User login
How do you dismiss a patient from your practice’s care?
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
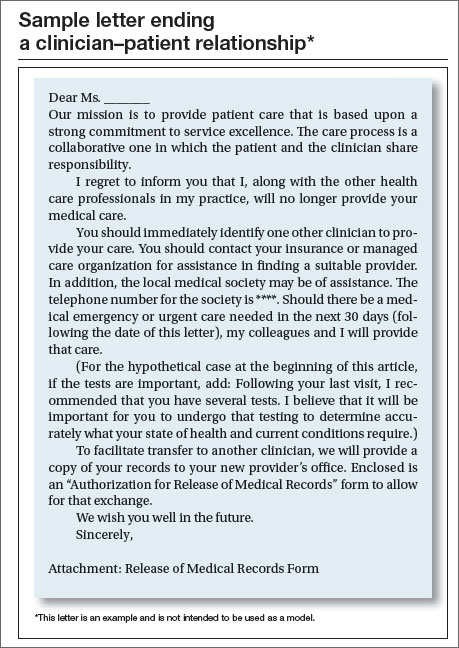
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |


The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
|
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |
The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Joseph S. Sanfilippo, MD, MBA, and Steven R. Smith, JD
|
| Joseph S. Sanfilippo, MD, MBA is Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility, at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
|
Steven R. Smith, JD, is Professor of Law and Dean Emeritus at California Western School of Law, San Diego, California. |
|
Shirley M. Pruitt, BSN, JD, is a Partner in the firm of Yates, McLamb & Weyher, LLP, in Raleigh, North Carolina. She is an OBG Management Contributing Editor. |
The authors report no financial relationships relevant to this article.
*The “facts” of this case are based on actual cases but are a composite of several events and do not reflect a specific case.
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Case: Patient becomes a liability when nonadherant to prescribed tests
MC, a 42-year-old woman (G1P1001), presents for an office visit. As the medical assistant hands you the chart, she says, “Good luck with this one. She yelled at me because you were 20 minutes behind schedule. She didn’t like sitting in the waiting room.” You greet the patient, obtain her medical history, proceed with a physical examination, and outline a management plan. You recall from the chart that you operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the operating room (OR) for a laparotomy to control bleeding. The patient has not brought this up since being discharged from the hospital.
During the current office visit, the esprit de corps in the consultation room is a bit uncomfortable, and you sense the patient is not happy. You leave the examination room and discuss the management plan with the nurse, who then returns to the patient to review the plan. The patient is unhappy with the battery of tests you have ordered but tells the nurse that she will comply.
One week later the nurse follows up with the patient by phone because she has not obtained the requested lab tests. The nurse reports to you, “She read me the riot act: ‘Why do I need all these tests? They are expensive.’ The patient indicated that she has no understanding as to why the tests were ordered in the first place.” After a discussion with you, the nurse calls the patient back in an effort to clarify her understanding of the need for the tests. The patient hangs up on her in the middle of the conversation.
The office manager tracks you down to discuss this patient. “Enough is enough,” she exclaims. “This patient is harassing the staff. She told the nurse what tests she herself believes are best and that those are the only ones she will comply with.” Your office manager states that this patient is “a liability.”
What are your choices at this point? You have thought about picking up the phone and calling her. You have considered ending her relationship with your practice. You ask yourself again, what is the best approach?
Patients have the legal right to “dismiss” or change health care providers at any time and for almost any reason without notice. But that right is not reciprocal—clinicians have a legal duty not to abandon a patient and an ethical duty to promote continuity of patient care. A clinician may dismiss a patient from his or her practice (other than for a discriminatory reason that violates ethical or legal limitations), but it must be done in the proper way.
We examine the legal, practical, and ethical issues in dismissing a patient, and how to do it without unnecessary risk. In addition, we will look at a new issue that sometimes arises in these circumstances—managed care limitations.
Physicians’ ethical obligations
The American Medical Association suggests the following ethical consideration:
Reference
- American Medical Association Council on Ethical and Judicial Affairs. Opinion 10.015. The Patient-Physician Relationship. Code of Medical Ethics. American Medical Association. http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion10015.page. Issued December 2001. Accessed May 8, 2015.
Legal and medical issues
Why would you end a clinician−patient relationship?
There are a number of reasons for dismissing a patient, including1,2:
- the patient’s failure to comply with a treatment plan (probably the most frequent reason)
- persistent, inappropriate, rude, or disruptive behavior
- falsifying medical history
- seductive behavior toward health care professionals or staff
- Sentinel incident (verbal threat, violence, or criminal activity—as when a patient threatens or inappropriately touches or hits your staff)
- failure to pay billed charges (this can raise special legal issues).
The legal details vary from state to state, but fortunately there is sufficient similarity that best practices can be determined. The law starts with the proposition that ordinarily professionals may choose their patients or clients. There are limits, however, in state and federal law. A clinician may not discriminate based, for example, on ethnicity, religion, gender, or sexual orientation. In addition, the Americans with Disabilities Act limits the basis for not providing care to a patient.3
Limiting factors when dismissing a patient
Once a patient has been accepted and a professional relationship has begun, the clinician has a duty of continued care and must act reasonably to end the relationship in a way that protects the patient’s well-being.
Other recognized limitations to the ending of a treatment relationship exist. These are:
- In an emergency situation or during ongoing care in which it proves unfeasible to find another physician. At the extreme, a surgeon may not leave in the middle of surgery. Less clear, but still problematic, is the obstetrician who wants to dismiss a patient 1 or 2 weeks before an expected delivery. In any event, a clinician should not leave a patient at a critical stage without giving reasonable notice or making suitable arrangements for the attendance of another equally competent substitute.
- When there is no other health care provider available who could provide the continuity of care the clinician has begun. This limitation probably arises from the frontier days (when it was much more common for no other health care professional to be available who could provide the continuity of care the clinician began). A modern version of this might be a patient in an HMO who does not have other physicians of the same subspecialty available who are taking patients. This, of course, requires consultation with the managed care organization.
Abandonment
The legal and ethical issues are essentially related to “abandonment”—dismissing a patient improperly. Technically, abandonment is a form of negligence (the clinician does not act reasonably to protect the patient’s interests). The Oklahoma Supreme Court put it clearly: “When further medical and/or surgical attention is needed, a physician may terminate the doctor−patient relationship only after giving reasonable notice and affording an ample opportunity for the patient to secure other medical attention from other physicians” (emphasis added).4–6
How to end a patient relationship
Always send a letter
Two elements must be taken into account when dismissing a patient:
- reasonable notice
- reasonable opportunity to find another clinician.
Together, these elements mean that the intention of ending the clinician−patient relationship and the importance of finding an alternative care provider must be clearly communicated to the patient. That communication needs to be in writing—both to get the patient’s attention and as clear proof of what was said.
Some experts suggest that the best process is to have a face-to-face meeting with the patient followed by a letter. A goal of such a meeting is to make the parting as amicable as possible. It may seem more professional for a clinician to communicate such an important matter in person. The risk is that it may become a confrontation that exacerbates the situation because one or both parties may have some built-up emotion. It, therefore, depends on the circumstances as to whether such a meeting is desirable. Even if there is an oral conversation, it must be followed up with a letter to the patient.
A reasonable time frame to give the patient to find another clinician is commonly a maximum of 30 days of follow-up and emergency care. A set period of time may be a legitimate starting point but it needs to be adjusted in lieu of special circumstances, such as the availability of other similar specialists in the vicinity who are taking new patients or managed care complications. A specific time period should be indicated, along with an agreement to provide care during that time period in “emergency” or “urgent” circumstances. Of course, ongoing care also should be continued for a reasonable time (30 days is often reasonable, as mentioned). It may be best to also discuss any specific ongoing issues that should be attended to (such as the recommended tests in our opening case).
There is disagreement among experts as to whether a general statement of the reasons for ending the care relationship should be included in the letter. The argument for doing so is that, without a stated reason, the patient may call to ask why. The other side of the argument is that it adds an element of accusation; the patient undoubtedly knows what the problem is. Not writing down the reasons seems the better part of valor, especially if there has been an oral conversation.7,8
The box above provides an example of a letter to a patient (but not a model). Experts agree that the letter should be sent by certified mail with return receipt. Should the patient reject the letter, a regular delivery letter should be sent with full documentation kept in the file of the time and place it was mailed.
Managed care considerations
A consideration of increasing importance is managed care. Before taking any action, ensure that the managed care contract(s) (including federal or state government programs) have provisions concerning patient dismissals. These may be as simple as notifying the organization as to any time limits for care or of the process of dismissal.
Make sure your staff knows
Your scheduling staff needs to know with clarity the rules for scheduling (or not scheduling) this patient in the future. As a general matter, the better course of action is to allow an appointment if the patient reports that it is an emergency, whether the staff believes it is or not. In such cases it may be good to document to the patient that the emergency care does not constitute reestablishing a regular clinician−patient relationship.
Document everything
The patient’s record, at a minimum, should contain a copy of the letter sent to the patient and a log of any conversations with her about ending the relationship. Keep your own notes concerning the disruption or problems with the patient over time.
Are there risks of a malpractice lawsuit?
The abandonment claim is, of course, one possibility for a malpractice lawsuit. That is why documentation and careful communication are so important. This is one area in which having legal advice when developing a letter template should be part of the ongoing relationship with a health law attorney.
