outreach are key here, especially in those traditionally underrepresented in the migraine space, such as men, people of color, blue-collar workers, etc.,” Dr. McAllister noted.
Dr. Buse emphasized the importance of education for patients and health care professionals alike. “A large percentage of people who meet criteria for migraine in the U.S. do not seek care or possibly even know that they have migraines,” Dr. Buse said. “This finding underscores the importance of public health education about migraine as well as well as providing migraine support, education, and resources to health care professionals on the front lines.”
Other strategies recommended by Dr, Buse to ease the impact of barriers include encouraging patient discussion, setting up time for follow-up appointments and education, referring patients for neurological and other specialty consults when warranted, reviewing essential lifestyle habits for migraine management, and creating personalized, mutually agreed-upon treatment plans.
Dr. Buse has received support and honoraria from AbbVie, Amgen, Avanir, Biohaven, Eli Lilly, and Promius.
, according to a study published in the April issue of Headache. People of African descent and Latinx ethnicity tend to fare worse than other people of color and their White counterparts.
“It should be shocking to neurologists and other clinicians who care for migraine patients how few are able to successfully traverse the barriers to achieve an accurate diagnosis and proper, evidence-based, acute and preventative treatment,” commented Peter McAllister, MD, medical director at the New England Institute for Neurology and Headache and chief medical officer for clinical research at Ki Clinical Research in Stamford, Conn. Dr. McAllister was not involved in this study.
Assessing barriers to care
Researchers designed the study with the primary objective of estimating the number of patients with migraines with unmet clinical needs and who were impacted by four preidentified barriers to care. To evaluate their objective, researchers conducted a longitudinal, Internet-based survey known as the Chronic Migraine Epidemiology and Outcomes (CaMEO) study. They collected data over 1 year examining a cohort of patients that mimicked the diverse demographics of the U.S. population. Researchers conducted longitudinal assessments every 3 months for 15 months, incorporating cross-sectional analyses that surveyed health care use, family burden, and comorbidities or endophenotypes.
Eligible enrollees were 18 years of age or older.
Researchers identified four barriers that hindered patient outcomes, and they served as the primary outcomes of the studies. They were:
- Health care provider consultations. Investigators used study participants’ responses to the following question during their interactions with their health care providers to help evaluate the quality of their consultation experience: “What type of doctor is currently managing your headaches?” Researchers included data from patients whose practitioners fit the description of those they deemed best suited to address ongoing headache challenges. These medical professionals included general practitioners, family physicians, internal medicine doctors, nurse practitioners, physician assistants, neurologists, pain specialists, headache specialists, and obstetrician-gynecologists.
- Diagnosis. Carefully evaluating patients’ responses to a series of questions helped researchers gauge the accuracy of diagnosis. Questions included: “Have you ever been diagnosed by a doctor or other health professional with any of the following types of headaches?” Respondents were also given a list of options that provided additional context around their headaches and were encouraged to select all appropriate responses. The list included a fictional response option of “citrene headache” to determine incorrect responses. For this study, researchers deemed it necessary to recognize a chronic migraine diagnosis to ensure that patients received appropriate treatment.
- Minimally appropriate pharmacologic treatment. Researchers used the following question to determine whether patients’ chronic migraine and episodic migraine were being managed with the least amount of pharmacological treatment necessary. “Which of these medications (if any) are you currently using (or typically keep on hand) to treat your headaches when you have them?” Researchers defined “minimally appropriate acute pharmacologic treatment” as the use of any prescription nonsteroidal anti-inflammatory drug (NSAID), triptan, ergotamine derivative, or isometheptene.
- Avoidance of medication overuse. The study authors pointed out the sometimes nebulous process of characterizing the appropriate use of preventative medication in patients with episodic migraines as “not straightforward” for some patients because not all patients require preventive treatment. Study participants were required to report having received any form of preventative therapy, defined as pharmacological therapies approved by guidelines and supported by data. Such therapies included various antiseizure medication, antidepressants (for example, doxepin, venlafaxine, duloxetine, amitriptyline, imipramine, nortriptyline, and desvenlafaxine), antihypertensives, and toxin injections. Treatments such as behavioral and neuromodulatory therapies were excluded from the list.
According to lead author Dawn C. Buse, PhD, of the department of neurology at Albert Einstein College of Medicine, New York, acute medication overuse provides an important modifiable target for intervention and recommends that clinicians use the opportunity to optimize migraine care by reducing the patients’ reliance on acute therapies. Taking such initiatives to decrease medication overuse is especially important in communities of color, who are more likely to overuse medications for migraines.
Patients with higher income levels were more likely to overcome each barrier. People of African, African American, or multiracial descent were more prone to overuse of medications to manage their migraines.
Of the 489,537 respondents invited to participate in the CaMEO study, 16,879 qualified for inclusion. Slightly more than half of the respondents (n = 9,184 [54.7%]) had a migraine-related disability (MIDAS) score of 6 or greater – an indicator of disability that is least mild in nature. Most patients who had episodic migraines or chronic migraines (86.2%) had some form of health insurance coverage (n = 9.184; 84.1%; P = .048). Of those patients who were insured, 7,930 patients experienced episodic migraine (86.3%) and the remainder had chronic migraine (n = 1,254; 13.7%). Higher-income patients were more likely to traverse barriers to care. While patients of African descent had higher consultation rates, they also had higher rates of acute medication overuse.
Patients with chronic migraine were more likely to be older than patients with episodic migraine (41.0 vs. 39.6 years; P = .0001) and female (83.0% vs. 79.0%; P = .001), and White (84.5% vs. 79.1%; P < .001). Similarly, patients with chronic migraine were more likely to have a higher mean body mass index (29.8 kg/m2 vs. 28.9 kg/m2; P < .001) and lower rates of full- or part-time employment (56.8% vs. 67.1%; P < .001), and were less likely to have a 4-year degree (64.8 vs. 55.6; P < .001) and annual household incomes below $75,000 (72.6% vs. 64.6%; P < .001). Approximately three-quarters of the patients with episodic migraine (75.7%; 1655/2187) and one-third of patients with chronic migraine (32.8%; 168/512) received accurate diagnoses.
The data uncovered an association with acute medication overuse. Among current consulters who had received an accurate diagnosis and minimally adequate treatment, medication overuse rates were highest among those reporting two or more races (53%) and Blacks and African Americans (45%) and lowest among Whites (33%) and those categorized as “other” race (32%). Ethnic and cultural differences in headache literacy may contribute to differences in medication overuse.
Strategies to improve outcomes
Both Dr. Buse and Dr. McAllister see the value advocacy and education offer in helping to improve outcomes in marginalized communities and other groups negatively impacted by various barriers.
“Patient advocacy and outreach are key here, especially in those traditionally underrepresented in the migraine space, such as men, people of color, blue-collar workers, etc.,” Dr. McAllister noted.
Dr. Buse emphasized the importance of education for patients and health care professionals alike. “A large percentage of people who meet criteria for migraine in the U.S. do not seek care or possibly even know that they have migraines,” Dr. Buse said. “This finding underscores the importance of public health education about migraine as well as well as providing migraine support, education, and resources to health care professionals on the front lines.”
Other strategies recommended by Dr, Buse to ease the impact of barriers include encouraging patient discussion, setting up time for follow-up appointments and education, referring patients for neurological and other specialty consults when warranted, reviewing essential lifestyle habits for migraine management, and creating personalized, mutually agreed-upon treatment plans.
Dr. Buse has received support and honoraria from AbbVie, Amgen, Avanir, Biohaven, Eli Lilly, and Promius.
, according to a study published in the April issue of Headache. People of African descent and Latinx ethnicity tend to fare worse than other people of color and their White counterparts.
“It should be shocking to neurologists and other clinicians who care for migraine patients how few are able to successfully traverse the barriers to achieve an accurate diagnosis and proper, evidence-based, acute and preventative treatment,” commented Peter McAllister, MD, medical director at the New England Institute for Neurology and Headache and chief medical officer for clinical research at Ki Clinical Research in Stamford, Conn. Dr. McAllister was not involved in this study.
Assessing barriers to care
Researchers designed the study with the primary objective of estimating the number of patients with migraines with unmet clinical needs and who were impacted by four preidentified barriers to care. To evaluate their objective, researchers conducted a longitudinal, Internet-based survey known as the Chronic Migraine Epidemiology and Outcomes (CaMEO) study. They collected data over 1 year examining a cohort of patients that mimicked the diverse demographics of the U.S. population. Researchers conducted longitudinal assessments every 3 months for 15 months, incorporating cross-sectional analyses that surveyed health care use, family burden, and comorbidities or endophenotypes.
Eligible enrollees were 18 years of age or older.
Researchers identified four barriers that hindered patient outcomes, and they served as the primary outcomes of the studies. They were:
- Health care provider consultations. Investigators used study participants’ responses to the following question during their interactions with their health care providers to help evaluate the quality of their consultation experience: “What type of doctor is currently managing your headaches?” Researchers included data from patients whose practitioners fit the description of those they deemed best suited to address ongoing headache challenges. These medical professionals included general practitioners, family physicians, internal medicine doctors, nurse practitioners, physician assistants, neurologists, pain specialists, headache specialists, and obstetrician-gynecologists.
- Diagnosis. Carefully evaluating patients’ responses to a series of questions helped researchers gauge the accuracy of diagnosis. Questions included: “Have you ever been diagnosed by a doctor or other health professional with any of the following types of headaches?” Respondents were also given a list of options that provided additional context around their headaches and were encouraged to select all appropriate responses. The list included a fictional response option of “citrene headache” to determine incorrect responses. For this study, researchers deemed it necessary to recognize a chronic migraine diagnosis to ensure that patients received appropriate treatment.
- Minimally appropriate pharmacologic treatment. Researchers used the following question to determine whether patients’ chronic migraine and episodic migraine were being managed with the least amount of pharmacological treatment necessary. “Which of these medications (if any) are you currently using (or typically keep on hand) to treat your headaches when you have them?” Researchers defined “minimally appropriate acute pharmacologic treatment” as the use of any prescription nonsteroidal anti-inflammatory drug (NSAID), triptan, ergotamine derivative, or isometheptene.
- Avoidance of medication overuse. The study authors pointed out the sometimes nebulous process of characterizing the appropriate use of preventative medication in patients with episodic migraines as “not straightforward” for some patients because not all patients require preventive treatment. Study participants were required to report having received any form of preventative therapy, defined as pharmacological therapies approved by guidelines and supported by data. Such therapies included various antiseizure medication, antidepressants (for example, doxepin, venlafaxine, duloxetine, amitriptyline, imipramine, nortriptyline, and desvenlafaxine), antihypertensives, and toxin injections. Treatments such as behavioral and neuromodulatory therapies were excluded from the list.
According to lead author Dawn C. Buse, PhD, of the department of neurology at Albert Einstein College of Medicine, New York, acute medication overuse provides an important modifiable target for intervention and recommends that clinicians use the opportunity to optimize migraine care by reducing the patients’ reliance on acute therapies. Taking such initiatives to decrease medication overuse is especially important in communities of color, who are more likely to overuse medications for migraines.
Patients with higher income levels were more likely to overcome each barrier. People of African, African American, or multiracial descent were more prone to overuse of medications to manage their migraines.
Of the 489,537 respondents invited to participate in the CaMEO study, 16,879 qualified for inclusion. Slightly more than half of the respondents (n = 9,184 [54.7%]) had a migraine-related disability (MIDAS) score of 6 or greater – an indicator of disability that is least mild in nature. Most patients who had episodic migraines or chronic migraines (86.2%) had some form of health insurance coverage (n = 9.184; 84.1%; P = .048). Of those patients who were insured, 7,930 patients experienced episodic migraine (86.3%) and the remainder had chronic migraine (n = 1,254; 13.7%). Higher-income patients were more likely to traverse barriers to care. While patients of African descent had higher consultation rates, they also had higher rates of acute medication overuse.
Patients with chronic migraine were more likely to be older than patients with episodic migraine (41.0 vs. 39.6 years; P = .0001) and female (83.0% vs. 79.0%; P = .001), and White (84.5% vs. 79.1%; P < .001). Similarly, patients with chronic migraine were more likely to have a higher mean body mass index (29.8 kg/m2 vs. 28.9 kg/m2; P < .001) and lower rates of full- or part-time employment (56.8% vs. 67.1%; P < .001), and were less likely to have a 4-year degree (64.8 vs. 55.6; P < .001) and annual household incomes below $75,000 (72.6% vs. 64.6%; P < .001). Approximately three-quarters of the patients with episodic migraine (75.7%; 1655/2187) and one-third of patients with chronic migraine (32.8%; 168/512) received accurate diagnoses.
The data uncovered an association with acute medication overuse. Among current consulters who had received an accurate diagnosis and minimally adequate treatment, medication overuse rates were highest among those reporting two or more races (53%) and Blacks and African Americans (45%) and lowest among Whites (33%) and those categorized as “other” race (32%). Ethnic and cultural differences in headache literacy may contribute to differences in medication overuse.
Strategies to improve outcomes
Both Dr. Buse and Dr. McAllister see the value advocacy and education offer in helping to improve outcomes in marginalized communities and other groups negatively impacted by various barriers.
“Patient advocacy and outreach are key here, especially in those traditionally underrepresented in the migraine space, such as men, people of color, blue-collar workers, etc.,” Dr. McAllister noted.
Dr. Buse emphasized the importance of education for patients and health care professionals alike. “A large percentage of people who meet criteria for migraine in the U.S. do not seek care or possibly even know that they have migraines,” Dr. Buse said. “This finding underscores the importance of public health education about migraine as well as well as providing migraine support, education, and resources to health care professionals on the front lines.”
Other strategies recommended by Dr, Buse to ease the impact of barriers include encouraging patient discussion, setting up time for follow-up appointments and education, referring patients for neurological and other specialty consults when warranted, reviewing essential lifestyle habits for migraine management, and creating personalized, mutually agreed-upon treatment plans.
Dr. Buse has received support and honoraria from AbbVie, Amgen, Avanir, Biohaven, Eli Lilly, and Promius.
FROM HEADACHE
BERENICE: Further evidence of heart safety of dual HER2 blockade
Dual HER2 blockade with pertuzumab (Perjeta) and trastuzumab (Herceptin) on top of anthracycline-based neoadjuvant chemotherapy for early-stage breast cancer was associated with a low rate of clinically relevant cardiac events in the final follow-up of the BERENICE study.