There is another malpractice risk illustrated in our hypothetical case. The physician “operated on her 8 months ago and there was a complication/maloccurrence in which postoperative bleeding necessitated return to the OR and laparotomy to control bleeding.” Malpractice claims (as opposed to actual malpractice occurrences) most often arise because of bad communication with patients or when patients feel ignored. The clinician is thus between a rock and a hard place. On one hand, by ending this relationship, the clinician could well precipitate a claim based primarily on the earlier “maloccurrence.” On the other hand, continuing to treat a patient who is resisting care and creating problems with the staff has its own difficulties. It may be time for the health care professional to discuss the matter with an attorney.
Although not present in this hypothetical case, ending a patient relationship because of nonpayment of professional fees is also a touchy situation. It can be one of the other precipitating events for malpractice claims, and calls for special care.
Tread with care
Having to dismiss a patient is almost always a difficult process. The decision neither can be made lightly nor implemented sloppily. Because it is difficult, it calls on professionals to be particularly careful to not cut essential corners.9
Case: Resolved
You ask the nurse to note the details of her follow-up phone conversation with the patient in the chart. You then call MC to explain the importance of the tests. She says she is unavailable to talk right now, so you ask her to come in for an appointment, free of charge. The patient makes an appointment but does not show.
You send a letter by certified mail describing the medical necessity for the tests and that her lack of adherence and refusal to come to the office have compelled you to end your clinician−patient relationship. You write that she should immediately identify another health care professional and suggest that she contact her managed care organization for assistance. You note that, should there be a medical emergency or urgent care needed in the next 30 days, you will provide that care. You enclose a release of medical records form in the letter.
In the patient’s record you note the details of the phone conversation and ask the office manager to add that the patient was a no show for her appointment. You include a copy of the certified letter and proof of mailing in the chart.
Two weeks later, the office manager reports that she is sending the patient’s records to another physician upon receipt of the release of medical records form from the patient.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
1. Kodner C. Challenging physician-patient interactions. FP Essentials. ed 354. AAFP home study. Leawood, KS: American Academy of Family Physicians; November 2008.
2. Harris SM. Take care when firing a patient. Am Med News. http://www.ama-assn.org/amed- news/2008/02/04/bica0204 .htm. Published February 4, 2008. Accessed May 8, 2015.
3. Lynch HF. Discrimination at the doctor’s office. N Engl J Med. 2013;386(18):1668–1670.
4. Jackson v Oklahoma Memorial Hospital, 909 P.2d 765 (OK 1995). http://law.justia.com/cases/oklahoma/supreme-court/1995/4226-1.html. Accessed May 8, 2015.
5. Randolph DS, Burkett TM. When physicians fire patients: avoiding patient “abandonment” lawsuits. J Okla State Med Assoc. 2009;102(11):356–358.
6. Crauman R, Baruch J. Abandonment in the physician-patient relationship. Med Health R I. 2004;87(5):154–156.
7. Cepelewicz BB. Firing a patient: when its needed and how to handle it correctly. Med Econ. 2014;91(2):42–43.
8. Santalucia C, Michota F. When and how is it appropriate to terminate the physician-patient relationship? Cleve Clin J Med. 2004;71(3):179–183.
9. Lippman H, Davenport J. Patient dismissal: the right way to do it. J Fam Pract. 2011;60(3):135–140. http://www.jfponline.com/specialty-focus/practice-management/article/patient-dismissal-the-right-way-to-do-it/30f9501e8b3eb6ddaf6dd67ce88e0d16.html. Accessed May 8, 2015.
In this article
- Physicians’ ethical obligations
- Sample letter ending a clinician–patient relationship

Lost needle tip during hysterectomy
CASE: Lost needle tip
A 36-year-old woman (G3 P2012) with stress urinary incontinence (SUI) and abnormal uterine bleeding presented to a gynecologist. She had explored medical therapy for her SUI with no symptom improvement. She had a previous tubal ligation, and the gynecologist ordered urodynamic testing, the results of which led to a discussion of vaginal hysterectomy; anterior, posterior colporrhaphy; and mesh placement. It was felt that the patient had a number of risk factors for incontinence (including pregnancy with vaginal delivery, well-controlled diabetes mellitus, and obesity). She had a long-standing history of chronic pelvic pain, with an established diagnosis of diverticulosis with episodes of diverticulitis in the past.
The gynecologist had the patient keep a bladder diary for 1 week. When asked, the patient reported no problems with sexual dysfunction, stating that her quality of life was “fine” except for the vaginal bleeding and loss of urine refractory to medical therapy. The Urogenital Distress Inventory was administered, and it identified frequent urination, leakage, and incontinence related to activities. An Incontinence Impact Questionnaire also was administered. Physical examination included cotton-tipped swab urethral, or Q-tip, test and cough stress test as part of POP-Q (Pelvic Organ Prolapse Quantification system) evaluation. Urinary tract infection was ruled out. The gynecologist counseled the patient about possible medical therapies for urinary incontinence, and she requested definitive surgery.
The gynecologist obtained informed consent for surgery that included preoperative discussion of potential surgical complications, including bleeding, infection, trauma to surrounding structures, and the possibility of additional surgical procedures secondary to complications. The gynecologist also discussed transvaginal tape versus transobturator tape (TOT) placement, including potential complications and sequelae. The final planned procedure, which was performed by the gynecologist, included vaginal hysterectomy, anterior colporrhaphy, and TOT placement.
Intraoperatively, the patient was identified (upon entering the operating room [OR]); time-out occurred, and the gynecologist proceeded with surgery. During the procedure, the tip of a needle broke off. The gynecologist noted the broken tip as he removed the needle and handed it to the surgical technician. The gynecologist palpated the sidewall in the presumed area of the needle tip and felt it easily. He attempted to remove the tip, but his effort was fruitless. He made the intraoperative decision to leave the tip in situ. A needle and sponge count was performed, reported as correct, and it was felt there was no indication for imaging of the pelvis. The circulating nurse filled out an incident report immediately following the surgery, noting the missing needle tip. The occurrence was discussed by the surgical committee at the hospital.
Postoperatively, while the patient was in the hospital, she was informed of the intra-operative incident.
Three months later, the patient reported vaginal and pelvic pain on the sidewall in the area of the lost needle tip, with radiating pain down the involved extremity. A segment of the TOT was noted to be protruding into the vagina, and this was addressed in the OR with “trimming of such.”
Postoperatively, again the patient reported pain on the involved side. She sought the opinion of another gynecologist, who subsequently performed surgical intervention to remove the needle tip. Her symptoms improved.
The patient sued the original gynecologic surgeon, alleging pain and suffering from the surgery involving the lost needle tip.
What’s the verdict?
A defense verdict was awarded.
Medical teaching points
Medical evaluation seemed appropriate. Parity is associated with SUI (but not urge incontinence). In general, urinary incontinence is more commonly associated with a history of lower urinary tract infections. The patient in this case was asked about and evaluated for:
- stress incontinence (associated with loss of urine with sneezing, coughing, and exercise)
- urge incontinence (inability to reach the bathroom in time)
- frequency of urination, especially while sleeping
- overflow incontinence
- overall loss of bladder control.
Was information on the broken needle handled appropriately? This case explores the question of what, if any, obligation the surgeon and hospital system have to the patient when informing her of a broken needle and the intraoperative decision-making process that led to its staying in place. When such a situation occurs, which is very uncommon, should an intraoperative x-ray be performed to assess the location of the needle tip? Should the patient automatically be brought back to the OR for removal?
The surgeon’s concern was a legitimate one—that additional attempts at removal could lead to complications far worse than having a small segment of a needle left in place. After all, shrapnel, bullets, etc, remain lodged in various locations throughout the body without subsequent ill effects. He did discuss with the patient the fact that a needle segment was left in the muscle wall. But how do you assess postoperative pelvic pain in a patient who had preoperative chronic pelvic pain? These are questions we as clinicians ask. Clearly, there are no black-and-white answers, and we will call upon our legal consultants for their expertise in addressing these queries.
From the gynecologic perspective, however, it is of paramount importance to address the patient’s postoperative vaginal pain and determine the best management approach. In this case the TOT, and its association with a 21.5% complication rate, including reported vaginal extrusion, introduces a whole new set of concerns.1 The TOT use in itself raises the question of liability on the part of the surgeon. This mesh has more than 150 associated complications, including obturator nerve injuries, extensive blood loss, and ischiorectal fossa abscesses.2 Once a device comes upon the radar screen of the US Food and Drug Administration for significant complications, where does that leave the clinician in regard to litigation? Let’s look to our legal colleagues for their insight and expertise.
Legal considerations
Given the facts in this case, it is not surprising that it resulted in a defense verdict. The majority of cases filed are ultimately disposed of in favor of the medical defendants, and the majority of medical malpractice cases that go to trial result in defense verdicts.
Medical malpractice, or “professional negligence,” consists of a claim that a medical professional had a duty of care to the patient, a breach of that duty, injury to the patient, and a causal connection (“causation”) between the breach of duty and the injury. It is the obligation of the plaintiff to prove the elements of negligence by a preponderance of the evidence.
Were the surgeon’s actions in line with other surgeons’ expected actions? The issue of the breach of the duty of care essentially is the question of whether the physician acted similarly to a reasonably careful practitioner of the same specialty under the same circumstances. Doctors are not held to a standard of perfection. That is, not every injury or bad outcome is negligence—only those injuries that result from actions, or inactions, that were not within the level of care acceptable in the profession.
Why would this patient file a lawsuit? The injury was not trivial (it had both pain and cost associated with it), but it was not catastrophic, and the negligence was going to be difficult to prove. Furthermore, lawsuits are expensive in terms of time, energy, and emotional commitment—few people file them for the fun of it. We can only speculate on the answer to the question but, frequently, such claims are a search for the answer to “What happened, and why?” or a reaction to feeling ignored or disrespected. There is little in the case facts that we have to work with to indicate what the communication was between the gynecologist and the patient and her family. The statement of facts, however, leaves the impression that communication deteriorated as the postoperative pain endured.
Some additional areas of potential claims for liability in this case include:
- The explanation for the needle breaking during surgery is unclear from the brief statement of case facts. There might be malpractice liability if the surgeon was unreasonable in how the needle was used, used the wrong needle, or ignored defects in the needle.
- The surgeon tried unsuccessfully to retrieve the needle during the original surgery. If the surgeon’s failure to retrieve the needle was because of inadequate training, lack of care or the like, it might be seen as the “cause” of the patient’s injuries.
- The fact that a second surgeon was able to remove the needle tip, which resolved the patient’s pain, may raise the question of whether the first surgeon’s decision not to seek to remove it in response to the continuing pain was reasonable. If the first surgeon did not want to remove the needle tip, a question might be raised about whether that surgeon should have referred the patient to another surgeon. (The patient ultimately found another surgeon on her own.)
- Regarding use of TOT: A 21.5% complication rate ordinarily would be a significant factor to consider in a decision to use the tape. Physicians are responsible for keeping up with current developments in the devices and pharmaceuticals they use. Therefore, if information on the complication rate was available, the surgeon’s documentation should reflect the basis for choosing to use the tape. More important, the surgeon should document a conversation with the patient about the risks and benefits of using the TOT and the discussion of alternatives to its use.
What factors could have tipped the case toward the defense?
The defense verdict indicates that the jury determined there was no negligence, or that the patient could not prove any of these potential bases of liability. As noted above, what may have helped the defense is the fact that the surgeon documented the details of the informed consent conversation, including that “discussion was carried out regarding” the tape. The informed consent process is an important opportunity for communication with the patient, and a chance to make sure that expectations are reasonable. Liability for the failure of informed consent is not common. When something has gone wrong, however, it can matter whether the problem was something mentioned in the informed consent process. In addition, it was positive that postoperatively the patient was informed of the broken needle—although it is not clear who informed her about it.
A couple of other legal issues are worth noting. From our fact scenario we do not know what was documented in the incident report filed by the circulating nurse and reviewed by the surgical committee. We also do not know whether the plaintiff was privy to the incident report document. The surgical committee is likely a peer-review committee, and most states provide some privilege for such committees (to avoid disclosure of committee information for discovery or at trial). The deliberations and conclusions of the committee, therefore, were likely privileged. However, incident reports are frequently used for other purposes, such as administrative reports, that are not privileged—so the incident report often is determined to be discoverable depending on the interpretation of the state’s law.
No winner in this case
Despite the defense verdict, the physician was not really the “winner” after having spent a great deal of time, energy, money, and emotion defending this suit. Ultimately, the goal is not to win malpractice cases but to avoid them—in this case, among other things, by being frank with patients about expectations, keeping an open line of communication with patients when they are concerned with an outcome that is less than ideal, and referring a patient when it may be appropriate.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Bladder sling risks, complications and side effects. DrugWatch Web site. http://www.drugwatch.com/trans vaginal-mesh/bladder-sling/. Updated January 2, 2015. Accessed February 13, 2015.
2. Boyles SH, Edwards R, Gregory W, Clark A. Complications associated with transobturator sling procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(1):19–22.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |


Disclosures
The authors report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
The authors report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
The authors report no financial relationships relevant to this article.
CASE: Lost needle tip
A 36-year-old woman (G3 P2012) with stress urinary incontinence (SUI) and abnormal uterine bleeding presented to a gynecologist. She had explored medical therapy for her SUI with no symptom improvement. She had a previous tubal ligation, and the gynecologist ordered urodynamic testing, the results of which led to a discussion of vaginal hysterectomy; anterior, posterior colporrhaphy; and mesh placement. It was felt that the patient had a number of risk factors for incontinence (including pregnancy with vaginal delivery, well-controlled diabetes mellitus, and obesity). She had a long-standing history of chronic pelvic pain, with an established diagnosis of diverticulosis with episodes of diverticulitis in the past.
The gynecologist had the patient keep a bladder diary for 1 week. When asked, the patient reported no problems with sexual dysfunction, stating that her quality of life was “fine” except for the vaginal bleeding and loss of urine refractory to medical therapy. The Urogenital Distress Inventory was administered, and it identified frequent urination, leakage, and incontinence related to activities. An Incontinence Impact Questionnaire also was administered. Physical examination included cotton-tipped swab urethral, or Q-tip, test and cough stress test as part of POP-Q (Pelvic Organ Prolapse Quantification system) evaluation. Urinary tract infection was ruled out. The gynecologist counseled the patient about possible medical therapies for urinary incontinence, and she requested definitive surgery.
The gynecologist obtained informed consent for surgery that included preoperative discussion of potential surgical complications, including bleeding, infection, trauma to surrounding structures, and the possibility of additional surgical procedures secondary to complications. The gynecologist also discussed transvaginal tape versus transobturator tape (TOT) placement, including potential complications and sequelae. The final planned procedure, which was performed by the gynecologist, included vaginal hysterectomy, anterior colporrhaphy, and TOT placement.
Intraoperatively, the patient was identified (upon entering the operating room [OR]); time-out occurred, and the gynecologist proceeded with surgery. During the procedure, the tip of a needle broke off. The gynecologist noted the broken tip as he removed the needle and handed it to the surgical technician. The gynecologist palpated the sidewall in the presumed area of the needle tip and felt it easily. He attempted to remove the tip, but his effort was fruitless. He made the intraoperative decision to leave the tip in situ. A needle and sponge count was performed, reported as correct, and it was felt there was no indication for imaging of the pelvis. The circulating nurse filled out an incident report immediately following the surgery, noting the missing needle tip. The occurrence was discussed by the surgical committee at the hospital.
Postoperatively, while the patient was in the hospital, she was informed of the intra-operative incident.
Three months later, the patient reported vaginal and pelvic pain on the sidewall in the area of the lost needle tip, with radiating pain down the involved extremity. A segment of the TOT was noted to be protruding into the vagina, and this was addressed in the OR with “trimming of such.”
Postoperatively, again the patient reported pain on the involved side. She sought the opinion of another gynecologist, who subsequently performed surgical intervention to remove the needle tip. Her symptoms improved.
The patient sued the original gynecologic surgeon, alleging pain and suffering from the surgery involving the lost needle tip.
What’s the verdict?
A defense verdict was awarded.
Medical teaching points
Medical evaluation seemed appropriate. Parity is associated with SUI (but not urge incontinence). In general, urinary incontinence is more commonly associated with a history of lower urinary tract infections. The patient in this case was asked about and evaluated for:
- stress incontinence (associated with loss of urine with sneezing, coughing, and exercise)
- urge incontinence (inability to reach the bathroom in time)
- frequency of urination, especially while sleeping
- overflow incontinence
- overall loss of bladder control.
Was information on the broken needle handled appropriately? This case explores the question of what, if any, obligation the surgeon and hospital system have to the patient when informing her of a broken needle and the intraoperative decision-making process that led to its staying in place. When such a situation occurs, which is very uncommon, should an intraoperative x-ray be performed to assess the location of the needle tip? Should the patient automatically be brought back to the OR for removal?
The surgeon’s concern was a legitimate one—that additional attempts at removal could lead to complications far worse than having a small segment of a needle left in place. After all, shrapnel, bullets, etc, remain lodged in various locations throughout the body without subsequent ill effects. He did discuss with the patient the fact that a needle segment was left in the muscle wall. But how do you assess postoperative pelvic pain in a patient who had preoperative chronic pelvic pain? These are questions we as clinicians ask. Clearly, there are no black-and-white answers, and we will call upon our legal consultants for their expertise in addressing these queries.
From the gynecologic perspective, however, it is of paramount importance to address the patient’s postoperative vaginal pain and determine the best management approach. In this case the TOT, and its association with a 21.5% complication rate, including reported vaginal extrusion, introduces a whole new set of concerns.1 The TOT use in itself raises the question of liability on the part of the surgeon. This mesh has more than 150 associated complications, including obturator nerve injuries, extensive blood loss, and ischiorectal fossa abscesses.2 Once a device comes upon the radar screen of the US Food and Drug Administration for significant complications, where does that leave the clinician in regard to litigation? Let’s look to our legal colleagues for their insight and expertise.
Legal considerations
Given the facts in this case, it is not surprising that it resulted in a defense verdict. The majority of cases filed are ultimately disposed of in favor of the medical defendants, and the majority of medical malpractice cases that go to trial result in defense verdicts.