After more than 5 years, 1.0%-1.5% of patients who had locally advanced, inflammatory, or early-stage breast cancer developed heart failure, and around 12%-13% showed any significant changes in left ventricular ejection fraction (LVEF).
Importantly, “there were no new safety concerns that arose during long-term follow-up,” study investigator Chau Dang, MD, said in presenting the findings at the European Society for Medical Oncology: Breast Cancer virtual meeting.
Dr. Dang, a medical oncologist at Memorial Sloan Kettering Cancer Centre in New York, reported that the most common cause of death was disease progression.
BERENICE was designed as a cardiac safety study and so not powered to look at long-term efficacy, which Dr. Dang was clear in reporting. Nevertheless event-free survival (EFS), invasive disease-free survival (IDFS), and overall survival (OS) rates at 5 years were all high, at least a respective 89.2%, 91%, and 93.8%, she said. “The medians have not been reached,” she observed.
“These data support the use of dual HER2 blockade with pertuzumab-trastuzumab–based regimens, including in combination with dose-dense, anthracycline-based chemotherapy, across the neoadjuvant and adjuvant treatment settings for the complete treatment of patients with HER2-positive early-stage breast cancer,” Dr. Dang said.
Evandro de Azambuja, MD, PhD, the invited discussant for the trial agreed that the regimens tested appeared “safe from a cardiac standpoint.” However, “you cannot forget that today we are using much less anthracyclines in our patient population.”
Patients in trials are also very different from those treated in clinical practice, often being younger and much fitter, he said. Therefore, it may be important to look at the baseline cardiac medications and comorbidities, Dr. de Azambuja, a medical oncologist at the Institut Jules Bordet in Brussels, Belgium, suggested.
That said, the BERENICE findings sit well with other trials that have been conducted, Dr. de Azambuja pointed out.
“If we look at other trials that have also tested dual HER2 blockade with anthracycline or nonanthracycline regimens, all of them reassure that dual blockade is not more cardiotoxic than single blockade,” he said. This includes trials such as TRYPHAENA, APHINITY, KRISTINE, NeoSphere and PEONY.
The 3-year IDFS rate of 91% in BERENICE also compares well to that seen in APHINITY (94%), Dr. de Azambuja said.
BERENICE study design
BERENICE was a multicenter, open-label, nonrandomized and noncomparative phase 2 trial that recruited 400 patients across 75 centers in 12 countries.
Eligibility criteria were that participants had to have been centrally confirmed HER2-positive locally advanced, inflammatory or early breast cancer, with the latter defined as tumors bigger than 2 cm or greater than 5 mm in size, and be node-positive. Patients also had to have a starting LVEF of 55% or higher.
Patients were allocated to one of two neoadjuvant chemotherapy regimens depending on the choice of their physician. One group received a regimen of dose-dense doxorubicin and cyclophosphamide (ddAC) given every 2 weeks for four cycles and then paclitaxel every week for 12 cycles. The other group received 5-fluorouracil, epirubicin, and cyclophosphamide (FEC) every 3 weeks for four cycles and then docetaxel every 3 weeks for four cycles.
Pertuzumab and trastuzumab were started at the same time as the taxanes in both groups and given every 3 weeks for four cycles. Patients then underwent surgery and continued pertuzumab/trastuzumab treatment alone for a further 13 cycles.
The co-primary endpoints were the incidence of New York Heart Association class III or IV heart failure and incidence of symptomatic and asymptomatic LVEF decline of 10% or more.
The primary analysis of the trial was published in 2018 and, at that time, it was reported that three patients in the ddAC cohort and none in the FEC cohort experienced heart failure. LVEF decline was observed in a respective 6.5% and 2% of patients.
Discussion points
Dr. de Azambuja noted that the contribution of the chemotherapy to the efficacy cannot be assessed because of the nonrandomized trial design. That should not matter, pointed out Sybille Loibl, MD, PhD, during discussion.
“I think it compares nicely to other trials that looked at dose-dense chemotherapy,” said Dr. Loibl, who is an associate professor at the University of Frankfurt in Germany. “It seems that, in the light of what we consider today probably one of the best anti-HER2 treatments, the chemotherapy is less relevant, and that’s why a dose-dense regimen doesn’t add so much on a standard anthracycline taxane-containing regimen.”
Dr. de Azambuja also commented on the assessment of cardiotoxicity and the use of reduced LVEF as a measure: LVEF decline is a late effect of cardiotoxicity, he observed, and he suggested a different approach in future trials.
“If you use Global Longitudinal Strain, this could be an optimal parameter to detect early subclinical LVEF dysfunction and you should consider it for the next trials looking for cardiac safety. Also, cardiac biomarkers. This was not implemented in this trial, and I strongly recommend this should be for the next trial.”
The BERENICE trial was funded by F. Hoffmann-La Roche. Dr. Dang disclosed receiving consultancy fees from F. Hoffmann-La Roche, Genentech, Daiichi Sankyo, Lilly, and Puma Biotechnology. Dr. de Azambuja was not involved in the study but disclosed receiving honoraria, travel grants, research grants from Roche and Genentech as well as from other companies. Dr. Loibl was one of the cochairs of the session and, among disclosures regarding many other companies, has been an invited speaker for Roche and received reimbursement via her institution for a writing engagement.
Dual HER2 blockade with pertuzumab (Perjeta) and trastuzumab (Herceptin) on top of anthracycline-based neoadjuvant chemotherapy for early-stage breast cancer was associated with a low rate of clinically relevant cardiac events in the final follow-up of the BERENICE study.
After more than 5 years, 1.0%-1.5% of patients who had locally advanced, inflammatory, or early-stage breast cancer developed heart failure, and around 12%-13% showed any significant changes in left ventricular ejection fraction (LVEF).
Importantly, “there were no new safety concerns that arose during long-term follow-up,” study investigator Chau Dang, MD, said in presenting the findings at the European Society for Medical Oncology: Breast Cancer virtual meeting.
Dr. Dang, a medical oncologist at Memorial Sloan Kettering Cancer Centre in New York, reported that the most common cause of death was disease progression.
BERENICE was designed as a cardiac safety study and so not powered to look at long-term efficacy, which Dr. Dang was clear in reporting. Nevertheless event-free survival (EFS), invasive disease-free survival (IDFS), and overall survival (OS) rates at 5 years were all high, at least a respective 89.2%, 91%, and 93.8%, she said. “The medians have not been reached,” she observed.
“These data support the use of dual HER2 blockade with pertuzumab-trastuzumab–based regimens, including in combination with dose-dense, anthracycline-based chemotherapy, across the neoadjuvant and adjuvant treatment settings for the complete treatment of patients with HER2-positive early-stage breast cancer,” Dr. Dang said.
Evandro de Azambuja, MD, PhD, the invited discussant for the trial agreed that the regimens tested appeared “safe from a cardiac standpoint.” However, “you cannot forget that today we are using much less anthracyclines in our patient population.”
Patients in trials are also very different from those treated in clinical practice, often being younger and much fitter, he said. Therefore, it may be important to look at the baseline cardiac medications and comorbidities, Dr. de Azambuja, a medical oncologist at the Institut Jules Bordet in Brussels, Belgium, suggested.
That said, the BERENICE findings sit well with other trials that have been conducted, Dr. de Azambuja pointed out.
“If we look at other trials that have also tested dual HER2 blockade with anthracycline or nonanthracycline regimens, all of them reassure that dual blockade is not more cardiotoxic than single blockade,” he said. This includes trials such as TRYPHAENA, APHINITY, KRISTINE, NeoSphere and PEONY.
The 3-year IDFS rate of 91% in BERENICE also compares well to that seen in APHINITY (94%), Dr. de Azambuja said.
BERENICE study design
BERENICE was a multicenter, open-label, nonrandomized and noncomparative phase 2 trial that recruited 400 patients across 75 centers in 12 countries.
Eligibility criteria were that participants had to have been centrally confirmed HER2-positive locally advanced, inflammatory or early breast cancer, with the latter defined as tumors bigger than 2 cm or greater than 5 mm in size, and be node-positive. Patients also had to have a starting LVEF of 55% or higher.
Patients were allocated to one of two neoadjuvant chemotherapy regimens depending on the choice of their physician. One group received a regimen of dose-dense doxorubicin and cyclophosphamide (ddAC) given every 2 weeks for four cycles and then paclitaxel every week for 12 cycles. The other group received 5-fluorouracil, epirubicin, and cyclophosphamide (FEC) every 3 weeks for four cycles and then docetaxel every 3 weeks for four cycles.
Pertuzumab and trastuzumab were started at the same time as the taxanes in both groups and given every 3 weeks for four cycles. Patients then underwent surgery and continued pertuzumab/trastuzumab treatment alone for a further 13 cycles.
The co-primary endpoints were the incidence of New York Heart Association class III or IV heart failure and incidence of symptomatic and asymptomatic LVEF decline of 10% or more.
The primary analysis of the trial was published in 2018 and, at that time, it was reported that three patients in the ddAC cohort and none in the FEC cohort experienced heart failure. LVEF decline was observed in a respective 6.5% and 2% of patients.
Discussion points
Dr. de Azambuja noted that the contribution of the chemotherapy to the efficacy cannot be assessed because of the nonrandomized trial design. That should not matter, pointed out Sybille Loibl, MD, PhD, during discussion.
“I think it compares nicely to other trials that looked at dose-dense chemotherapy,” said Dr. Loibl, who is an associate professor at the University of Frankfurt in Germany. “It seems that, in the light of what we consider today probably one of the best anti-HER2 treatments, the chemotherapy is less relevant, and that’s why a dose-dense regimen doesn’t add so much on a standard anthracycline taxane-containing regimen.”
Dr. de Azambuja also commented on the assessment of cardiotoxicity and the use of reduced LVEF as a measure: LVEF decline is a late effect of cardiotoxicity, he observed, and he suggested a different approach in future trials.
“If you use Global Longitudinal Strain, this could be an optimal parameter to detect early subclinical LVEF dysfunction and you should consider it for the next trials looking for cardiac safety. Also, cardiac biomarkers. This was not implemented in this trial, and I strongly recommend this should be for the next trial.”
The BERENICE trial was funded by F. Hoffmann-La Roche. Dr. Dang disclosed receiving consultancy fees from F. Hoffmann-La Roche, Genentech, Daiichi Sankyo, Lilly, and Puma Biotechnology. Dr. de Azambuja was not involved in the study but disclosed receiving honoraria, travel grants, research grants from Roche and Genentech as well as from other companies. Dr. Loibl was one of the cochairs of the session and, among disclosures regarding many other companies, has been an invited speaker for Roche and received reimbursement via her institution for a writing engagement.
Dual HER2 blockade with pertuzumab (Perjeta) and trastuzumab (Herceptin) on top of anthracycline-based neoadjuvant chemotherapy for early-stage breast cancer was associated with a low rate of clinically relevant cardiac events in the final follow-up of the BERENICE study.
After more than 5 years, 1.0%-1.5% of patients who had locally advanced, inflammatory, or early-stage breast cancer developed heart failure, and around 12%-13% showed any significant changes in left ventricular ejection fraction (LVEF).
Importantly, “there were no new safety concerns that arose during long-term follow-up,” study investigator Chau Dang, MD, said in presenting the findings at the European Society for Medical Oncology: Breast Cancer virtual meeting.
Dr. Dang, a medical oncologist at Memorial Sloan Kettering Cancer Centre in New York, reported that the most common cause of death was disease progression.
BERENICE was designed as a cardiac safety study and so not powered to look at long-term efficacy, which Dr. Dang was clear in reporting. Nevertheless event-free survival (EFS), invasive disease-free survival (IDFS), and overall survival (OS) rates at 5 years were all high, at least a respective 89.2%, 91%, and 93.8%, she said. “The medians have not been reached,” she observed.
“These data support the use of dual HER2 blockade with pertuzumab-trastuzumab–based regimens, including in combination with dose-dense, anthracycline-based chemotherapy, across the neoadjuvant and adjuvant treatment settings for the complete treatment of patients with HER2-positive early-stage breast cancer,” Dr. Dang said.
Evandro de Azambuja, MD, PhD, the invited discussant for the trial agreed that the regimens tested appeared “safe from a cardiac standpoint.” However, “you cannot forget that today we are using much less anthracyclines in our patient population.”
Patients in trials are also very different from those treated in clinical practice, often being younger and much fitter, he said. Therefore, it may be important to look at the baseline cardiac medications and comorbidities, Dr. de Azambuja, a medical oncologist at the Institut Jules Bordet in Brussels, Belgium, suggested.
That said, the BERENICE findings sit well with other trials that have been conducted, Dr. de Azambuja pointed out.
“If we look at other trials that have also tested dual HER2 blockade with anthracycline or nonanthracycline regimens, all of them reassure that dual blockade is not more cardiotoxic than single blockade,” he said. This includes trials such as TRYPHAENA, APHINITY, KRISTINE, NeoSphere and PEONY.
The 3-year IDFS rate of 91% in BERENICE also compares well to that seen in APHINITY (94%), Dr. de Azambuja said.
BERENICE study design
BERENICE was a multicenter, open-label, nonrandomized and noncomparative phase 2 trial that recruited 400 patients across 75 centers in 12 countries.
Eligibility criteria were that participants had to have been centrally confirmed HER2-positive locally advanced, inflammatory or early breast cancer, with the latter defined as tumors bigger than 2 cm or greater than 5 mm in size, and be node-positive. Patients also had to have a starting LVEF of 55% or higher.
Patients were allocated to one of two neoadjuvant chemotherapy regimens depending on the choice of their physician. One group received a regimen of dose-dense doxorubicin and cyclophosphamide (ddAC) given every 2 weeks for four cycles and then paclitaxel every week for 12 cycles. The other group received 5-fluorouracil, epirubicin, and cyclophosphamide (FEC) every 3 weeks for four cycles and then docetaxel every 3 weeks for four cycles.
Pertuzumab and trastuzumab were started at the same time as the taxanes in both groups and given every 3 weeks for four cycles. Patients then underwent surgery and continued pertuzumab/trastuzumab treatment alone for a further 13 cycles.
The co-primary endpoints were the incidence of New York Heart Association class III or IV heart failure and incidence of symptomatic and asymptomatic LVEF decline of 10% or more.
The primary analysis of the trial was published in 2018 and, at that time, it was reported that three patients in the ddAC cohort and none in the FEC cohort experienced heart failure. LVEF decline was observed in a respective 6.5% and 2% of patients.
Discussion points
Dr. de Azambuja noted that the contribution of the chemotherapy to the efficacy cannot be assessed because of the nonrandomized trial design. That should not matter, pointed out Sybille Loibl, MD, PhD, during discussion.
“I think it compares nicely to other trials that looked at dose-dense chemotherapy,” said Dr. Loibl, who is an associate professor at the University of Frankfurt in Germany. “It seems that, in the light of what we consider today probably one of the best anti-HER2 treatments, the chemotherapy is less relevant, and that’s why a dose-dense regimen doesn’t add so much on a standard anthracycline taxane-containing regimen.”
Dr. de Azambuja also commented on the assessment of cardiotoxicity and the use of reduced LVEF as a measure: LVEF decline is a late effect of cardiotoxicity, he observed, and he suggested a different approach in future trials.
“If you use Global Longitudinal Strain, this could be an optimal parameter to detect early subclinical LVEF dysfunction and you should consider it for the next trials looking for cardiac safety. Also, cardiac biomarkers. This was not implemented in this trial, and I strongly recommend this should be for the next trial.”
The BERENICE trial was funded by F. Hoffmann-La Roche. Dr. Dang disclosed receiving consultancy fees from F. Hoffmann-La Roche, Genentech, Daiichi Sankyo, Lilly, and Puma Biotechnology. Dr. de Azambuja was not involved in the study but disclosed receiving honoraria, travel grants, research grants from Roche and Genentech as well as from other companies. Dr. Loibl was one of the cochairs of the session and, among disclosures regarding many other companies, has been an invited speaker for Roche and received reimbursement via her institution for a writing engagement.
FROM ESMO BREAST CANCER 2021
Headache on the Hill goes virtual
Participants in the Alliance for Headache Disorders Advocacy session requested federal funding for headache research and treatment. While patients told their stories, a noted advocate said headache is “an eminently solvable problem, but the urgency is now.”

It is going to take more than a pandemic to stop key headache advocacy stakeholders from raising awareness of the devastating impact of migraine and cluster headache and to motivate Congress to act.
With COVID-19 still very much a part of our lives, the Alliance for Headache Disorders Advocacy (AHDA)—a nonprofit dedicated to advocating for equitable policies for people with headache disorders—moved forward with its annual Headache on the Hill advocacy day, which took place virtually for the first time via videoconferencing on March 23, 2021.
While participants missed the opportunity to travel to Washington to meet with key legislators face-to-face, optimists saw it as a chance to involve more patients, providers, researchers, and caregivers who otherwise would not be able to participate. Indeed, more were involved than ever before: 217 individuals from 47 states and 178 Congressional districts attended, meeting with influential lawmakers, including Senator Patrick Leahy (D-VT), chair of the Appropriations Committee; Senator Richard Shelby (R-AL), vice chair of the Appropriations Committee; Rep. Rose DeLauro (D-CT), chair of the House Committee on Appropriations; Senator Jon Tester (D-MT), chair of Senate Committee on Veterans’ Affairs; Senator Jerry Moran (R-KS), ranking member of the Senate Committee on Veterans’ Affairs; Senator Patty Murray (D-WA), chair of the Senate HELP Committee; and Senator Richard Burr (R-NC), ranking member of the Senate HELP Committee.
I have had the privilege of being a part of Headache on the Hill for 13 years and was pleased to participate in this year’s virtual event. Though the setting was different, our mission remained the same: to make our important legislative requests (“asks”) of as many offices in Congress as possible. This year, we had 2 asks that aim to improve headache research and access to treatment, especially for our Veterans:
- Increased research funding: The group requested that the National Institutes of Health (NIH) Helping to End Addiction Long-Term (HEAL) initiative focus on headache disorders to reduce disease burden and opioid prescribing. This would make more funding available for headache research.
- Improved treatment access: The group also asked Congress to fully fund Veterans Health Administration (VHA) Headache Disorders Centers of Excellence (HCoE), facilitating equitable access to care for disabled veterans. This would double the number of VA Centers of Excellence to treat headache disorders in our veterans.
Of course, getting results means more than simply asking. The request to our congresspeople and their staff is more likely to succeed if it is well-reasoned and backed by evidence; and the Headache on the Hill contingent delivered on these requirements.
Why Congress should direct HEAL to focus on headache disorders:
- Headache disorders are extraordinarily burdensome. As most of us know (but not all legislators are aware), 60 million Americans suffer from migraine headache; it is the second leading cause of disability lifetime in the world.1 Additionally, cluster headache is thought to be the most severe type of pain humans can experience.2
- There is a critical need for more effective and safer treatments for headache disorders. Opioid use is known to worsen migraine frequency and severity for some and make medications for headache less effective.3 Guidelines uniformly recommend against treating migraine with opioids; yet somehow 10% of migraine sufferers actively use opioids,4 and nearly 60% receive opioids during visits to the emergency room.5
- NIH has underfunded research on headache disorders. NIH has not prioritized programs for headache disorders research despite the fact that since 2009, 17 appropriations report language statements have strongly urged NIH to do so.6 In fact, headache is the least-funded research area among the most burdensome diseases.7,8 Instead, other important disorders were funded, even though Headache on the Hill advocacy arranged for the report language for headache.
- Statutory authority for the HEAL initiative calls for disease burden to be a “crucial consideration” in prioritizing research programs. Less than 1% of HEAL grants have been for headache disorders research.10 If disease burden was used as the only gauge for funding, NIH investment for migraine research would likely be 15 times higher than the roughly $20 million that has historically been allocated.9 We hope our work this year will get us where we need to be.
Why Congress should fully fund VHA Headache Disorders Centers of Excellence
- Headache disorders are a major health issue for veterans. Some 350,000 Global War on Terror (GWOT) veterans have sustained traumatic brain injuries. Many of them experience headaches. In fact, research shows that half of these veterans reported 15 or more headache days per month 4 to 11 years after sustaining traumatic brain injury. Nine of every 10 veterans met the criteria for migraine.10 Moreover, 3 million GWOT veterans have been exposed to toxic open burn pits.11 These individuals have been found to be twice as likely to experience functional limitations due to migraine than those who did not have burn pit duties.12
- Headache Centers of Excellence (HCoEs) work. In 2018, $10 million was appropriated to establish at least 5 HCoEs that provided 1) comprehensive direct patient specialized headache medicine care within the VHA; 2) consultation and referral specialized headache care centers within the VHA; 3) education and training of VHA healthcare providers in headache medicine; and 4) research to improve the quality of headache disorders care for veterans and civilians.13
- Fourteen sites now exist, and success continues to be demonstrated. Last year more than 400,000 veterans sought specialty care for headache disorders from the VHA.14 However, only half of these vets are within reasonable reach of a HCoE.
The asks
Armed with this evidence, we made specific asks of the House and Senate with respect to annual appropriations spending bills:
- Legislators were asked to sign on to a letter or send their own letter to officials on the House and Senate Labor, Health and Human Services, Education, and Related Agencies appropriations subcommittees to allocate $50 million from the HEAL initiative for headache disorders research in fiscal year 2022.
- Similarly, lawmakers were asked to sign onto a letter or send their own letter to members of the Military Construction and Veterans Affairs subcommittee to appropriate $25 million to fund a doubling of HCoEs from 14 to 28 to improve access to those seeking care for headache disorders.
Stories from Americans nationwide
Headache on the Hill is about more than just presenting evidence and making requests. If that were the case, there is a pretty good chance that, before long, legislators would be looking at their watches, checking their smartphones, and flashing knowing glances at their aides in an effort to cut things short. However, humanizing the topic by sharing stories of the toll migraine and cluster headaches take on individuals is compelling testimony that hopefully will lead to meaningful action and positive outcomes. Here is a sampling of the stories told during and after the Headache on the Hill session:
- Rachel Koh and Ronetta Stokes: Koh registered for both the 2019 and 2020 Headache on the Hill sessions, only to be forced to cancel due to migraine attacks. But this year, according to the American Migraine Foundation, she was able to participate virtually and tell her representatives why increased funding was important for her, as well as veterans, including her father and uncle. Meanwhile, Stokes, a first-time participant, said she was struck by the conversations she had with legislators. Most knew someone with migraine, and some were sufferers themselves. “The more we share and spread the word, the sooner we can end the stigma,” Stokes told the American Migraine Foundation.
- Mia Maysack: Maysack wrote about her experience in a column for Pain News Network. “I live with both migraine disease and cluster headaches, which are called ‘suicide headaches’ for good reason,” she wrote. “There’s no limit to the chaos, interruption, inconvenience, and discomfort these conditions have caused in my life, requiring my full-time attention just to manage the symptoms. The difficult experiences I and countless others have faced in seeking, finding, and attempting different forms of treatment is why I continue to advocate—even when I don't feel up to it.” Maysack added that although it is relatively easy for her to receive a medication prescription for her condition, she’d like to see more consideration given to treatments such as water therapy, massage, oxygen, and mindful meditation.
- Chloe Vruno: Vruno, a 21-year-old college student, has suffered with migraine since the age of 15. “Some days are worse than others,” she noted in an article in her local newspaper, the Steuben County, IN Herald Republican. “Most days I have to push through a migraine to make it to class, but some days are so severe that I cannot make it to classes. On days I cannot make it, I use my accommodation for attendance flexibility, or now with COVID, I Zoom into class from my room.” Vruno wanted to make her representatives aware of these types of disruptions, a regular occurrence for migraine sufferers like her. This was her second Headache on the Hill event, and she found lawmakers whom she spoke with to be “extremely attentive, engaged, and excited.”
“A moral imperative”
Stories like these from regular individuals across the United States who suffer from headache disorders go a long way in convincing legislators to act. It also helps to tap into a celebrity’s endorsement when you can. Headache on the Hill did not disappoint in this regard, with Jon Stewart, the former host of The Daily Show, appearing as a special guest during a policy panel discussion on chronic headache disorders and toxic exposure. The session, which took place virtually as part of Headache on the Hill, featured Stewart, a national advocate for service personnel with toxic exposures, and Rep. Mark Takano (D-CA), who delivered the keynote address. The panel discussion included first responders, veterans, and clinicians.
Stewart summed up the sentiments of all Headache on the Hill stakeholders this way: “This is an eminently solvable problem, but the urgency is now. People will continue to suffer needlessly if we don’t get this done. It is a moral imperative that we pass a bill on presumption as soon as possible.”
I always enjoy going to Washington on cold days in February to be part of Headache on the Hill, and I hope we will be back in-person next year. We have tripled the number of attendees over the last 13 years and have a higher percentage of great patients and advocates now. I have to give a special thanks to Dr. Bob Shapiro, Professor of Neurology at the University of Vermont, who started and has guided this phenomenal effort over the years, to Dr. Chris Gottschalk, Professor of Neurology at Yale, who is gradually taking over the reins, and to Katie MacDonald who runs the entire show, even though she suffers from chronic migraine on a daily basis.
1. Global Health Data Exchange. Global Burden of Disease Study 2019 (GBD 2019) Data Resources. http://ghdx.healthdata.org/gbd-2019. Accessed April 12, 2021.
2.Burish MJ, Pearson SM, RE Shapiro, et al. Cluster headache is one of the most intensely painful human conditions: Results from the International Cluster Headache Questionnaire. Headache. 2021;61:117-124.
3. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71:1821-1828.
4. Lipton RB, Buse DB, Dodick DW, et al. Burden of increasing opioid use in the treatment of migraine: Results from the Migraine in America Symptoms and Treatment Study. Headache. 2020;61:103-116.
5. Friedman BW, West J, Vinson DR, et al. Current management of migraine in US emergency departments: An analysis of the National Hospital Ambulatory Medical Care Survey. Cephalalgia. 2015;35:301-309.
6. Shapiro RE. What will it take to move the needle for headache disorders? An advocacy perspective. Headache. 2020;60:2059-2077.
7. NIH RePORT. Report on NIH funding vs. global burden of disease. https://report.nih.gov/report-nih-funding-vs-global-burden-disease. Accessed April 12, 2021.
8. NIH RePORT. Estimates of funding for various research, condition, and disease categories (RCDC). https://report.nih.gov/funding/categorical-spending#/. Published February 24, 2020. Accessed April 12, 2021.
9. National Institutes of Health. Funded projects. https://heal.nih.gov/funding/awarded. Updated March 18, 2020. Accessed April 12, 2021.
10. Couch JR, Stewart KE. Headache prevalence at 4-11 years after deployment-related traumatic brain injury in veterans of Iraq and Afghanistan wars and comparison to controls: A matched case-controlled study. Headache 2016;56:1004-1021.
11. Dr. Richard A. Stone, Acting Under Secretary for Health. Message to Staff-Airborne Hazards and Open Burn Pit Registry. https://players.brightcove.net/2851863979001/default_default/index.html?videoId=6228317154001. Published February 2021. Accessed April 12, 2021.
12. US Department of Veterans Affairs. Report on Data from the Airborne Hazards and Open Burn Pit (AH&OBP) Registry. https://www.publichealth.va.gov/docs/exposures/va-ahobp-registry-data-report-june2015.pdf#. Published June 2015. Accessed April 12, 2021.
13. US Government Publishing Office. Military construction, Veterans Affairs, and related agencies appropriation bill, 2018. https://www.appropriations.senate.gov/imo/media/doc/FY2018%20MiliCon-VA%20Bill%20S1557.pdf. Published July 13, 2017. Accessed April 12, 2021.
14. Fenton BT, Lindsey H, Grinberg AS, et al. Presentation given at: 62nd Annual Scientific Meeting American Headache Society- Prevalence of Headache and Comorbidities Among Men and Women Veterans Across the Veterans Health Administration – a 10‐year Cohort Study. VA Connecticut Healthcare System, West Haven, CT; Yale School of Medicine, West Haven, CT; 3Yeshiva University, Bronx, NY. https://headachejournal.onlinelibrary.wiley.com/doi/full/10.1111/head.13854. Published June 13, 2020. Accessed April 12, 2021.