Medical malpractice, or “professional negligence,” consists of a claim that a medical professional had a duty of care to the patient, a breach of that duty, injury to the patient, and a causal connection (“causation”) between the breach of duty and the injury. It is the obligation of the plaintiff to prove the elements of negligence by a preponderance of the evidence.
Were the surgeon’s actions in line with other surgeons’ expected actions? The issue of the breach of the duty of care essentially is the question of whether the physician acted similarly to a reasonably careful practitioner of the same specialty under the same circumstances. Doctors are not held to a standard of perfection. That is, not every injury or bad outcome is negligence—only those injuries that result from actions, or inactions, that were not within the level of care acceptable in the profession.
Why would this patient file a lawsuit? The injury was not trivial (it had both pain and cost associated with it), but it was not catastrophic, and the negligence was going to be difficult to prove. Furthermore, lawsuits are expensive in terms of time, energy, and emotional commitment—few people file them for the fun of it. We can only speculate on the answer to the question but, frequently, such claims are a search for the answer to “What happened, and why?” or a reaction to feeling ignored or disrespected. There is little in the case facts that we have to work with to indicate what the communication was between the gynecologist and the patient and her family. The statement of facts, however, leaves the impression that communication deteriorated as the postoperative pain endured.
Some additional areas of potential claims for liability in this case include:
- The explanation for the needle breaking during surgery is unclear from the brief statement of case facts. There might be malpractice liability if the surgeon was unreasonable in how the needle was used, used the wrong needle, or ignored defects in the needle.
- The surgeon tried unsuccessfully to retrieve the needle during the original surgery. If the surgeon’s failure to retrieve the needle was because of inadequate training, lack of care or the like, it might be seen as the “cause” of the patient’s injuries.
- The fact that a second surgeon was able to remove the needle tip, which resolved the patient’s pain, may raise the question of whether the first surgeon’s decision not to seek to remove it in response to the continuing pain was reasonable. If the first surgeon did not want to remove the needle tip, a question might be raised about whether that surgeon should have referred the patient to another surgeon. (The patient ultimately found another surgeon on her own.)
- Regarding use of TOT: A 21.5% complication rate ordinarily would be a significant factor to consider in a decision to use the tape. Physicians are responsible for keeping up with current developments in the devices and pharmaceuticals they use. Therefore, if information on the complication rate was available, the surgeon’s documentation should reflect the basis for choosing to use the tape. More important, the surgeon should document a conversation with the patient about the risks and benefits of using the TOT and the discussion of alternatives to its use.
What factors could have tipped the case toward the defense?
The defense verdict indicates that the jury determined there was no negligence, or that the patient could not prove any of these potential bases of liability. As noted above, what may have helped the defense is the fact that the surgeon documented the details of the informed consent conversation, including that “discussion was carried out regarding” the tape. The informed consent process is an important opportunity for communication with the patient, and a chance to make sure that expectations are reasonable. Liability for the failure of informed consent is not common. When something has gone wrong, however, it can matter whether the problem was something mentioned in the informed consent process. In addition, it was positive that postoperatively the patient was informed of the broken needle—although it is not clear who informed her about it.
A couple of other legal issues are worth noting. From our fact scenario we do not know what was documented in the incident report filed by the circulating nurse and reviewed by the surgical committee. We also do not know whether the plaintiff was privy to the incident report document. The surgical committee is likely a peer-review committee, and most states provide some privilege for such committees (to avoid disclosure of committee information for discovery or at trial). The deliberations and conclusions of the committee, therefore, were likely privileged. However, incident reports are frequently used for other purposes, such as administrative reports, that are not privileged—so the incident report often is determined to be discoverable depending on the interpretation of the state’s law.
No winner in this case
Despite the defense verdict, the physician was not really the “winner” after having spent a great deal of time, energy, money, and emotion defending this suit. Ultimately, the goal is not to win malpractice cases but to avoid them—in this case, among other things, by being frank with patients about expectations, keeping an open line of communication with patients when they are concerned with an outcome that is less than ideal, and referring a patient when it may be appropriate.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
CASE: Lost needle tip
A 36-year-old woman (G3 P2012) with stress urinary incontinence (SUI) and abnormal uterine bleeding presented to a gynecologist. She had explored medical therapy for her SUI with no symptom improvement. She had a previous tubal ligation, and the gynecologist ordered urodynamic testing, the results of which led to a discussion of vaginal hysterectomy; anterior, posterior colporrhaphy; and mesh placement. It was felt that the patient had a number of risk factors for incontinence (including pregnancy with vaginal delivery, well-controlled diabetes mellitus, and obesity). She had a long-standing history of chronic pelvic pain, with an established diagnosis of diverticulosis with episodes of diverticulitis in the past.
The gynecologist had the patient keep a bladder diary for 1 week. When asked, the patient reported no problems with sexual dysfunction, stating that her quality of life was “fine” except for the vaginal bleeding and loss of urine refractory to medical therapy. The Urogenital Distress Inventory was administered, and it identified frequent urination, leakage, and incontinence related to activities. An Incontinence Impact Questionnaire also was administered. Physical examination included cotton-tipped swab urethral, or Q-tip, test and cough stress test as part of POP-Q (Pelvic Organ Prolapse Quantification system) evaluation. Urinary tract infection was ruled out. The gynecologist counseled the patient about possible medical therapies for urinary incontinence, and she requested definitive surgery.
The gynecologist obtained informed consent for surgery that included preoperative discussion of potential surgical complications, including bleeding, infection, trauma to surrounding structures, and the possibility of additional surgical procedures secondary to complications. The gynecologist also discussed transvaginal tape versus transobturator tape (TOT) placement, including potential complications and sequelae. The final planned procedure, which was performed by the gynecologist, included vaginal hysterectomy, anterior colporrhaphy, and TOT placement.
Intraoperatively, the patient was identified (upon entering the operating room [OR]); time-out occurred, and the gynecologist proceeded with surgery. During the procedure, the tip of a needle broke off. The gynecologist noted the broken tip as he removed the needle and handed it to the surgical technician. The gynecologist palpated the sidewall in the presumed area of the needle tip and felt it easily. He attempted to remove the tip, but his effort was fruitless. He made the intraoperative decision to leave the tip in situ. A needle and sponge count was performed, reported as correct, and it was felt there was no indication for imaging of the pelvis. The circulating nurse filled out an incident report immediately following the surgery, noting the missing needle tip. The occurrence was discussed by the surgical committee at the hospital.
Postoperatively, while the patient was in the hospital, she was informed of the intra-operative incident.
Three months later, the patient reported vaginal and pelvic pain on the sidewall in the area of the lost needle tip, with radiating pain down the involved extremity. A segment of the TOT was noted to be protruding into the vagina, and this was addressed in the OR with “trimming of such.”
Postoperatively, again the patient reported pain on the involved side. She sought the opinion of another gynecologist, who subsequently performed surgical intervention to remove the needle tip. Her symptoms improved.
The patient sued the original gynecologic surgeon, alleging pain and suffering from the surgery involving the lost needle tip.
What’s the verdict?
A defense verdict was awarded.
Medical teaching points
Medical evaluation seemed appropriate. Parity is associated with SUI (but not urge incontinence). In general, urinary incontinence is more commonly associated with a history of lower urinary tract infections. The patient in this case was asked about and evaluated for:
- stress incontinence (associated with loss of urine with sneezing, coughing, and exercise)
- urge incontinence (inability to reach the bathroom in time)
- frequency of urination, especially while sleeping
- overflow incontinence
- overall loss of bladder control.
Was information on the broken needle handled appropriately? This case explores the question of what, if any, obligation the surgeon and hospital system have to the patient when informing her of a broken needle and the intraoperative decision-making process that led to its staying in place. When such a situation occurs, which is very uncommon, should an intraoperative x-ray be performed to assess the location of the needle tip? Should the patient automatically be brought back to the OR for removal?
The surgeon’s concern was a legitimate one—that additional attempts at removal could lead to complications far worse than having a small segment of a needle left in place. After all, shrapnel, bullets, etc, remain lodged in various locations throughout the body without subsequent ill effects. He did discuss with the patient the fact that a needle segment was left in the muscle wall. But how do you assess postoperative pelvic pain in a patient who had preoperative chronic pelvic pain? These are questions we as clinicians ask. Clearly, there are no black-and-white answers, and we will call upon our legal consultants for their expertise in addressing these queries.
From the gynecologic perspective, however, it is of paramount importance to address the patient’s postoperative vaginal pain and determine the best management approach. In this case the TOT, and its association with a 21.5% complication rate, including reported vaginal extrusion, introduces a whole new set of concerns.1 The TOT use in itself raises the question of liability on the part of the surgeon. This mesh has more than 150 associated complications, including obturator nerve injuries, extensive blood loss, and ischiorectal fossa abscesses.2 Once a device comes upon the radar screen of the US Food and Drug Administration for significant complications, where does that leave the clinician in regard to litigation? Let’s look to our legal colleagues for their insight and expertise.
Legal considerations
Given the facts in this case, it is not surprising that it resulted in a defense verdict. The majority of cases filed are ultimately disposed of in favor of the medical defendants, and the majority of medical malpractice cases that go to trial result in defense verdicts.
Medical malpractice, or “professional negligence,” consists of a claim that a medical professional had a duty of care to the patient, a breach of that duty, injury to the patient, and a causal connection (“causation”) between the breach of duty and the injury. It is the obligation of the plaintiff to prove the elements of negligence by a preponderance of the evidence.