Participants in the Alliance for Headache Disorders Advocacy session requested federal funding for headache research and treatment. While patients told their stories, a noted advocate said headache is “an eminently solvable problem, but the urgency is now.”
It is going to take more than a pandemic to stop key headache advocacy stakeholders from raising awareness of the devastating impact of migraine and cluster headache and to motivate Congress to act.
With COVID-19 still very much a part of our lives, the Alliance for Headache Disorders Advocacy (AHDA)—a nonprofit dedicated to advocating for equitable policies for people with headache disorders—moved forward with its annual Headache on the Hill advocacy day, which took place virtually for the first time via videoconferencing on March 23, 2021.
While participants missed the opportunity to travel to Washington to meet with key legislators face-to-face, optimists saw it as a chance to involve more patients, providers, researchers, and caregivers who otherwise would not be able to participate. Indeed, more were involved than ever before: 217 individuals from 47 states and 178 Congressional districts attended, meeting with influential lawmakers, including Senator Patrick Leahy (D-VT), chair of the Appropriations Committee; Senator Richard Shelby (R-AL), vice chair of the Appropriations Committee; Rep. Rose DeLauro (D-CT), chair of the House Committee on Appropriations; Senator Jon Tester (D-MT), chair of Senate Committee on Veterans’ Affairs; Senator Jerry Moran (R-KS), ranking member of the Senate Committee on Veterans’ Affairs; Senator Patty Murray (D-WA), chair of the Senate HELP Committee; and Senator Richard Burr (R-NC), ranking member of the Senate HELP Committee.
I have had the privilege of being a part of Headache on the Hill for 13 years and was pleased to participate in this year’s virtual event. Though the setting was different, our mission remained the same: to make our important legislative requests (“asks”) of as many offices in Congress as possible. This year, we had 2 asks that aim to improve headache research and access to treatment, especially for our Veterans:
- Increased research funding: The group requested that the National Institutes of Health (NIH) Helping to End Addiction Long-Term (HEAL) initiative focus on headache disorders to reduce disease burden and opioid prescribing. This would make more funding available for headache research.
- Improved treatment access: The group also asked Congress to fully fund Veterans Health Administration (VHA) Headache Disorders Centers of Excellence (HCoE), facilitating equitable access to care for disabled veterans. This would double the number of VA Centers of Excellence to treat headache disorders in our veterans.
Of course, getting results means more than simply asking. The request to our congresspeople and their staff is more likely to succeed if it is well-reasoned and backed by evidence; and the Headache on the Hill contingent delivered on these requirements.
Why Congress should direct HEAL to focus on headache disorders:
- Headache disorders are extraordinarily burdensome. As most of us know (but not all legislators are aware), 60 million Americans suffer from migraine headache; it is the second leading cause of disability lifetime in the world.1 Additionally, cluster headache is thought to be the most severe type of pain humans can experience.2
- There is a critical need for more effective and safer treatments for headache disorders. Opioid use is known to worsen migraine frequency and severity for some and make medications for headache less effective.3 Guidelines uniformly recommend against treating migraine with opioids; yet somehow 10% of migraine sufferers actively use opioids,4 and nearly 60% receive opioids during visits to the emergency room.5
- NIH has underfunded research on headache disorders. NIH has not prioritized programs for headache disorders research despite the fact that since 2009, 17 appropriations report language statements have strongly urged NIH to do so.6 In fact, headache is the least-funded research area among the most burdensome diseases.7,8 Instead, other important disorders were funded, even though Headache on the Hill advocacy arranged for the report language for headache.
- Statutory authority for the HEAL initiative calls for disease burden to be a “crucial consideration” in prioritizing research programs. Less than 1% of HEAL grants have been for headache disorders research.10 If disease burden was used as the only gauge for funding, NIH investment for migraine research would likely be 15 times higher than the roughly $20 million that has historically been allocated.9 We hope our work this year will get us where we need to be.
Why Congress should fully fund VHA Headache Disorders Centers of Excellence
- Headache disorders are a major health issue for veterans. Some 350,000 Global War on Terror (GWOT) veterans have sustained traumatic brain injuries. Many of them experience headaches. In fact, research shows that half of these veterans reported 15 or more headache days per month 4 to 11 years after sustaining traumatic brain injury. Nine of every 10 veterans met the criteria for migraine.10 Moreover, 3 million GWOT veterans have been exposed to toxic open burn pits.11 These individuals have been found to be twice as likely to experience functional limitations due to migraine than those who did not have burn pit duties.12
- Headache Centers of Excellence (HCoEs) work. In 2018, $10 million was appropriated to establish at least 5 HCoEs that provided 1) comprehensive direct patient specialized headache medicine care within the VHA; 2) consultation and referral specialized headache care centers within the VHA; 3) education and training of VHA healthcare providers in headache medicine; and 4) research to improve the quality of headache disorders care for veterans and civilians.13
- Fourteen sites now exist, and success continues to be demonstrated. Last year more than 400,000 veterans sought specialty care for headache disorders from the VHA.14 However, only half of these vets are within reasonable reach of a HCoE.
The asks
Armed with this evidence, we made specific asks of the House and Senate with respect to annual appropriations spending bills:
- Legislators were asked to sign on to a letter or send their own letter to officials on the House and Senate Labor, Health and Human Services, Education, and Related Agencies appropriations subcommittees to allocate $50 million from the HEAL initiative for headache disorders research in fiscal year 2022.
- Similarly, lawmakers were asked to sign onto a letter or send their own letter to members of the Military Construction and Veterans Affairs subcommittee to appropriate $25 million to fund a doubling of HCoEs from 14 to 28 to improve access to those seeking care for headache disorders.
Stories from Americans nationwide
Headache on the Hill is about more than just presenting evidence and making requests. If that were the case, there is a pretty good chance that, before long, legislators would be looking at their watches, checking their smartphones, and flashing knowing glances at their aides in an effort to cut things short. However, humanizing the topic by sharing stories of the toll migraine and cluster headaches take on individuals is compelling testimony that hopefully will lead to meaningful action and positive outcomes. Here is a sampling of the stories told during and after the Headache on the Hill session:
- Rachel Koh and Ronetta Stokes: Koh registered for both the 2019 and 2020 Headache on the Hill sessions, only to be forced to cancel due to migraine attacks. But this year, according to the American Migraine Foundation, she was able to participate virtually and tell her representatives why increased funding was important for her, as well as veterans, including her father and uncle. Meanwhile, Stokes, a first-time participant, said she was struck by the conversations she had with legislators. Most knew someone with migraine, and some were sufferers themselves. “The more we share and spread the word, the sooner we can end the stigma,” Stokes told the American Migraine Foundation.
- Mia Maysack: Maysack wrote about her experience in a column for Pain News Network. “I live with both migraine disease and cluster headaches, which are called ‘suicide headaches’ for good reason,” she wrote. “There’s no limit to the chaos, interruption, inconvenience, and discomfort these conditions have caused in my life, requiring my full-time attention just to manage the symptoms. The difficult experiences I and countless others have faced in seeking, finding, and attempting different forms of treatment is why I continue to advocate—even when I don't feel up to it.” Maysack added that although it is relatively easy for her to receive a medication prescription for her condition, she’d like to see more consideration given to treatments such as water therapy, massage, oxygen, and mindful meditation.
- Chloe Vruno: Vruno, a 21-year-old college student, has suffered with migraine since the age of 15. “Some days are worse than others,” she noted in an article in her local newspaper, the Steuben County, IN Herald Republican. “Most days I have to push through a migraine to make it to class, but some days are so severe that I cannot make it to classes. On days I cannot make it, I use my accommodation for attendance flexibility, or now with COVID, I Zoom into class from my room.” Vruno wanted to make her representatives aware of these types of disruptions, a regular occurrence for migraine sufferers like her. This was her second Headache on the Hill event, and she found lawmakers whom she spoke with to be “extremely attentive, engaged, and excited.”
“A moral imperative”
Stories like these from regular individuals across the United States who suffer from headache disorders go a long way in convincing legislators to act. It also helps to tap into a celebrity’s endorsement when you can. Headache on the Hill did not disappoint in this regard, with Jon Stewart, the former host of The Daily Show, appearing as a special guest during a policy panel discussion on chronic headache disorders and toxic exposure. The session, which took place virtually as part of Headache on the Hill, featured Stewart, a national advocate for service personnel with toxic exposures, and Rep. Mark Takano (D-CA), who delivered the keynote address. The panel discussion included first responders, veterans, and clinicians.
Stewart summed up the sentiments of all Headache on the Hill stakeholders this way: “This is an eminently solvable problem, but the urgency is now. People will continue to suffer needlessly if we don’t get this done. It is a moral imperative that we pass a bill on presumption as soon as possible.”
I always enjoy going to Washington on cold days in February to be part of Headache on the Hill, and I hope we will be back in-person next year. We have tripled the number of attendees over the last 13 years and have a higher percentage of great patients and advocates now. I have to give a special thanks to Dr. Bob Shapiro, Professor of Neurology at the University of Vermont, who started and has guided this phenomenal effort over the years, to Dr. Chris Gottschalk, Professor of Neurology at Yale, who is gradually taking over the reins, and to Katie MacDonald who runs the entire show, even though she suffers from chronic migraine on a daily basis.
Participants in the Alliance for Headache Disorders Advocacy session requested federal funding for headache research and treatment. While patients told their stories, a noted advocate said headache is “an eminently solvable problem, but the urgency is now.”
It is going to take more than a pandemic to stop key headache advocacy stakeholders from raising awareness of the devastating impact of migraine and cluster headache and to motivate Congress to act.
With COVID-19 still very much a part of our lives, the Alliance for Headache Disorders Advocacy (AHDA)—a nonprofit dedicated to advocating for equitable policies for people with headache disorders—moved forward with its annual Headache on the Hill advocacy day, which took place virtually for the first time via videoconferencing on March 23, 2021.
While participants missed the opportunity to travel to Washington to meet with key legislators face-to-face, optimists saw it as a chance to involve more patients, providers, researchers, and caregivers who otherwise would not be able to participate. Indeed, more were involved than ever before: 217 individuals from 47 states and 178 Congressional districts attended, meeting with influential lawmakers, including Senator Patrick Leahy (D-VT), chair of the Appropriations Committee; Senator Richard Shelby (R-AL), vice chair of the Appropriations Committee; Rep. Rose DeLauro (D-CT), chair of the House Committee on Appropriations; Senator Jon Tester (D-MT), chair of Senate Committee on Veterans’ Affairs; Senator Jerry Moran (R-KS), ranking member of the Senate Committee on Veterans’ Affairs; Senator Patty Murray (D-WA), chair of the Senate HELP Committee; and Senator Richard Burr (R-NC), ranking member of the Senate HELP Committee.
I have had the privilege of being a part of Headache on the Hill for 13 years and was pleased to participate in this year’s virtual event. Though the setting was different, our mission remained the same: to make our important legislative requests (“asks”) of as many offices in Congress as possible. This year, we had 2 asks that aim to improve headache research and access to treatment, especially for our Veterans:
- Increased research funding: The group requested that the National Institutes of Health (NIH) Helping to End Addiction Long-Term (HEAL) initiative focus on headache disorders to reduce disease burden and opioid prescribing. This would make more funding available for headache research.
- Improved treatment access: The group also asked Congress to fully fund Veterans Health Administration (VHA) Headache Disorders Centers of Excellence (HCoE), facilitating equitable access to care for disabled veterans. This would double the number of VA Centers of Excellence to treat headache disorders in our veterans.
Of course, getting results means more than simply asking. The request to our congresspeople and their staff is more likely to succeed if it is well-reasoned and backed by evidence; and the Headache on the Hill contingent delivered on these requirements.
Why Congress should direct HEAL to focus on headache disorders:
- Headache disorders are extraordinarily burdensome. As most of us know (but not all legislators are aware), 60 million Americans suffer from migraine headache; it is the second leading cause of disability lifetime in the world.1 Additionally, cluster headache is thought to be the most severe type of pain humans can experience.2
- There is a critical need for more effective and safer treatments for headache disorders. Opioid use is known to worsen migraine frequency and severity for some and make medications for headache less effective.3 Guidelines uniformly recommend against treating migraine with opioids; yet somehow 10% of migraine sufferers actively use opioids,4 and nearly 60% receive opioids during visits to the emergency room.5
- NIH has underfunded research on headache disorders. NIH has not prioritized programs for headache disorders research despite the fact that since 2009, 17 appropriations report language statements have strongly urged NIH to do so.6 In fact, headache is the least-funded research area among the most burdensome diseases.7,8 Instead, other important disorders were funded, even though Headache on the Hill advocacy arranged for the report language for headache.
- Statutory authority for the HEAL initiative calls for disease burden to be a “crucial consideration” in prioritizing research programs. Less than 1% of HEAL grants have been for headache disorders research.10 If disease burden was used as the only gauge for funding, NIH investment for migraine research would likely be 15 times higher than the roughly $20 million that has historically been allocated.9 We hope our work this year will get us where we need to be.
Why Congress should fully fund VHA Headache Disorders Centers of Excellence
- Headache disorders are a major health issue for veterans. Some 350,000 Global War on Terror (GWOT) veterans have sustained traumatic brain injuries. Many of them experience headaches. In fact, research shows that half of these veterans reported 15 or more headache days per month 4 to 11 years after sustaining traumatic brain injury. Nine of every 10 veterans met the criteria for migraine.10 Moreover, 3 million GWOT veterans have been exposed to toxic open burn pits.11 These individuals have been found to be twice as likely to experience functional limitations due to migraine than those who did not have burn pit duties.12
- Headache Centers of Excellence (HCoEs) work. In 2018, $10 million was appropriated to establish at least 5 HCoEs that provided 1) comprehensive direct patient specialized headache medicine care within the VHA; 2) consultation and referral specialized headache care centers within the VHA; 3) education and training of VHA healthcare providers in headache medicine; and 4) research to improve the quality of headache disorders care for veterans and civilians.13
- Fourteen sites now exist, and success continues to be demonstrated. Last year more than 400,000 veterans sought specialty care for headache disorders from the VHA.14 However, only half of these vets are within reasonable reach of a HCoE.
The asks
Armed with this evidence, we made specific asks of the House and Senate with respect to annual appropriations spending bills:
- Legislators were asked to sign on to a letter or send their own letter to officials on the House and Senate Labor, Health and Human Services, Education, and Related Agencies appropriations subcommittees to allocate $50 million from the HEAL initiative for headache disorders research in fiscal year 2022.
- Similarly, lawmakers were asked to sign onto a letter or send their own letter to members of the Military Construction and Veterans Affairs subcommittee to appropriate $25 million to fund a doubling of HCoEs from 14 to 28 to improve access to those seeking care for headache disorders.
Stories from Americans nationwide
Headache on the Hill is about more than just presenting evidence and making requests. If that were the case, there is a pretty good chance that, before long, legislators would be looking at their watches, checking their smartphones, and flashing knowing glances at their aides in an effort to cut things short. However, humanizing the topic by sharing stories of the toll migraine and cluster headaches take on individuals is compelling testimony that hopefully will lead to meaningful action and positive outcomes. Here is a sampling of the stories told during and after the Headache on the Hill session:
- Rachel Koh and Ronetta Stokes: Koh registered for both the 2019 and 2020 Headache on the Hill sessions, only to be forced to cancel due to migraine attacks. But this year, according to the American Migraine Foundation, she was able to participate virtually and tell her representatives why increased funding was important for her, as well as veterans, including her father and uncle. Meanwhile, Stokes, a first-time participant, said she was struck by the conversations she had with legislators. Most knew someone with migraine, and some were sufferers themselves. “The more we share and spread the word, the sooner we can end the stigma,” Stokes told the American Migraine Foundation.
- Mia Maysack: Maysack wrote about her experience in a column for Pain News Network. “I live with both migraine disease and cluster headaches, which are called ‘suicide headaches’ for good reason,” she wrote. “There’s no limit to the chaos, interruption, inconvenience, and discomfort these conditions have caused in my life, requiring my full-time attention just to manage the symptoms. The difficult experiences I and countless others have faced in seeking, finding, and attempting different forms of treatment is why I continue to advocate—even when I don't feel up to it.” Maysack added that although it is relatively easy for her to receive a medication prescription for her condition, she’d like to see more consideration given to treatments such as water therapy, massage, oxygen, and mindful meditation.
- Chloe Vruno: Vruno, a 21-year-old college student, has suffered with migraine since the age of 15. “Some days are worse than others,” she noted in an article in her local newspaper, the Steuben County, IN Herald Republican. “Most days I have to push through a migraine to make it to class, but some days are so severe that I cannot make it to classes. On days I cannot make it, I use my accommodation for attendance flexibility, or now with COVID, I Zoom into class from my room.” Vruno wanted to make her representatives aware of these types of disruptions, a regular occurrence for migraine sufferers like her. This was her second Headache on the Hill event, and she found lawmakers whom she spoke with to be “extremely attentive, engaged, and excited.”
“A moral imperative”
Stories like these from regular individuals across the United States who suffer from headache disorders go a long way in convincing legislators to act. It also helps to tap into a celebrity’s endorsement when you can. Headache on the Hill did not disappoint in this regard, with Jon Stewart, the former host of The Daily Show, appearing as a special guest during a policy panel discussion on chronic headache disorders and toxic exposure. The session, which took place virtually as part of Headache on the Hill, featured Stewart, a national advocate for service personnel with toxic exposures, and Rep. Mark Takano (D-CA), who delivered the keynote address. The panel discussion included first responders, veterans, and clinicians.
Stewart summed up the sentiments of all Headache on the Hill stakeholders this way: “This is an eminently solvable problem, but the urgency is now. People will continue to suffer needlessly if we don’t get this done. It is a moral imperative that we pass a bill on presumption as soon as possible.”
I always enjoy going to Washington on cold days in February to be part of Headache on the Hill, and I hope we will be back in-person next year. We have tripled the number of attendees over the last 13 years and have a higher percentage of great patients and advocates now. I have to give a special thanks to Dr. Bob Shapiro, Professor of Neurology at the University of Vermont, who started and has guided this phenomenal effort over the years, to Dr. Chris Gottschalk, Professor of Neurology at Yale, who is gradually taking over the reins, and to Katie MacDonald who runs the entire show, even though she suffers from chronic migraine on a daily basis.
1. Global Health Data Exchange. Global Burden of Disease Study 2019 (GBD 2019) Data Resources. http://ghdx.healthdata.org/gbd-2019. Accessed April 12, 2021.
2.Burish MJ, Pearson SM, RE Shapiro, et al. Cluster headache is one of the most intensely painful human conditions: Results from the International Cluster Headache Questionnaire. Headache. 2021;61:117-124.
3. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71:1821-1828.
4. Lipton RB, Buse DB, Dodick DW, et al. Burden of increasing opioid use in the treatment of migraine: Results from the Migraine in America Symptoms and Treatment Study. Headache. 2020;61:103-116.
5. Friedman BW, West J, Vinson DR, et al. Current management of migraine in US emergency departments: An analysis of the National Hospital Ambulatory Medical Care Survey. Cephalalgia. 2015;35:301-309.
6. Shapiro RE. What will it take to move the needle for headache disorders? An advocacy perspective. Headache. 2020;60:2059-2077.
7. NIH RePORT. Report on NIH funding vs. global burden of disease. https://report.nih.gov/report-nih-funding-vs-global-burden-disease. Accessed April 12, 2021.
8. NIH RePORT. Estimates of funding for various research, condition, and disease categories (RCDC). https://report.nih.gov/funding/categorical-spending#/. Published February 24, 2020. Accessed April 12, 2021.
9. National Institutes of Health. Funded projects. https://heal.nih.gov/funding/awarded. Updated March 18, 2020. Accessed April 12, 2021.
10. Couch JR, Stewart KE. Headache prevalence at 4-11 years after deployment-related traumatic brain injury in veterans of Iraq and Afghanistan wars and comparison to controls: A matched case-controlled study. Headache 2016;56:1004-1021.
11. Dr. Richard A. Stone, Acting Under Secretary for Health. Message to Staff-Airborne Hazards and Open Burn Pit Registry. https://players.brightcove.net/2851863979001/default_default/index.html?videoId=6228317154001. Published February 2021. Accessed April 12, 2021.
12. US Department of Veterans Affairs. Report on Data from the Airborne Hazards and Open Burn Pit (AH&OBP) Registry. https://www.publichealth.va.gov/docs/exposures/va-ahobp-registry-data-report-june2015.pdf#. Published June 2015. Accessed April 12, 2021.
13. US Government Publishing Office. Military construction, Veterans Affairs, and related agencies appropriation bill, 2018. https://www.appropriations.senate.gov/imo/media/doc/FY2018%20MiliCon-VA%20Bill%20S1557.pdf. Published July 13, 2017. Accessed April 12, 2021.
14. Fenton BT, Lindsey H, Grinberg AS, et al. Presentation given at: 62nd Annual Scientific Meeting American Headache Society- Prevalence of Headache and Comorbidities Among Men and Women Veterans Across the Veterans Health Administration – a 10‐year Cohort Study. VA Connecticut Healthcare System, West Haven, CT; Yale School of Medicine, West Haven, CT; 3Yeshiva University, Bronx, NY. https://headachejournal.onlinelibrary.wiley.com/doi/full/10.1111/head.13854. Published June 13, 2020. Accessed April 12, 2021.
1. Global Health Data Exchange. Global Burden of Disease Study 2019 (GBD 2019) Data Resources. http://ghdx.healthdata.org/gbd-2019. Accessed April 12, 2021.
2.Burish MJ, Pearson SM, RE Shapiro, et al. Cluster headache is one of the most intensely painful human conditions: Results from the International Cluster Headache Questionnaire. Headache. 2021;61:117-124.
3. Bigal ME, Lipton RB. Excessive acute migraine medication use and migraine progression. Neurology. 2008;71:1821-1828.
4. Lipton RB, Buse DB, Dodick DW, et al. Burden of increasing opioid use in the treatment of migraine: Results from the Migraine in America Symptoms and Treatment Study. Headache. 2020;61:103-116.
5. Friedman BW, West J, Vinson DR, et al. Current management of migraine in US emergency departments: An analysis of the National Hospital Ambulatory Medical Care Survey. Cephalalgia. 2015;35:301-309.
6. Shapiro RE. What will it take to move the needle for headache disorders? An advocacy perspective. Headache. 2020;60:2059-2077.
7. NIH RePORT. Report on NIH funding vs. global burden of disease. https://report.nih.gov/report-nih-funding-vs-global-burden-disease. Accessed April 12, 2021.
8. NIH RePORT. Estimates of funding for various research, condition, and disease categories (RCDC). https://report.nih.gov/funding/categorical-spending#/. Published February 24, 2020. Accessed April 12, 2021.
9. National Institutes of Health. Funded projects. https://heal.nih.gov/funding/awarded. Updated March 18, 2020. Accessed April 12, 2021.
10. Couch JR, Stewart KE. Headache prevalence at 4-11 years after deployment-related traumatic brain injury in veterans of Iraq and Afghanistan wars and comparison to controls: A matched case-controlled study. Headache 2016;56:1004-1021.
11. Dr. Richard A. Stone, Acting Under Secretary for Health. Message to Staff-Airborne Hazards and Open Burn Pit Registry. https://players.brightcove.net/2851863979001/default_default/index.html?videoId=6228317154001. Published February 2021. Accessed April 12, 2021.
12. US Department of Veterans Affairs. Report on Data from the Airborne Hazards and Open Burn Pit (AH&OBP) Registry. https://www.publichealth.va.gov/docs/exposures/va-ahobp-registry-data-report-june2015.pdf#. Published June 2015. Accessed April 12, 2021.
13. US Government Publishing Office. Military construction, Veterans Affairs, and related agencies appropriation bill, 2018. https://www.appropriations.senate.gov/imo/media/doc/FY2018%20MiliCon-VA%20Bill%20S1557.pdf. Published July 13, 2017. Accessed April 12, 2021.
14. Fenton BT, Lindsey H, Grinberg AS, et al. Presentation given at: 62nd Annual Scientific Meeting American Headache Society- Prevalence of Headache and Comorbidities Among Men and Women Veterans Across the Veterans Health Administration – a 10‐year Cohort Study. VA Connecticut Healthcare System, West Haven, CT; Yale School of Medicine, West Haven, CT; 3Yeshiva University, Bronx, NY. https://headachejournal.onlinelibrary.wiley.com/doi/full/10.1111/head.13854. Published June 13, 2020. Accessed April 12, 2021.
Delayed Coronary Vasospasm in a Patient with Metastatic Gastric Cancer Receiving FOLFOX Therapy
A 40-year-old man with stage IV gastric adenocarcinoma was found to have coronary artery vasospasm in the setting of recent 5-fluorouracil administration.
Coronary artery vasospasm is a rare but well-known adverse effect of 5-fluorouracil (5-FU) that can be life threatening if unrecognized. Patients typically present with anginal chest pain and ST elevations on electrocardiogram (ECG) without atherosclerotic disease on coronary angiography. This phenomenon typically occurs during or shortly after infusion and resolves within hours to days after cessation of 5-FU.
In this report, we present an unusual case of coronary artery vasospasm that intermittently recurred for 25 days following 5-FU treatment in a 40-year-old male with stage IV gastric adenocarcinoma. We also review the literature on typical presentation and risk factors for 5-FU-induced coronary vasospasm, findings on coronary angiography, and management options.
5-FU is an IV administered antimetabolite chemotherapy commonly used to treat solid tumors, including gastrointestinal, pancreatic, breast, and head and neck tumors. 5-FU inhibits thymidylate synthase, which reduces levels of thymidine, a key pyrimidine nucleoside required for DNA replication within tumor cells.1 For several decades, 5-FU has remained one of the first-line drugs for colorectal cancer because it may be curative. It is the third most commonly used chemotherapy in the world and is included on the World Health Organization’s list of essential medicines.2
Cardiotoxicity occurs in 1.2 to 18% of patients who receive 5-FU therapy.3 Although there is variability in presentation for acute cardiotoxicity from 5-FU, including sudden death, angina pectoris, myocardial infarction, and ventricular arrhythmias, the mechanism most commonly implicated is coronary artery vasospasm.3 The direct observation of active coronary artery vasospasm during left heart catheterization is rare due its transient nature; however, several case studies have managed to demonstrate this.4,5 The pathophysiology of 5-FU-induced cardiotoxicity is unknown, but adverse effects on cardiac microvasculature, myocyte metabolism, platelet aggregation, and coronary vasoconstriction have all been proposed.3,6In the current case, we present a patient with stage IV gastric adenocarcinoma who complained of chest pain during hospitalization and was found to have coronary artery vasospasm in the setting of recent 5-FU administration. Following coronary angiography that showed a lack of atherosclerotic disease, the patient continued to experience episodes of chest pain with ST elevations on ECG that recurred despite cessation of 5-FU and repeated administration of vasodilatory medications.
Case Presentation
A male aged 40 years was admitted to the hospital for abdominal pain, with initial imaging concerning for partial small bowel obstruction. His history included recently diagnosed stage IV gastric adenocarcinoma complicated by peritoneal carcinomatosis status post initiation of infusional FOLFOX-4 (5-FU, leucovorin, and oxaliplatin) 11 days prior. The patient was treated for small bowel obstruction. However, several days after admission, he developed nonpleuritic, substernal chest pain unrelated to exertion and unrelieved by rest. The patient reported no known risk factors, family history, or personal history of coronary artery disease. Baseline echocardiography and ECG performed several months prior showed normal left ventricular function without ischemic findings.
Physical examination at the time of chest pain revealed a heart rate of 140 beats/min. The remainder of his vital signs were within normal range. There were no murmurs, rubs, gallops, or additional heart sounds heard on cardiac auscultation. Chest pain was not reproducible to palpation or positional in nature. An ECG demonstrated dynamic inferolateral ST elevations with reciprocal changes in leads I and aVL (Figure 1). A bedside echocardiogram showed hypokinesis of the septal wall. Troponin-I returned below the detectable level.