Were the surgeon’s actions in line with other surgeons’ expected actions? The issue of the breach of the duty of care essentially is the question of whether the physician acted similarly to a reasonably careful practitioner of the same specialty under the same circumstances. Doctors are not held to a standard of perfection. That is, not every injury or bad outcome is negligence—only those injuries that result from actions, or inactions, that were not within the level of care acceptable in the profession.
Why would this patient file a lawsuit? The injury was not trivial (it had both pain and cost associated with it), but it was not catastrophic, and the negligence was going to be difficult to prove. Furthermore, lawsuits are expensive in terms of time, energy, and emotional commitment—few people file them for the fun of it. We can only speculate on the answer to the question but, frequently, such claims are a search for the answer to “What happened, and why?” or a reaction to feeling ignored or disrespected. There is little in the case facts that we have to work with to indicate what the communication was between the gynecologist and the patient and her family. The statement of facts, however, leaves the impression that communication deteriorated as the postoperative pain endured.
Some additional areas of potential claims for liability in this case include:
- The explanation for the needle breaking during surgery is unclear from the brief statement of case facts. There might be malpractice liability if the surgeon was unreasonable in how the needle was used, used the wrong needle, or ignored defects in the needle.
- The surgeon tried unsuccessfully to retrieve the needle during the original surgery. If the surgeon’s failure to retrieve the needle was because of inadequate training, lack of care or the like, it might be seen as the “cause” of the patient’s injuries.
- The fact that a second surgeon was able to remove the needle tip, which resolved the patient’s pain, may raise the question of whether the first surgeon’s decision not to seek to remove it in response to the continuing pain was reasonable. If the first surgeon did not want to remove the needle tip, a question might be raised about whether that surgeon should have referred the patient to another surgeon. (The patient ultimately found another surgeon on her own.)
- Regarding use of TOT: A 21.5% complication rate ordinarily would be a significant factor to consider in a decision to use the tape. Physicians are responsible for keeping up with current developments in the devices and pharmaceuticals they use. Therefore, if information on the complication rate was available, the surgeon’s documentation should reflect the basis for choosing to use the tape. More important, the surgeon should document a conversation with the patient about the risks and benefits of using the TOT and the discussion of alternatives to its use.
What factors could have tipped the case toward the defense?
The defense verdict indicates that the jury determined there was no negligence, or that the patient could not prove any of these potential bases of liability. As noted above, what may have helped the defense is the fact that the surgeon documented the details of the informed consent conversation, including that “discussion was carried out regarding” the tape. The informed consent process is an important opportunity for communication with the patient, and a chance to make sure that expectations are reasonable. Liability for the failure of informed consent is not common. When something has gone wrong, however, it can matter whether the problem was something mentioned in the informed consent process. In addition, it was positive that postoperatively the patient was informed of the broken needle—although it is not clear who informed her about it.
A couple of other legal issues are worth noting. From our fact scenario we do not know what was documented in the incident report filed by the circulating nurse and reviewed by the surgical committee. We also do not know whether the plaintiff was privy to the incident report document. The surgical committee is likely a peer-review committee, and most states provide some privilege for such committees (to avoid disclosure of committee information for discovery or at trial). The deliberations and conclusions of the committee, therefore, were likely privileged. However, incident reports are frequently used for other purposes, such as administrative reports, that are not privileged—so the incident report often is determined to be discoverable depending on the interpretation of the state’s law.
No winner in this case
Despite the defense verdict, the physician was not really the “winner” after having spent a great deal of time, energy, money, and emotion defending this suit. Ultimately, the goal is not to win malpractice cases but to avoid them—in this case, among other things, by being frank with patients about expectations, keeping an open line of communication with patients when they are concerned with an outcome that is less than ideal, and referring a patient when it may be appropriate.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
1. Bladder sling risks, complications and side effects. DrugWatch Web site. http://www.drugwatch.com/trans vaginal-mesh/bladder-sling/. Updated January 2, 2015. Accessed February 13, 2015.
2. Boyles SH, Edwards R, Gregory W, Clark A. Complications associated with transobturator sling procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(1):19–22.
1. Bladder sling risks, complications and side effects. DrugWatch Web site. http://www.drugwatch.com/trans vaginal-mesh/bladder-sling/. Updated January 2, 2015. Accessed February 13, 2015.
2. Boyles SH, Edwards R, Gregory W, Clark A. Complications associated with transobturator sling procedures. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(1):19–22.
Vicarious liability. Second of 2 parts: When a colleague is out of line
Last month, we began consideration of the obligations of physicians and health-care organizations to take action concerning colleagues who are out of line. In part 1, we looked at a recently reported case of “The gynecologist who wore an unusual pen.” He admitted taking more than 1,000 videos and images of patients using a tiny camera embedded in a pen or key fob that he wore around his neck. This serious misconduct continued for many years without being noticed.
A class-action lawsuit against the medical center and physician resulted in a settlement of $190 million, despite the fact that the physician had not transferred the images to others. Here, we look at the obligation of the medical profession to notice and manage colleagues who are creating a risk to patients or the institution. What are the legal consequences of your relationships with your colleagues, and why is it so important for physicians and health-care centers to be alert to inappropriate conduct and deal promptly with those problems?
CASE: Well-respected clinician turns increasingly grumpy toward colleagues and patients
In your role as president of the practice, you have been asked to comment on a colleague’s behavior. You’ve known him for a long time. Dr. X has been in practice for more than 20 years, and always has been well respected in the community. Over his career he has served as residency program director for a large community hospital. He has been, in essence, a role model for physicians in training.
Over the past 6 months, a number of complaints have been brought to your attention as practice president. The primary concern is Dr. X’s temper, which he seems to be having trouble controlling. Nurses have stopped you in the hallway to discuss his change in attitude. “What’s with Dr. X?” they ask. “We are noticing a change in the way he handles patients and residents in the program.”
Now, the threat of a lawsuit because of his negative behavior has been brought to your attention.
Vicarious liability
This case scenario is becoming more frequent as time and reimbursement pressures mount. Learning to deal with it all in a meaningful manner can be a challenge.
What “checks and balances” do you have regarding colleagues’ behavior in your practice? Ethics come into play here, as we all hear about the cases, although not typical, of the clinician who has sex with his patient, sexual abuse accusations, and so forth. But there are significant legal issues even in much less extreme cases.
When the clinician is not an employee
In part 1, we discussed how and why an employer is responsible for the actions of its employees. In many circumstances, however, hospitals grant privileges to physicians who are not employees. Suppose the gynecologist in “The case of the unusual pen” had not been an employee of the hospital, but had staff privileges. Would the hospital have been liable?
Typically, a clinician with hospital privileges who is not an employee is an “independent contractor” rather than an “agent” of the hospital. As such, the vicarious liability that is a hallmark of a principal-agent arrangement is absent. However, the hospital still may be responsible for the clinician’s misconduct if that liability arises from the hospital’s own carelessness. For example, suppose the hospital had given privileges to a clinician without adequately reviewing his or her credentials, qualifications, and past conduct. Imagine that this clinician had a history of abusing patients but the hospital had failed to ascertain that fact.
A hospital that unreasonably fails to find information that would have prevented a clinician from being given privileges or that would have resulted in the limitation or removal of privileges may be liable for the harm done by the clinician, even when that person is an independent contractor. Furthermore, the failure to observe and assess the professional practice of the independent contractor may result in liability to the hospital.
Review process for hospital privileges. The National Practitioner Data Bank (NPDB) was developed to help hospitals find information about physicians who have been disciplined or had malpractice problems. A query to the NPDB may not be sufficient to discover all relevant information, however. Indeed, the NPDB itself notes that “the information from the Data Bank should be used in conjunction with, not in replacement of, information from other sources.”1 Most institutions have standard protocols for performing background checks on anyone applying for privileges; those processes must be followed carefully and reviewed on a regular basis.
The appointment procedure is the beginning, not the end, of the review process. An ongoing assessment of performance is formalized in committees in all hospitals. In addition, there are formal reappointment processes to assure continued competency and compliance with hospital standards and regulations.
And all of this is good—but still not enough.
In some cases an apology may be in order when things go wrong with patient care—and sometimes it can help defuse the tensions that arise when a bad outcome happens. For example, in an article titled, “The Last Word: The Power of Apology” a clinician’s thoughts are depicted as follows1:
Where was the right balance between sincere apology and excessive self-blame? How would this patient and the family react? Would they kick me out of the room and open up the yellow pages to find the closest malpractice attorney? Maybe.
The physician came up with a plan, reviewed it one last time right outside the door, took a deep breath and entered the room, “I’m so, so, so, sorry this happened to you.”1
The hour that followed focused on what had happened and what other physicians had told the family when they weighed in. Bottom line? There was agreement that it was a complex and tragic case. As the doctor exited, the family inquired, “You’ll still be our doctor, won’t you? We love you. You are our friend.”1
The tension left his shoulders as the physician reflected on the importance of honesty and humility and apologizing appropriately.1
Saying “I’m sorry” can be a rewarding experience.
References
- Cohen ML. The last word: the power of apology. Fam Pract Manag. 2010;17(1):40–41.
Are you responsible for reporting your colleagues’ behavior?