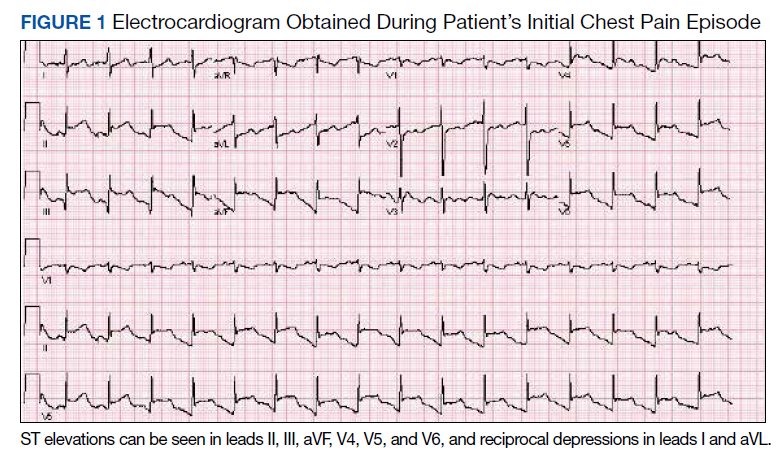
The patient was taken for emergent coronary catheterization, which demonstrated patent epicardial coronary arteries without atherosclerosis, a left ventricular ejection fraction of 60%, and a right dominant heart (Figures 2 and 3). Ventriculogram showed normal wall motion. Repeat troponin-I several hours after catheterization was again below detectable levels.
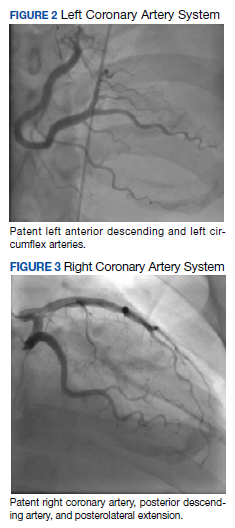
Given the patient’s acute onset of chest pain and inferolateral ST elevations seen on ECG, the working diagnosis prior to coronary catherization was acute coronary syndrome. The differential diagnosis included other causes of life-threatening chest pain, including pulmonary embolism, pneumonia, aortic dissection, myopericarditis, pericardial effusion, cardiac tamponade, or coronary artery vasospasm. Computed tomography (CT) angiography of the chest was not consistent with pulmonary embolism or other acute cardiopulmonary process. Based on findings from coronary angiography and recent exposure to 5-FU, as well as resolution followed by recurrence of chest pain and ECG changes over weeks, the most likely diagnosis after coronary catheterization was coronary artery vasospasm.
Treatment
Following catheterization, the patient returned to the medical intensive care unit, where he continued to report intermittent episodes of chest pain with ST elevations. In the following days, he was started on isosorbide mononitrate 150 mg daily and amlodipine 10 mg daily. Although these vasodilatory agents reduced the frequency of his chest pain episodes, intermittent chest pain associated with ST elevations on ECG continued even with maximal doses of isosorbide mononitrate and amlodipine. Administration of sublingual nitroglycerin during chest pain episodes effectively relieved his chest pain. Given the severity and frequency of the patient’s chest pain, the oncology consult team recommended foregoing further chemotherapeutic treatment with 5-FU.
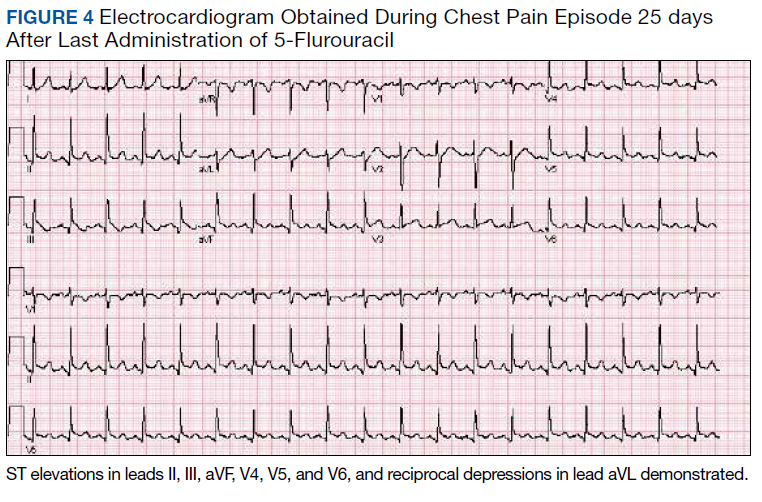
Outcome
Despite holding 5-FU throughout the patient’s hospitalization and treating the patient with antianginal mediations, frequent chest pain episodes associated with ST elevations continued to recur until 25 days after his last treatment with 5-FU (Figure 4). The patient eventually expired during this hospital stay due to cancer-related complications.
Discussion
Coronary artery vasospasm is a well-known complication of 5-FU that can be life threatening if unrecognized.6-8 As seen in our case, patients typically present with anginal chest pain relieved with nitrates and ST elevations on ECG in the absence of occlusive macrovascular disease on coronary angiography.
A unique aspect of 5-FU is its variability in dose and frequency of administration across chemotherapeutic regimens. Particularly, 5-FU can be administered in daily intravenous bolus doses or as a continuous infusion for a protracted length of time. The spectrum of toxicity from 5-FU differs depending on the dose and frequency of administration. Bolus administration of 5-FU, for example, is thought to be associated with a higher rate of myelosuppression, while infusional administration of 5-FU is thought to be associated with a higher rate of cardiotoxicity and a higher tumor response rate.9
Most cases of coronary vasospasm occur either during infusion of 5-FU or within hours to days after completion. The median time of presentation for 5-FU-induced coronary artery vasospasm is about 12 hours postinfusion, while the most delayed presentation reported in the literature is 72 hours postinfusion.6,8 Delayed presentation of vasospasm may result from the release of potent vasoactive metabolites of 5-FU that accumulate over time; therefore, infusional administration may accentuate this effect.6,9 Remarkably, our patient’s chest pain episodes persisted for 25 days despite treatment with anti-anginal medications, highlighting the extent to which infusional 5-FU can produce a delay in adverse cardiotoxic effects and the importance of ongoing clinical vigilance after 5-FU exposure.
Vasospasm alone does not completely explain the spectrum of cardiac toxicity attributed to 5-FU administration. As in our case, coronary angiography during symptomatic episodes often fails to demonstrate coronary vasospasm.8 Additionally, ergonovine, an alkaloid agent used to assess coronary vasomotor function, failed to induce coronary vasospasm in some patients with suspected 5-FU-induced cardiac toxicity.10 The lack of vasospasm in some patients with 5-FU-induced cardiac toxicity suggests multiple independent effects of 5-FU on cardiac tissue that are poorly understood.
In the absence of obvious macrovascular effects, there also may be a deleterious effect of 5-FU on the coronary microvasculature that may result in coronary artery vasospasm. Though coronary microvasculature cannot be directly visualized, observation of slowed coronary blood velocity indicates a reduction in microvascular flow.8 Thus, the failure to observe epicardial coronary vasospasm in our patient does not preclude a vasospastic pathology.
The heterogeneous presentation of coronary artery vasospasm demands consideration of other disease processes such as atherosclerotic coronary artery disease, pericarditis, myopericarditis, primary arrythmias, and stress-induced cardiomyopathy, all of which have been described in association with 5-FU administration.8 A 12-lead ECG should be performed during a suspected attack. An ECG will typically demonstrate ST elevations corresponding to spasm of the involved vessel. Reciprocal ST depressions in the contralateral leads also may be seen. ECG may be useful in the acute setting to identify regional wall motion abnormalities or to rule out pericardial effusion as a cause. Cardiac biomarkers such as troponin-I, -C, and creatine kinase typically are less useful because they are often normal, even in known coronary artery vasospasm.11
Coronary angiography during an episode may show a localized region of vasospasm in an epicardial artery. Diffuse multivessel vasospasm does occur, and the location of vasospasm may change, but these events are rare. Under normal circumstances, provocative testing involving angiography with administration of acetylcholine, ergot agents, or hyperventilation can be performed. However, this type of investigation should be limited to specialized centers and should not be performed in the acute phase of the disease.12
Treatment of suspected coronary vasospasm in patients receiving 5-FU involves stopping the infusion and administering calcium channel blockers or oral nitrates to relieve anginal symptoms.13 5-FU-induced coronary artery vasospasm has a 90% rate of recurrence with subsequent infusions.8 If possible, alternate chemotherapy regimens should be considered once coronary artery vasospasm has been identified.14,15 If further 5-FU use is required, or if benefits are deemed to outweigh risks, infusions should be given in an inpatient setting with continuous cardiac monitoring.16
Calcium channel blockers and oral nitrates have been found to produce benefit in patients in acute settings; however, there is little evidence to attest to their effectiveness as prophylactic agents in those receiving 5-FU. Some reports demonstrate episodes where both calcium channel blockers and oral nitrates failed to prevent subsequent vasospasms.17 Although this was the case for our patient, short-acting sublingual nitroglycerin seemed to be effective in reducing the frequency of anginal symptoms.
Long-term outcomes have not been well investigated for patients with 5-FU-induced coronary vasospasm. However, many case reports show improvements in left ventricular function between 8 and 15 days after discontinuation of 5-FU.7,10 Although this would be a valuable topic for further research, the rarity of this phenomenon creates limitations.
Conclusions
5-FU is a first-line chemotherapy for gastrointestinal cancers that is generally well tolerated but may be associated with potentially life-threatening cardiotoxic effects, of which coronary artery vasospasm is the most common. Coronary artery vasospasm presents with anginal chest pain and ST elevations on ECG that can be indistinguishable from acute coronary syndrome. Diagnosis requires cardiac catheterization, which will reveal patent coronary arteries. Infusional administration of 5-FU may be more likely to produce late cardiotoxic effects and a longer period of persistent symptoms, necessitating close monitoring for days or even weeks from last administration of 5-FU. Coronary artery vasospasm should be treated with anti-anginal medications, though varying degrees of effectiveness can be seen; clinicians should remain vigilant for recurrent episodes of chest pain despite treatment.
1. Wacker A, Lersch C, Scherpinski U, Reindl L, Seyfarth M. High incidence of angina pectoris in patients treated with 5-fluorouracil. A planned surveillance study with 102 patients. Oncology. 2003;65(2):108-112. doi:10.1159/000072334
2. World Health Organization Model List of Essential Medicines, 21st List, 2019. Accessed April 14, 2021. https://apps.who.int/iris/rest/bitstreams/1237479/retrieve
3. Jensen SA, Sørensen JB. Risk factors and prevention of cardiotoxicity induced by 5-fluorouracil or capecitabine. Cancer Chemother Pharmacol. 2006;58(4):487-493. doi:10.1007/s00280-005-0178-1
4. Shoemaker LK, Arora U, Rocha Lima CM. 5-fluorouracil-induced coronary vasospasm. Cancer Control. 2004;11(1):46-49. doi:10.1177/107327480401100207
5. Luwaert RJ, Descamps O, Majois F, Chaudron JM, Beauduin M. Coronary artery spasm induced by 5-fluorouracil. Eur Heart J. 1991;12(3):468-470. doi:10.1093/oxfordjournals.eurheartj.a059919
6. Saif MW, Shah MM, Shah AR. Fluoropyrimidine-associated cardiotoxicity: revisited. Expert Opin Drug Saf. 2009;8(2):191-202. doi:10.1517/14740330902733961
7. Patel B, Kloner RA, Ensley J, Al-Sarraf M, Kish J, Wynne J. 5-Fluorouracil cardiotoxicity: left ventricular dysfunction and effect of coronary vasodilators. Am J Med Sci. 1987;294(4):238-243. doi:10.1097/00000441-198710000-00004
8. Sara JD, Kaur J, Khodadadi R, et al. 5-fluorouracil and cardiotoxicity: a review. Ther Adv Med Oncol. 2018;10:1758835918780140. Published 2018 Jun 18. doi:10.1177/1758835918780140
9. Hansen RM, Ryan L, Anderson T, et al. Phase III study of bolus versus infusion fluorouracil with or without cisplatin in advanced colorectal cancer. J Natl Cancer Inst. 1996;88(10):668-674. doi:10.1093/jnci/88.10.668
10. Kim SM, Kwak CH, Lee B, et al. A case of severe coronary spasm associated with 5-fluorouracil chemotherapy. Korean J Intern Med. 2012;27(3):342-345. doi:10.3904/kjim.2012.27.3.342
11. Swarup S, Patibandla S, Grossman SA. Coronary Artery Vasospasm. StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2021.
12. Beijk MA, Vlastra WV, Delewi R, et al. Myocardial infarction with non-obstructive coronary arteries: a focus on vasospastic angina. Neth Heart J. 2019;27(5):237-245. doi:10.1007/s12471-019-1232-7
13. Giza DE, Boccalandro F, Lopez-Mattei J, et al. Ischemic heart disease: special considerations in cardio-oncology. Curr Treat Options Cardiovasc Med. 2017;19(5):37. doi:10.1007/s11936-017-0535-5
14. Meydan N, Kundak I, Yavuzsen T, et al. Cardiotoxicity of de Gramont’s regimen: incidence, clinical characteristics and long-term follow-up. Jpn J Clin Oncol. 2005;35(5):265-270. doi:10.1093/jjco/hyi071
15. Senkus E, Jassem J. Cardiovascular effects of systemic cancer treatment. Cancer Treat Rev. 2011;37(4):300-311. doi:10.1016/j.ctrv.2010.11.001
16. Rezkalla S, Kloner RA, Ensley J, et al. Continuous ambulatory ECG monitoring during fluorouracil therapy: a prospective study. J Clin Oncol. 1989;7(4):509-514. doi:10.1200/JCO.1989.7.4.509
17. Akpek G, Hartshorn KL. Failure of oral nitrate and calcium channel blocker therapy to prevent 5-fluorouracil-related myocardial ischemia: a case report. Cancer Chemother Pharmacol. 1999;43(2):157-161. doi:10.1007/s002800050877
A 40-year-old man with stage IV gastric adenocarcinoma was found to have coronary artery vasospasm in the setting of recent 5-fluorouracil administration.
A 40-year-old man with stage IV gastric adenocarcinoma was found to have coronary artery vasospasm in the setting of recent 5-fluorouracil administration.
Coronary artery vasospasm is a rare but well-known adverse effect of 5-fluorouracil (5-FU) that can be life threatening if unrecognized. Patients typically present with anginal chest pain and ST elevations on electrocardiogram (ECG) without atherosclerotic disease on coronary angiography. This phenomenon typically occurs during or shortly after infusion and resolves within hours to days after cessation of 5-FU.