An important part of a hospital’s or practice’s quality assurance is the day-to-day observations of physicians, nurses, and staff members. Courts have been increasingly insistent that an institution may be liable when its physicians or nurses witness inappropriate medical practice but fail to take action to protect patients. Inappropriate practices include:
- undertaking procedures for which the clinician is not qualified or credentialed
- violating hospital or practice policy or
procedures - causing problems for patients or others.
In “The case of the unusual pen,” the plaintiffs claimed that the institution failed to “discover, stop and report” the physician because its staff was not trained to recognize and report inappropriate conduct. For example, the physician routinely may have performed gynecologic exams without a medial assistant in the room. The hospital described the physician as a “rogue” employee whose actions could not have been discovered, according to the facts we know—but the plaintiffs claimed that the hospital should have known what the physician was doing. Whatever the details of this actual case, the continued, undiscovered misconduct of a physician is, at best, bound to raise questions as to why the hospital or practice did not know about it and take action.
That brings us back to the hypothetical situation that began this article:
CASE: Next steps to confront the issue
In your role as president of the practice, you are asked to comment on a colleague’s questionable behavior.
Do you issue a statement regarding that behavior and let the matter ride, or is more action advisable?
From a legal standpoint, the suggestion that a clinician’s problem behavior is being brought to the attention of the president of the practice is positive. Identifying the problem is only the first step, however. Being asked to comment on the colleague will not be enough. Your responsibility to the practice has now been triggered and you must undertake appropriate procedures. Summarily (and inappropriately) dismissing the colleague may result in all kinds of problems, not to mention a lawsuit. Yet just observing the situation for a few months carries other legal risks. The practice or institution undoubtedly has a standard set of procedures, and you immediately should begin implementing them. These procedures usually involve informal steps—investigating the situation and giving the physician the opportunity to respond.
When the matter is outside of routine, as this case may be, we believe that it is worthwhile to consult a legal expert. Beyond the duty to patients, there are likely to be contractual obligations and complex business law issues. Ideally, the practice has an ongoing relationship with an attorney who is an expert in health matters. Knowing your practice, the attorney can be invaluable in helping you avoid problems and find a resolution to the problems that arise, and he or she should provide consultation if the matter requires formal processes.
These obligations are supported by sound legal principles. It is always important to remember that the purpose of these obligations is to avoid unnecessary harm, stress, and expense to patients who are putting their trust in your practice.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. US Department of Health and Human Services, Health Resources and Services Administration. The National Practitioner Data Bank: about us. HRSA Web site. http://www.npdb.hrsa.gov/topNavigation/aboutUs.jsp. Accessed December 11, 2014.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |


Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
Last month, we began consideration of the obligations of physicians and health-care organizations to take action concerning colleagues who are out of line. In part 1, we looked at a recently reported case of “The gynecologist who wore an unusual pen.” He admitted taking more than 1,000 videos and images of patients using a tiny camera embedded in a pen or key fob that he wore around his neck. This serious misconduct continued for many years without being noticed.
A class-action lawsuit against the medical center and physician resulted in a settlement of $190 million, despite the fact that the physician had not transferred the images to others. Here, we look at the obligation of the medical profession to notice and manage colleagues who are creating a risk to patients or the institution. What are the legal consequences of your relationships with your colleagues, and why is it so important for physicians and health-care centers to be alert to inappropriate conduct and deal promptly with those problems?
CASE: Well-respected clinician turns increasingly grumpy toward colleagues and patients
In your role as president of the practice, you have been asked to comment on a colleague’s behavior. You’ve known him for a long time. Dr. X has been in practice for more than 20 years, and always has been well respected in the community. Over his career he has served as residency program director for a large community hospital. He has been, in essence, a role model for physicians in training.
Over the past 6 months, a number of complaints have been brought to your attention as practice president. The primary concern is Dr. X’s temper, which he seems to be having trouble controlling. Nurses have stopped you in the hallway to discuss his change in attitude. “What’s with Dr. X?” they ask. “We are noticing a change in the way he handles patients and residents in the program.”
Now, the threat of a lawsuit because of his negative behavior has been brought to your attention.
Vicarious liability
This case scenario is becoming more frequent as time and reimbursement pressures mount. Learning to deal with it all in a meaningful manner can be a challenge.
What “checks and balances” do you have regarding colleagues’ behavior in your practice? Ethics come into play here, as we all hear about the cases, although not typical, of the clinician who has sex with his patient, sexual abuse accusations, and so forth. But there are significant legal issues even in much less extreme cases.
When the clinician is not an employee
In part 1, we discussed how and why an employer is responsible for the actions of its employees. In many circumstances, however, hospitals grant privileges to physicians who are not employees. Suppose the gynecologist in “The case of the unusual pen” had not been an employee of the hospital, but had staff privileges. Would the hospital have been liable?
Typically, a clinician with hospital privileges who is not an employee is an “independent contractor” rather than an “agent” of the hospital. As such, the vicarious liability that is a hallmark of a principal-agent arrangement is absent. However, the hospital still may be responsible for the clinician’s misconduct if that liability arises from the hospital’s own carelessness. For example, suppose the hospital had given privileges to a clinician without adequately reviewing his or her credentials, qualifications, and past conduct. Imagine that this clinician had a history of abusing patients but the hospital had failed to ascertain that fact.
A hospital that unreasonably fails to find information that would have prevented a clinician from being given privileges or that would have resulted in the limitation or removal of privileges may be liable for the harm done by the clinician, even when that person is an independent contractor. Furthermore, the failure to observe and assess the professional practice of the independent contractor may result in liability to the hospital.
Review process for hospital privileges. The National Practitioner Data Bank (NPDB) was developed to help hospitals find information about physicians who have been disciplined or had malpractice problems. A query to the NPDB may not be sufficient to discover all relevant information, however. Indeed, the NPDB itself notes that “the information from the Data Bank should be used in conjunction with, not in replacement of, information from other sources.”1 Most institutions have standard protocols for performing background checks on anyone applying for privileges; those processes must be followed carefully and reviewed on a regular basis.
The appointment procedure is the beginning, not the end, of the review process. An ongoing assessment of performance is formalized in committees in all hospitals. In addition, there are formal reappointment processes to assure continued competency and compliance with hospital standards and regulations.
And all of this is good—but still not enough.
In some cases an apology may be in order when things go wrong with patient care—and sometimes it can help defuse the tensions that arise when a bad outcome happens. For example, in an article titled, “The Last Word: The Power of Apology” a clinician’s thoughts are depicted as follows1:
Where was the right balance between sincere apology and excessive self-blame? How would this patient and the family react? Would they kick me out of the room and open up the yellow pages to find the closest malpractice attorney? Maybe.
The physician came up with a plan, reviewed it one last time right outside the door, took a deep breath and entered the room, “I’m so, so, so, sorry this happened to you.”1
The hour that followed focused on what had happened and what other physicians had told the family when they weighed in. Bottom line? There was agreement that it was a complex and tragic case. As the doctor exited, the family inquired, “You’ll still be our doctor, won’t you? We love you. You are our friend.”1
The tension left his shoulders as the physician reflected on the importance of honesty and humility and apologizing appropriately.1
Saying “I’m sorry” can be a rewarding experience.
References
- Cohen ML. The last word: the power of apology. Fam Pract Manag. 2010;17(1):40–41.
Are you responsible for reporting your colleagues’ behavior?
An important part of a hospital’s or practice’s quality assurance is the day-to-day observations of physicians, nurses, and staff members. Courts have been increasingly insistent that an institution may be liable when its physicians or nurses witness inappropriate medical practice but fail to take action to protect patients. Inappropriate practices include:
- undertaking procedures for which the clinician is not qualified or credentialed
- violating hospital or practice policy or
procedures - causing problems for patients or others.
In “The case of the unusual pen,” the plaintiffs claimed that the institution failed to “discover, stop and report” the physician because its staff was not trained to recognize and report inappropriate conduct. For example, the physician routinely may have performed gynecologic exams without a medial assistant in the room. The hospital described the physician as a “rogue” employee whose actions could not have been discovered, according to the facts we know—but the plaintiffs claimed that the hospital should have known what the physician was doing. Whatever the details of this actual case, the continued, undiscovered misconduct of a physician is, at best, bound to raise questions as to why the hospital or practice did not know about it and take action.
That brings us back to the hypothetical situation that began this article:
CASE: Next steps to confront the issue
In your role as president of the practice, you are asked to comment on a colleague’s questionable behavior.
Do you issue a statement regarding that behavior and let the matter ride, or is more action advisable?
From a legal standpoint, the suggestion that a clinician’s problem behavior is being brought to the attention of the president of the practice is positive. Identifying the problem is only the first step, however. Being asked to comment on the colleague will not be enough. Your responsibility to the practice has now been triggered and you must undertake appropriate procedures. Summarily (and inappropriately) dismissing the colleague may result in all kinds of problems, not to mention a lawsuit. Yet just observing the situation for a few months carries other legal risks. The practice or institution undoubtedly has a standard set of procedures, and you immediately should begin implementing them. These procedures usually involve informal steps—investigating the situation and giving the physician the opportunity to respond.
When the matter is outside of routine, as this case may be, we believe that it is worthwhile to consult a legal expert. Beyond the duty to patients, there are likely to be contractual obligations and complex business law issues. Ideally, the practice has an ongoing relationship with an attorney who is an expert in health matters. Knowing your practice, the attorney can be invaluable in helping you avoid problems and find a resolution to the problems that arise, and he or she should provide consultation if the matter requires formal processes.
These obligations are supported by sound legal principles. It is always important to remember that the purpose of these obligations is to avoid unnecessary harm, stress, and expense to patients who are putting their trust in your practice.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Last month, we began consideration of the obligations of physicians and health-care organizations to take action concerning colleagues who are out of line. In part 1, we looked at a recently reported case of “The gynecologist who wore an unusual pen.” He admitted taking more than 1,000 videos and images of patients using a tiny camera embedded in a pen or key fob that he wore around his neck. This serious misconduct continued for many years without being noticed.
A class-action lawsuit against the medical center and physician resulted in a settlement of $190 million, despite the fact that the physician had not transferred the images to others. Here, we look at the obligation of the medical profession to notice and manage colleagues who are creating a risk to patients or the institution. What are the legal consequences of your relationships with your colleagues, and why is it so important for physicians and health-care centers to be alert to inappropriate conduct and deal promptly with those problems?
CASE: Well-respected clinician turns increasingly grumpy toward colleagues and patients
In your role as president of the practice, you have been asked to comment on a colleague’s behavior. You’ve known him for a long time. Dr. X has been in practice for more than 20 years, and always has been well respected in the community. Over his career he has served as residency program director for a large community hospital. He has been, in essence, a role model for physicians in training.
Over the past 6 months, a number of complaints have been brought to your attention as practice president. The primary concern is Dr. X’s temper, which he seems to be having trouble controlling. Nurses have stopped you in the hallway to discuss his change in attitude. “What’s with Dr. X?” they ask. “We are noticing a change in the way he handles patients and residents in the program.”
Now, the threat of a lawsuit because of his negative behavior has been brought to your attention.
Vicarious liability
This case scenario is becoming more frequent as time and reimbursement pressures mount. Learning to deal with it all in a meaningful manner can be a challenge.
What “checks and balances” do you have regarding colleagues’ behavior in your practice? Ethics come into play here, as we all hear about the cases, although not typical, of the clinician who has sex with his patient, sexual abuse accusations, and so forth. But there are significant legal issues even in much less extreme cases.
When the clinician is not an employee
In part 1, we discussed how and why an employer is responsible for the actions of its employees. In many circumstances, however, hospitals grant privileges to physicians who are not employees. Suppose the gynecologist in “The case of the unusual pen” had not been an employee of the hospital, but had staff privileges. Would the hospital have been liable?
Typically, a clinician with hospital privileges who is not an employee is an “independent contractor” rather than an “agent” of the hospital. As such, the vicarious liability that is a hallmark of a principal-agent arrangement is absent. However, the hospital still may be responsible for the clinician’s misconduct if that liability arises from the hospital’s own carelessness. For example, suppose the hospital had given privileges to a clinician without adequately reviewing his or her credentials, qualifications, and past conduct. Imagine that this clinician had a history of abusing patients but the hospital had failed to ascertain that fact.
A hospital that unreasonably fails to find information that would have prevented a clinician from being given privileges or that would have resulted in the limitation or removal of privileges may be liable for the harm done by the clinician, even when that person is an independent contractor. Furthermore, the failure to observe and assess the professional practice of the independent contractor may result in liability to the hospital.
Review process for hospital privileges. The National Practitioner Data Bank (NPDB) was developed to help hospitals find information about physicians who have been disciplined or had malpractice problems. A query to the NPDB may not be sufficient to discover all relevant information, however. Indeed, the NPDB itself notes that “the information from the Data Bank should be used in conjunction with, not in replacement of, information from other sources.”1 Most institutions have standard protocols for performing background checks on anyone applying for privileges; those processes must be followed carefully and reviewed on a regular basis.
The appointment procedure is the beginning, not the end, of the review process. An ongoing assessment of performance is formalized in committees in all hospitals. In addition, there are formal reappointment processes to assure continued competency and compliance with hospital standards and regulations.
And all of this is good—but still not enough.
In some cases an apology may be in order when things go wrong with patient care—and sometimes it can help defuse the tensions that arise when a bad outcome happens. For example, in an article titled, “The Last Word: The Power of Apology” a clinician’s thoughts are depicted as follows1:
Where was the right balance between sincere apology and excessive self-blame? How would this patient and the family react? Would they kick me out of the room and open up the yellow pages to find the closest malpractice attorney? Maybe.
The physician came up with a plan, reviewed it one last time right outside the door, took a deep breath and entered the room, “I’m so, so, so, sorry this happened to you.”1
The hour that followed focused on what had happened and what other physicians had told the family when they weighed in. Bottom line? There was agreement that it was a complex and tragic case. As the doctor exited, the family inquired, “You’ll still be our doctor, won’t you? We love you. You are our friend.”1
The tension left his shoulders as the physician reflected on the importance of honesty and humility and apologizing appropriately.1
Saying “I’m sorry” can be a rewarding experience.
References
- Cohen ML. The last word: the power of apology. Fam Pract Manag. 2010;17(1):40–41.
Are you responsible for reporting your colleagues’ behavior?
An important part of a hospital’s or practice’s quality assurance is the day-to-day observations of physicians, nurses, and staff members. Courts have been increasingly insistent that an institution may be liable when its physicians or nurses witness inappropriate medical practice but fail to take action to protect patients. Inappropriate practices include:
- undertaking procedures for which the clinician is not qualified or credentialed
- violating hospital or practice policy or
procedures - causing problems for patients or others.
In “The case of the unusual pen,” the plaintiffs claimed that the institution failed to “discover, stop and report” the physician because its staff was not trained to recognize and report inappropriate conduct. For example, the physician routinely may have performed gynecologic exams without a medial assistant in the room. The hospital described the physician as a “rogue” employee whose actions could not have been discovered, according to the facts we know—but the plaintiffs claimed that the hospital should have known what the physician was doing. Whatever the details of this actual case, the continued, undiscovered misconduct of a physician is, at best, bound to raise questions as to why the hospital or practice did not know about it and take action.
That brings us back to the hypothetical situation that began this article:
CASE: Next steps to confront the issue
In your role as president of the practice, you are asked to comment on a colleague’s questionable behavior.
Do you issue a statement regarding that behavior and let the matter ride, or is more action advisable?
From a legal standpoint, the suggestion that a clinician’s problem behavior is being brought to the attention of the president of the practice is positive. Identifying the problem is only the first step, however. Being asked to comment on the colleague will not be enough. Your responsibility to the practice has now been triggered and you must undertake appropriate procedures. Summarily (and inappropriately) dismissing the colleague may result in all kinds of problems, not to mention a lawsuit. Yet just observing the situation for a few months carries other legal risks. The practice or institution undoubtedly has a standard set of procedures, and you immediately should begin implementing them. These procedures usually involve informal steps—investigating the situation and giving the physician the opportunity to respond.
When the matter is outside of routine, as this case may be, we believe that it is worthwhile to consult a legal expert. Beyond the duty to patients, there are likely to be contractual obligations and complex business law issues. Ideally, the practice has an ongoing relationship with an attorney who is an expert in health matters. Knowing your practice, the attorney can be invaluable in helping you avoid problems and find a resolution to the problems that arise, and he or she should provide consultation if the matter requires formal processes.
These obligations are supported by sound legal principles. It is always important to remember that the purpose of these obligations is to avoid unnecessary harm, stress, and expense to patients who are putting their trust in your practice.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. US Department of Health and Human Services, Health Resources and Services Administration. The National Practitioner Data Bank: about us. HRSA Web site. http://www.npdb.hrsa.gov/topNavigation/aboutUs.jsp. Accessed December 11, 2014.
Reference
1. US Department of Health and Human Services, Health Resources and Services Administration. The National Practitioner Data Bank: about us. HRSA Web site. http://www.npdb.hrsa.gov/topNavigation/aboutUs.jsp. Accessed December 11, 2014.

Vicarious liability. First of 2 Parts: The gynecologist who wore an unusual pen
What obligations do physicians and medical facilities have when it comes to dealing with troubled or troublesome clinicians? In this 2-part column, we look at a recently reported case of a gynecologist who engaged in serious misconduct without being noticed. In part 2, we will discuss the obligation of the medical profession to notice and deal with colleagues who are creating a risk to patients or the institution.
CASE: Medical center blamed for negligence when rogue physician records pelvic exams
Dr. A, a gynecologist, had been a physician at a leading academic medical center for many years. His employment was terminated in February 2013 when he admitted taking more than 1,000 videos and images using a tiny camera embedded in a pen or key fob that he wore around his neck. He stored the images on his home computer. It seems that he had been secretly recording pelvic examinations since 2005.
A class-action lawsuit initiated against the academic medical center and the physician suggested invasion of privacy, emotional distress, and negligence in oversight on the part of the academic institution. (This case was settled before trial and most of the records are not publicly available. The facts used here are based on press releases and published articles and, therefore, are incomplete and may be subject to interpretation.)
Breach of trust
Talk about a violation of the doctor-patient relationship! The suit claims, among other things, “harmful and offensive sexual contact with patients.” The hospital identified 12,700 patients that the gynecologist might have seen during his 25-year-span as an employee.