In this report, we present an unusual case of coronary artery vasospasm that intermittently recurred for 25 days following 5-FU treatment in a 40-year-old male with stage IV gastric adenocarcinoma. We also review the literature on typical presentation and risk factors for 5-FU-induced coronary vasospasm, findings on coronary angiography, and management options.
5-FU is an IV administered antimetabolite chemotherapy commonly used to treat solid tumors, including gastrointestinal, pancreatic, breast, and head and neck tumors. 5-FU inhibits thymidylate synthase, which reduces levels of thymidine, a key pyrimidine nucleoside required for DNA replication within tumor cells.1 For several decades, 5-FU has remained one of the first-line drugs for colorectal cancer because it may be curative. It is the third most commonly used chemotherapy in the world and is included on the World Health Organization’s list of essential medicines.2
Cardiotoxicity occurs in 1.2 to 18% of patients who receive 5-FU therapy.3 Although there is variability in presentation for acute cardiotoxicity from 5-FU, including sudden death, angina pectoris, myocardial infarction, and ventricular arrhythmias, the mechanism most commonly implicated is coronary artery vasospasm.3 The direct observation of active coronary artery vasospasm during left heart catheterization is rare due its transient nature; however, several case studies have managed to demonstrate this.4,5 The pathophysiology of 5-FU-induced cardiotoxicity is unknown, but adverse effects on cardiac microvasculature, myocyte metabolism, platelet aggregation, and coronary vasoconstriction have all been proposed.3,6In the current case, we present a patient with stage IV gastric adenocarcinoma who complained of chest pain during hospitalization and was found to have coronary artery vasospasm in the setting of recent 5-FU administration. Following coronary angiography that showed a lack of atherosclerotic disease, the patient continued to experience episodes of chest pain with ST elevations on ECG that recurred despite cessation of 5-FU and repeated administration of vasodilatory medications.
Case Presentation
A male aged 40 years was admitted to the hospital for abdominal pain, with initial imaging concerning for partial small bowel obstruction. His history included recently diagnosed stage IV gastric adenocarcinoma complicated by peritoneal carcinomatosis status post initiation of infusional FOLFOX-4 (5-FU, leucovorin, and oxaliplatin) 11 days prior. The patient was treated for small bowel obstruction. However, several days after admission, he developed nonpleuritic, substernal chest pain unrelated to exertion and unrelieved by rest. The patient reported no known risk factors, family history, or personal history of coronary artery disease. Baseline echocardiography and ECG performed several months prior showed normal left ventricular function without ischemic findings.
Physical examination at the time of chest pain revealed a heart rate of 140 beats/min. The remainder of his vital signs were within normal range. There were no murmurs, rubs, gallops, or additional heart sounds heard on cardiac auscultation. Chest pain was not reproducible to palpation or positional in nature. An ECG demonstrated dynamic inferolateral ST elevations with reciprocal changes in leads I and aVL (Figure 1). A bedside echocardiogram showed hypokinesis of the septal wall. Troponin-I returned below the detectable level.
The patient was taken for emergent coronary catheterization, which demonstrated patent epicardial coronary arteries without atherosclerosis, a left ventricular ejection fraction of 60%, and a right dominant heart (Figures 2 and 3). Ventriculogram showed normal wall motion. Repeat troponin-I several hours after catheterization was again below detectable levels.
Given the patient’s acute onset of chest pain and inferolateral ST elevations seen on ECG, the working diagnosis prior to coronary catherization was acute coronary syndrome. The differential diagnosis included other causes of life-threatening chest pain, including pulmonary embolism, pneumonia, aortic dissection, myopericarditis, pericardial effusion, cardiac tamponade, or coronary artery vasospasm. Computed tomography (CT) angiography of the chest was not consistent with pulmonary embolism or other acute cardiopulmonary process. Based on findings from coronary angiography and recent exposure to 5-FU, as well as resolution followed by recurrence of chest pain and ECG changes over weeks, the most likely diagnosis after coronary catheterization was coronary artery vasospasm.
Treatment
Following catheterization, the patient returned to the medical intensive care unit, where he continued to report intermittent episodes of chest pain with ST elevations. In the following days, he was started on isosorbide mononitrate 150 mg daily and amlodipine 10 mg daily. Although these vasodilatory agents reduced the frequency of his chest pain episodes, intermittent chest pain associated with ST elevations on ECG continued even with maximal doses of isosorbide mononitrate and amlodipine. Administration of sublingual nitroglycerin during chest pain episodes effectively relieved his chest pain. Given the severity and frequency of the patient’s chest pain, the oncology consult team recommended foregoing further chemotherapeutic treatment with 5-FU.
Outcome
Despite holding 5-FU throughout the patient’s hospitalization and treating the patient with antianginal mediations, frequent chest pain episodes associated with ST elevations continued to recur until 25 days after his last treatment with 5-FU (Figure 4). The patient eventually expired during this hospital stay due to cancer-related complications.
Discussion
Coronary artery vasospasm is a well-known complication of 5-FU that can be life threatening if unrecognized.6-8 As seen in our case, patients typically present with anginal chest pain relieved with nitrates and ST elevations on ECG in the absence of occlusive macrovascular disease on coronary angiography.
A unique aspect of 5-FU is its variability in dose and frequency of administration across chemotherapeutic regimens. Particularly, 5-FU can be administered in daily intravenous bolus doses or as a continuous infusion for a protracted length of time. The spectrum of toxicity from 5-FU differs depending on the dose and frequency of administration. Bolus administration of 5-FU, for example, is thought to be associated with a higher rate of myelosuppression, while infusional administration of 5-FU is thought to be associated with a higher rate of cardiotoxicity and a higher tumor response rate.9
Most cases of coronary vasospasm occur either during infusion of 5-FU or within hours to days after completion. The median time of presentation for 5-FU-induced coronary artery vasospasm is about 12 hours postinfusion, while the most delayed presentation reported in the literature is 72 hours postinfusion.6,8 Delayed presentation of vasospasm may result from the release of potent vasoactive metabolites of 5-FU that accumulate over time; therefore, infusional administration may accentuate this effect.6,9 Remarkably, our patient’s chest pain episodes persisted for 25 days despite treatment with anti-anginal medications, highlighting the extent to which infusional 5-FU can produce a delay in adverse cardiotoxic effects and the importance of ongoing clinical vigilance after 5-FU exposure.
Vasospasm alone does not completely explain the spectrum of cardiac toxicity attributed to 5-FU administration. As in our case, coronary angiography during symptomatic episodes often fails to demonstrate coronary vasospasm.8 Additionally, ergonovine, an alkaloid agent used to assess coronary vasomotor function, failed to induce coronary vasospasm in some patients with suspected 5-FU-induced cardiac toxicity.10 The lack of vasospasm in some patients with 5-FU-induced cardiac toxicity suggests multiple independent effects of 5-FU on cardiac tissue that are poorly understood.
In the absence of obvious macrovascular effects, there also may be a deleterious effect of 5-FU on the coronary microvasculature that may result in coronary artery vasospasm. Though coronary microvasculature cannot be directly visualized, observation of slowed coronary blood velocity indicates a reduction in microvascular flow.8 Thus, the failure to observe epicardial coronary vasospasm in our patient does not preclude a vasospastic pathology.
The heterogeneous presentation of coronary artery vasospasm demands consideration of other disease processes such as atherosclerotic coronary artery disease, pericarditis, myopericarditis, primary arrythmias, and stress-induced cardiomyopathy, all of which have been described in association with 5-FU administration.8 A 12-lead ECG should be performed during a suspected attack. An ECG will typically demonstrate ST elevations corresponding to spasm of the involved vessel. Reciprocal ST depressions in the contralateral leads also may be seen. ECG may be useful in the acute setting to identify regional wall motion abnormalities or to rule out pericardial effusion as a cause. Cardiac biomarkers such as troponin-I, -C, and creatine kinase typically are less useful because they are often normal, even in known coronary artery vasospasm.11
Coronary angiography during an episode may show a localized region of vasospasm in an epicardial artery. Diffuse multivessel vasospasm does occur, and the location of vasospasm may change, but these events are rare. Under normal circumstances, provocative testing involving angiography with administration of acetylcholine, ergot agents, or hyperventilation can be performed. However, this type of investigation should be limited to specialized centers and should not be performed in the acute phase of the disease.12
Treatment of suspected coronary vasospasm in patients receiving 5-FU involves stopping the infusion and administering calcium channel blockers or oral nitrates to relieve anginal symptoms.13 5-FU-induced coronary artery vasospasm has a 90% rate of recurrence with subsequent infusions.8 If possible, alternate chemotherapy regimens should be considered once coronary artery vasospasm has been identified.14,15 If further 5-FU use is required, or if benefits are deemed to outweigh risks, infusions should be given in an inpatient setting with continuous cardiac monitoring.16
Calcium channel blockers and oral nitrates have been found to produce benefit in patients in acute settings; however, there is little evidence to attest to their effectiveness as prophylactic agents in those receiving 5-FU. Some reports demonstrate episodes where both calcium channel blockers and oral nitrates failed to prevent subsequent vasospasms.17 Although this was the case for our patient, short-acting sublingual nitroglycerin seemed to be effective in reducing the frequency of anginal symptoms.
Long-term outcomes have not been well investigated for patients with 5-FU-induced coronary vasospasm. However, many case reports show improvements in left ventricular function between 8 and 15 days after discontinuation of 5-FU.7,10 Although this would be a valuable topic for further research, the rarity of this phenomenon creates limitations.
Conclusions
5-FU is a first-line chemotherapy for gastrointestinal cancers that is generally well tolerated but may be associated with potentially life-threatening cardiotoxic effects, of which coronary artery vasospasm is the most common. Coronary artery vasospasm presents with anginal chest pain and ST elevations on ECG that can be indistinguishable from acute coronary syndrome. Diagnosis requires cardiac catheterization, which will reveal patent coronary arteries. Infusional administration of 5-FU may be more likely to produce late cardiotoxic effects and a longer period of persistent symptoms, necessitating close monitoring for days or even weeks from last administration of 5-FU. Coronary artery vasospasm should be treated with anti-anginal medications, though varying degrees of effectiveness can be seen; clinicians should remain vigilant for recurrent episodes of chest pain despite treatment.
Coronary artery vasospasm is a rare but well-known adverse effect of 5-fluorouracil (5-FU) that can be life threatening if unrecognized. Patients typically present with anginal chest pain and ST elevations on electrocardiogram (ECG) without atherosclerotic disease on coronary angiography. This phenomenon typically occurs during or shortly after infusion and resolves within hours to days after cessation of 5-FU.
In this report, we present an unusual case of coronary artery vasospasm that intermittently recurred for 25 days following 5-FU treatment in a 40-year-old male with stage IV gastric adenocarcinoma. We also review the literature on typical presentation and risk factors for 5-FU-induced coronary vasospasm, findings on coronary angiography, and management options.
5-FU is an IV administered antimetabolite chemotherapy commonly used to treat solid tumors, including gastrointestinal, pancreatic, breast, and head and neck tumors. 5-FU inhibits thymidylate synthase, which reduces levels of thymidine, a key pyrimidine nucleoside required for DNA replication within tumor cells.1 For several decades, 5-FU has remained one of the first-line drugs for colorectal cancer because it may be curative. It is the third most commonly used chemotherapy in the world and is included on the World Health Organization’s list of essential medicines.2
Cardiotoxicity occurs in 1.2 to 18% of patients who receive 5-FU therapy.3 Although there is variability in presentation for acute cardiotoxicity from 5-FU, including sudden death, angina pectoris, myocardial infarction, and ventricular arrhythmias, the mechanism most commonly implicated is coronary artery vasospasm.3 The direct observation of active coronary artery vasospasm during left heart catheterization is rare due its transient nature; however, several case studies have managed to demonstrate this.4,5 The pathophysiology of 5-FU-induced cardiotoxicity is unknown, but adverse effects on cardiac microvasculature, myocyte metabolism, platelet aggregation, and coronary vasoconstriction have all been proposed.3,6In the current case, we present a patient with stage IV gastric adenocarcinoma who complained of chest pain during hospitalization and was found to have coronary artery vasospasm in the setting of recent 5-FU administration. Following coronary angiography that showed a lack of atherosclerotic disease, the patient continued to experience episodes of chest pain with ST elevations on ECG that recurred despite cessation of 5-FU and repeated administration of vasodilatory medications.
Case Presentation
A male aged 40 years was admitted to the hospital for abdominal pain, with initial imaging concerning for partial small bowel obstruction. His history included recently diagnosed stage IV gastric adenocarcinoma complicated by peritoneal carcinomatosis status post initiation of infusional FOLFOX-4 (5-FU, leucovorin, and oxaliplatin) 11 days prior. The patient was treated for small bowel obstruction. However, several days after admission, he developed nonpleuritic, substernal chest pain unrelated to exertion and unrelieved by rest. The patient reported no known risk factors, family history, or personal history of coronary artery disease. Baseline echocardiography and ECG performed several months prior showed normal left ventricular function without ischemic findings.
Physical examination at the time of chest pain revealed a heart rate of 140 beats/min. The remainder of his vital signs were within normal range. There were no murmurs, rubs, gallops, or additional heart sounds heard on cardiac auscultation. Chest pain was not reproducible to palpation or positional in nature. An ECG demonstrated dynamic inferolateral ST elevations with reciprocal changes in leads I and aVL (Figure 1). A bedside echocardiogram showed hypokinesis of the septal wall. Troponin-I returned below the detectable level.
The patient was taken for emergent coronary catheterization, which demonstrated patent epicardial coronary arteries without atherosclerosis, a left ventricular ejection fraction of 60%, and a right dominant heart (Figures 2 and 3). Ventriculogram showed normal wall motion. Repeat troponin-I several hours after catheterization was again below detectable levels.
Given the patient’s acute onset of chest pain and inferolateral ST elevations seen on ECG, the working diagnosis prior to coronary catherization was acute coronary syndrome. The differential diagnosis included other causes of life-threatening chest pain, including pulmonary embolism, pneumonia, aortic dissection, myopericarditis, pericardial effusion, cardiac tamponade, or coronary artery vasospasm. Computed tomography (CT) angiography of the chest was not consistent with pulmonary embolism or other acute cardiopulmonary process. Based on findings from coronary angiography and recent exposure to 5-FU, as well as resolution followed by recurrence of chest pain and ECG changes over weeks, the most likely diagnosis after coronary catheterization was coronary artery vasospasm.
Treatment
Following catheterization, the patient returned to the medical intensive care unit, where he continued to report intermittent episodes of chest pain with ST elevations. In the following days, he was started on isosorbide mononitrate 150 mg daily and amlodipine 10 mg daily. Although these vasodilatory agents reduced the frequency of his chest pain episodes, intermittent chest pain associated with ST elevations on ECG continued even with maximal doses of isosorbide mononitrate and amlodipine. Administration of sublingual nitroglycerin during chest pain episodes effectively relieved his chest pain. Given the severity and frequency of the patient’s chest pain, the oncology consult team recommended foregoing further chemotherapeutic treatment with 5-FU.
Outcome
Despite holding 5-FU throughout the patient’s hospitalization and treating the patient with antianginal mediations, frequent chest pain episodes associated with ST elevations continued to recur until 25 days after his last treatment with 5-FU (Figure 4). The patient eventually expired during this hospital stay due to cancer-related complications.
Discussion
Coronary artery vasospasm is a well-known complication of 5-FU that can be life threatening if unrecognized.6-8 As seen in our case, patients typically present with anginal chest pain relieved with nitrates and ST elevations on ECG in the absence of occlusive macrovascular disease on coronary angiography.
A unique aspect of 5-FU is its variability in dose and frequency of administration across chemotherapeutic regimens. Particularly, 5-FU can be administered in daily intravenous bolus doses or as a continuous infusion for a protracted length of time. The spectrum of toxicity from 5-FU differs depending on the dose and frequency of administration. Bolus administration of 5-FU, for example, is thought to be associated with a higher rate of myelosuppression, while infusional administration of 5-FU is thought to be associated with a higher rate of cardiotoxicity and a higher tumor response rate.9
Most cases of coronary vasospasm occur either during infusion of 5-FU or within hours to days after completion. The median time of presentation for 5-FU-induced coronary artery vasospasm is about 12 hours postinfusion, while the most delayed presentation reported in the literature is 72 hours postinfusion.6,8 Delayed presentation of vasospasm may result from the release of potent vasoactive metabolites of 5-FU that accumulate over time; therefore, infusional administration may accentuate this effect.6,9 Remarkably, our patient’s chest pain episodes persisted for 25 days despite treatment with anti-anginal medications, highlighting the extent to which infusional 5-FU can produce a delay in adverse cardiotoxic effects and the importance of ongoing clinical vigilance after 5-FU exposure.
Vasospasm alone does not completely explain the spectrum of cardiac toxicity attributed to 5-FU administration. As in our case, coronary angiography during symptomatic episodes often fails to demonstrate coronary vasospasm.8 Additionally, ergonovine, an alkaloid agent used to assess coronary vasomotor function, failed to induce coronary vasospasm in some patients with suspected 5-FU-induced cardiac toxicity.10 The lack of vasospasm in some patients with 5-FU-induced cardiac toxicity suggests multiple independent effects of 5-FU on cardiac tissue that are poorly understood.
In the absence of obvious macrovascular effects, there also may be a deleterious effect of 5-FU on the coronary microvasculature that may result in coronary artery vasospasm. Though coronary microvasculature cannot be directly visualized, observation of slowed coronary blood velocity indicates a reduction in microvascular flow.8 Thus, the failure to observe epicardial coronary vasospasm in our patient does not preclude a vasospastic pathology.
The heterogeneous presentation of coronary artery vasospasm demands consideration of other disease processes such as atherosclerotic coronary artery disease, pericarditis, myopericarditis, primary arrythmias, and stress-induced cardiomyopathy, all of which have been described in association with 5-FU administration.8 A 12-lead ECG should be performed during a suspected attack. An ECG will typically demonstrate ST elevations corresponding to spasm of the involved vessel. Reciprocal ST depressions in the contralateral leads also may be seen. ECG may be useful in the acute setting to identify regional wall motion abnormalities or to rule out pericardial effusion as a cause. Cardiac biomarkers such as troponin-I, -C, and creatine kinase typically are less useful because they are often normal, even in known coronary artery vasospasm.11
Coronary angiography during an episode may show a localized region of vasospasm in an epicardial artery. Diffuse multivessel vasospasm does occur, and the location of vasospasm may change, but these events are rare. Under normal circumstances, provocative testing involving angiography with administration of acetylcholine, ergot agents, or hyperventilation can be performed. However, this type of investigation should be limited to specialized centers and should not be performed in the acute phase of the disease.12
Treatment of suspected coronary vasospasm in patients receiving 5-FU involves stopping the infusion and administering calcium channel blockers or oral nitrates to relieve anginal symptoms.13 5-FU-induced coronary artery vasospasm has a 90% rate of recurrence with subsequent infusions.8 If possible, alternate chemotherapy regimens should be considered once coronary artery vasospasm has been identified.14,15 If further 5-FU use is required, or if benefits are deemed to outweigh risks, infusions should be given in an inpatient setting with continuous cardiac monitoring.16
Calcium channel blockers and oral nitrates have been found to produce benefit in patients in acute settings; however, there is little evidence to attest to their effectiveness as prophylactic agents in those receiving 5-FU. Some reports demonstrate episodes where both calcium channel blockers and oral nitrates failed to prevent subsequent vasospasms.17 Although this was the case for our patient, short-acting sublingual nitroglycerin seemed to be effective in reducing the frequency of anginal symptoms.
Long-term outcomes have not been well investigated for patients with 5-FU-induced coronary vasospasm. However, many case reports show improvements in left ventricular function between 8 and 15 days after discontinuation of 5-FU.7,10 Although this would be a valuable topic for further research, the rarity of this phenomenon creates limitations.
Conclusions
5-FU is a first-line chemotherapy for gastrointestinal cancers that is generally well tolerated but may be associated with potentially life-threatening cardiotoxic effects, of which coronary artery vasospasm is the most common. Coronary artery vasospasm presents with anginal chest pain and ST elevations on ECG that can be indistinguishable from acute coronary syndrome. Diagnosis requires cardiac catheterization, which will reveal patent coronary arteries. Infusional administration of 5-FU may be more likely to produce late cardiotoxic effects and a longer period of persistent symptoms, necessitating close monitoring for days or even weeks from last administration of 5-FU. Coronary artery vasospasm should be treated with anti-anginal medications, though varying degrees of effectiveness can be seen; clinicians should remain vigilant for recurrent episodes of chest pain despite treatment.
1. Wacker A, Lersch C, Scherpinski U, Reindl L, Seyfarth M. High incidence of angina pectoris in patients treated with 5-fluorouracil. A planned surveillance study with 102 patients. Oncology. 2003;65(2):108-112. doi:10.1159/000072334
2. World Health Organization Model List of Essential Medicines, 21st List, 2019. Accessed April 14, 2021. https://apps.who.int/iris/rest/bitstreams/1237479/retrieve
3. Jensen SA, Sørensen JB. Risk factors and prevention of cardiotoxicity induced by 5-fluorouracil or capecitabine. Cancer Chemother Pharmacol. 2006;58(4):487-493. doi:10.1007/s00280-005-0178-1
4. Shoemaker LK, Arora U, Rocha Lima CM. 5-fluorouracil-induced coronary vasospasm. Cancer Control. 2004;11(1):46-49. doi:10.1177/107327480401100207
5. Luwaert RJ, Descamps O, Majois F, Chaudron JM, Beauduin M. Coronary artery spasm induced by 5-fluorouracil. Eur Heart J. 1991;12(3):468-470. doi:10.1093/oxfordjournals.eurheartj.a059919
6. Saif MW, Shah MM, Shah AR. Fluoropyrimidine-associated cardiotoxicity: revisited. Expert Opin Drug Saf. 2009;8(2):191-202. doi:10.1517/14740330902733961
7. Patel B, Kloner RA, Ensley J, Al-Sarraf M, Kish J, Wynne J. 5-Fluorouracil cardiotoxicity: left ventricular dysfunction and effect of coronary vasodilators. Am J Med Sci. 1987;294(4):238-243. doi:10.1097/00000441-198710000-00004
8. Sara JD, Kaur J, Khodadadi R, et al. 5-fluorouracil and cardiotoxicity: a review. Ther Adv Med Oncol. 2018;10:1758835918780140. Published 2018 Jun 18. doi:10.1177/1758835918780140
9. Hansen RM, Ryan L, Anderson T, et al. Phase III study of bolus versus infusion fluorouracil with or without cisplatin in advanced colorectal cancer. J Natl Cancer Inst. 1996;88(10):668-674. doi:10.1093/jnci/88.10.668
10. Kim SM, Kwak CH, Lee B, et al. A case of severe coronary spasm associated with 5-fluorouracil chemotherapy. Korean J Intern Med. 2012;27(3):342-345. doi:10.3904/kjim.2012.27.3.342
11. Swarup S, Patibandla S, Grossman SA. Coronary Artery Vasospasm. StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2021.
12. Beijk MA, Vlastra WV, Delewi R, et al. Myocardial infarction with non-obstructive coronary arteries: a focus on vasospastic angina. Neth Heart J. 2019;27(5):237-245. doi:10.1007/s12471-019-1232-7
13. Giza DE, Boccalandro F, Lopez-Mattei J, et al. Ischemic heart disease: special considerations in cardio-oncology. Curr Treat Options Cardiovasc Med. 2017;19(5):37. doi:10.1007/s11936-017-0535-5
14. Meydan N, Kundak I, Yavuzsen T, et al. Cardiotoxicity of de Gramont’s regimen: incidence, clinical characteristics and long-term follow-up. Jpn J Clin Oncol. 2005;35(5):265-270. doi:10.1093/jjco/hyi071
15. Senkus E, Jassem J. Cardiovascular effects of systemic cancer treatment. Cancer Treat Rev. 2011;37(4):300-311. doi:10.1016/j.ctrv.2010.11.001
16. Rezkalla S, Kloner RA, Ensley J, et al. Continuous ambulatory ECG monitoring during fluorouracil therapy: a prospective study. J Clin Oncol. 1989;7(4):509-514. doi:10.1200/JCO.1989.7.4.509
17. Akpek G, Hartshorn KL. Failure of oral nitrate and calcium channel blocker therapy to prevent 5-fluorouracil-related myocardial ischemia: a case report. Cancer Chemother Pharmacol. 1999;43(2):157-161. doi:10.1007/s002800050877
1. Wacker A, Lersch C, Scherpinski U, Reindl L, Seyfarth M. High incidence of angina pectoris in patients treated with 5-fluorouracil. A planned surveillance study with 102 patients. Oncology. 2003;65(2):108-112. doi:10.1159/000072334
2. World Health Organization Model List of Essential Medicines, 21st List, 2019. Accessed April 14, 2021. https://apps.who.int/iris/rest/bitstreams/1237479/retrieve
3. Jensen SA, Sørensen JB. Risk factors and prevention of cardiotoxicity induced by 5-fluorouracil or capecitabine. Cancer Chemother Pharmacol. 2006;58(4):487-493. doi:10.1007/s00280-005-0178-1
4. Shoemaker LK, Arora U, Rocha Lima CM. 5-fluorouracil-induced coronary vasospasm. Cancer Control. 2004;11(1):46-49. doi:10.1177/107327480401100207
5. Luwaert RJ, Descamps O, Majois F, Chaudron JM, Beauduin M. Coronary artery spasm induced by 5-fluorouracil. Eur Heart J. 1991;12(3):468-470. doi:10.1093/oxfordjournals.eurheartj.a059919
6. Saif MW, Shah MM, Shah AR. Fluoropyrimidine-associated cardiotoxicity: revisited. Expert Opin Drug Saf. 2009;8(2):191-202. doi:10.1517/14740330902733961
7. Patel B, Kloner RA, Ensley J, Al-Sarraf M, Kish J, Wynne J. 5-Fluorouracil cardiotoxicity: left ventricular dysfunction and effect of coronary vasodilators. Am J Med Sci. 1987;294(4):238-243. doi:10.1097/00000441-198710000-00004
8. Sara JD, Kaur J, Khodadadi R, et al. 5-fluorouracil and cardiotoxicity: a review. Ther Adv Med Oncol. 2018;10:1758835918780140. Published 2018 Jun 18. doi:10.1177/1758835918780140
9. Hansen RM, Ryan L, Anderson T, et al. Phase III study of bolus versus infusion fluorouracil with or without cisplatin in advanced colorectal cancer. J Natl Cancer Inst. 1996;88(10):668-674. doi:10.1093/jnci/88.10.668
10. Kim SM, Kwak CH, Lee B, et al. A case of severe coronary spasm associated with 5-fluorouracil chemotherapy. Korean J Intern Med. 2012;27(3):342-345. doi:10.3904/kjim.2012.27.3.342
11. Swarup S, Patibandla S, Grossman SA. Coronary Artery Vasospasm. StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2021.
12. Beijk MA, Vlastra WV, Delewi R, et al. Myocardial infarction with non-obstructive coronary arteries: a focus on vasospastic angina. Neth Heart J. 2019;27(5):237-245. doi:10.1007/s12471-019-1232-7
13. Giza DE, Boccalandro F, Lopez-Mattei J, et al. Ischemic heart disease: special considerations in cardio-oncology. Curr Treat Options Cardiovasc Med. 2017;19(5):37. doi:10.1007/s11936-017-0535-5
14. Meydan N, Kundak I, Yavuzsen T, et al. Cardiotoxicity of de Gramont’s regimen: incidence, clinical characteristics and long-term follow-up. Jpn J Clin Oncol. 2005;35(5):265-270. doi:10.1093/jjco/hyi071
15. Senkus E, Jassem J. Cardiovascular effects of systemic cancer treatment. Cancer Treat Rev. 2011;37(4):300-311. doi:10.1016/j.ctrv.2010.11.001
16. Rezkalla S, Kloner RA, Ensley J, et al. Continuous ambulatory ECG monitoring during fluorouracil therapy: a prospective study. J Clin Oncol. 1989;7(4):509-514. doi:10.1200/JCO.1989.7.4.509
17. Akpek G, Hartshorn KL. Failure of oral nitrate and calcium channel blocker therapy to prevent 5-fluorouracil-related myocardial ischemia: a case report. Cancer Chemother Pharmacol. 1999;43(2):157-161. doi:10.1007/s002800050877