Some victims report posttraumatic stress disorder (PTSD). In addition to feeling betrayed by their physician, the victims feel the action was a breach of faith, of trust. They report being fearful of being examined by another physician, and some have refused to seek medical care. The sense of mistrust of the medical profession has resulted in some victims’ reluctance to allow their children to be seen by pediatricians.1
CASE: SETTLED
This lawsuit, possibly the largest medical malpractice case of its kind, resulted in a $190 million settlement. The academic medical center will disperse the funds to more than 7,000 possible victims.1 A special hotline Web site and a toll-free number have been established to facilitate victim reporting. A board-certified psychologist will work with victims.
Similar suits have settled
Other lawsuits involving physicians who have secretly recorded patients also have been settled:
- A Connecticut endocrinologist who took photos of patients nude settled for $50 million in 2012.1
- A pediatrician pedophile in Delaware was associated with a $123-million settlement with long-term follow-up of victims.2
WHAT ARE THE ETHICAL OBLIGATIONS?
Ethics in medicine can be discussed at great length (see “Issues of ethics in medicine”). An important question related to this case concerns the investigators’ obligations to make their findings public with the scenario that the patient/victims are not aware that a crime occurred.3 This is among the issues that will be considered in part 2 of this article that will be published next month. One concern is that publicly identifying the victims may lead to the development of PTSD and its intrinsic consequences. How can one prosecute the perpetrator and yet prevent psychological consequences of the victims?
What do ACOG and the AMA say about sexual misconduct in medicine?
ACOG. The American College of Obstetricians and Gynecologists (ACOG) is explicit about sexual misconduct. Specifically, the physician-patient relationship can be damaged when there is “confusion regarding professional roles and behavior or clear lack of integrity”1 that results in sexual exploitation and harm. ACOG further states that1:
- Mere mutual consent is rejected as a justification for sexual relations with patients because the disparity in power, status, vulnerability, and need make it difficult for a patient to give meaningful consent to sexual contact or sexual relations.
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances. The relevant standard is the potential for misuse of physician power and exploitation of patient emotions derived from the former relationship.
- Education on ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- Physicians have a responsibility to report offending colleagues to disciplinary boards.
The request by either a patient or a physician to have a chaperone present during a physical examination should be accommodated regardless of the physician’s sex. If a chaperone is present during the physical examination, the physician should provide a separate opportunity for private conversation.
The AMA. The American Medical Association’s Council on Ethical and Judicial Affairs developed a report titled “Sexual Misconduct in the Practice of Medicine.” The Council concluded that2:
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances.
- Education on the ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- In the case of sexual misconduct, reporting offending colleagues is especially important.
References
- Committee on Ethics. ACOG Committee Opinion No. 373. Sexual misconduct. http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Ethics/Sexual-Misconduct. Published August 2007. Accessed November 11, 2014.
- McMurray RJ, Clarke OW, Barrasso JA, et al; Council on Ethical and Judicial Affairs. Sexual misconduct in the practice of medicine. JAMA. 1991;266(19):2741–2745. http://jama.jamanetwork.com/article.aspx?articleid=393342&resultClick=3. Accessed November 11, 2014.
UNUSUAL ELEMENTS OF THIS CASE
The case of “The gynecologist who wore an unusual pen” is extraordinary in terms of the financial consequences for the medical center. Indeed, the $190 million class-action settlement is probably a record in cases of this kind. The facts (insofar as we know them, and we certainly do not know them all) are sufficiently unusual to seem more like fiction than reality.
An unusual element of the case is that the images were apparently not shared with others, but retained by the gynecologist. Thus, the $190 million settlement was not for disclosing confidential information, but for the unauthorized and inappropriate act of taking the videos and storing them at home. This case was a violation of professional obligations and clearly unethical and likely illegal. It was not associated with the distribution of images that is so often the hallmark of breach of privacy cases.
Another very unusual condition of this case was that there was no way to identify the victims. The faces of the women were not in the videos, so the subjects of the 1,200 videos and 140 images found on the physician’s home computer could have been any of more than 7,000 patients.1 The distribution of funds, therefore, may encompass all of these former patients, and the size of an individual’s recovery may depend largely on the degree of emotional upset she experiences. The victims will be asked how much time they spent with the physician, whether a nurse was present, whether there was any verbal or sexual abuse, and details about emotional harm they experienced.
VICARIOUS LIABILITY
Why was the medical center responsible?
At first blush it may seem puzzling that the medical center, rather than the gynecologist, was responsible for the damages. In fact, the gynecologist might well have been both criminally and civilly responsible, but sadly, he committed suicide after his wrongdoing was discovered.3
The hospital was civilly responsible. In this instance it appears (again, from our limited facts) that the gynecologist was an employee of the medical center. Employees are generally considered agents of their employers (“principals”). By definition, a principal has the right and obligation to oversee and control the actions of its agents. As such, the principal is generally legally liable for the actions of an employee within the course of employment. Vicarious liability essentially allows someone harmed by an agent to seek compensation from the principal because the principal selected and appointed the agent.
The vicarious responsibility of an agency relationship applies even when the employee is not following the direct instructions of the employer. For example, even if a trucking company tells its employee, “Do not drink at all and do not drive over the speed limit for any reason,” the company can still be liable when an employee becomes drunk or speeds and causes an accident. At some point, however, the employee may so deviate from tasks related to employment that the employee is off on a “lark of his own.” For example, if the driver is supposed to travel from New York City to Buffalo, but instead takes a personal side trip to Baltimore, where the truck hits a pedestrian, that side trip is probably not the responsibility of the employer.
Applying these principles to this case (assuming the physician was an employee of the medical center), the center would generally be legally responsible for the torts (wrongful acts) of the gynecologist. Now you ask, “what about the ‘lark of his own’? Wasn’t taking all those pictures and videos for his own purposes not really part of the job?” (Now you are thinking like a lawyer—that was meant as a compliment.) It is a good question. First, this involved serious misconduct, which was a violation of basic professional ethics. Second, this videotaping was not part of the job the physician was supposed to be doing. Although it may have been for his own benefit, this deviation of good practice was closely related to and entangled with the purpose of his employment. It is perhaps analogous to the truck driver who drank at lunch and then caused the accident. It made sense, therefore, for the medical center to conclude that it would likely be responsible for the actions of this employee, and settle the case.
As a side note, this vicarious liability does not just apply to medical centers. Physicians have agents in their offices (employees: nurses, interns, and even volunteers). Your medical practice is likely responsible for the actions of your staff members via the concept of vicarious liability.
In hospitals, it is common for physicians to have staff privileges without being employees. Would this case have a different result if the physician had staff privileges but was not an employee? Another good question. We are going to look at that in the next installment—and the answer has significant implications for physicians and nurses as well as for medical facilities.
We want to hear from you! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
- Gabriel T. Hospital agrees to pay $190 million over recording of pelvic exams. http://www.nytimes.com/2014/07/22/us/johns-hopkins-settlement-190-million.html?_r=0. Published July 21, 2014. Accessed November 11, 2014.
- Doe v. Bradley, 64 A.3d 379 (Del. Super. Ct. 2012). http://capegazette.villagesoup.com/media/Common/11/3A/735985/bradley-settlement-opinion.pdf. Accessed November 24, 2014.
- Klosterman C. Should unwitting victims be informed of the crime? NY Times Magazine. http://www.nytimes.com/2014/08/17/magazine/should-unwitting-victims-be-informed-of-the-crime.html. Published August 17, 2014. Accessed November 11, 2014.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith reports no financial relationships relevant to this article.
What obligations do physicians and medical facilities have when it comes to dealing with troubled or troublesome clinicians? In this 2-part column, we look at a recently reported case of a gynecologist who engaged in serious misconduct without being noticed. In part 2, we will discuss the obligation of the medical profession to notice and deal with colleagues who are creating a risk to patients or the institution.
CASE: Medical center blamed for negligence when rogue physician records pelvic exams
Dr. A, a gynecologist, had been a physician at a leading academic medical center for many years. His employment was terminated in February 2013 when he admitted taking more than 1,000 videos and images using a tiny camera embedded in a pen or key fob that he wore around his neck. He stored the images on his home computer. It seems that he had been secretly recording pelvic examinations since 2005.
A class-action lawsuit initiated against the academic medical center and the physician suggested invasion of privacy, emotional distress, and negligence in oversight on the part of the academic institution. (This case was settled before trial and most of the records are not publicly available. The facts used here are based on press releases and published articles and, therefore, are incomplete and may be subject to interpretation.)
Breach of trust
Talk about a violation of the doctor-patient relationship! The suit claims, among other things, “harmful and offensive sexual contact with patients.” The hospital identified 12,700 patients that the gynecologist might have seen during his 25-year-span as an employee.
Some victims report posttraumatic stress disorder (PTSD). In addition to feeling betrayed by their physician, the victims feel the action was a breach of faith, of trust. They report being fearful of being examined by another physician, and some have refused to seek medical care. The sense of mistrust of the medical profession has resulted in some victims’ reluctance to allow their children to be seen by pediatricians.1
CASE: SETTLED
This lawsuit, possibly the largest medical malpractice case of its kind, resulted in a $190 million settlement. The academic medical center will disperse the funds to more than 7,000 possible victims.1 A special hotline Web site and a toll-free number have been established to facilitate victim reporting. A board-certified psychologist will work with victims.
Similar suits have settled
Other lawsuits involving physicians who have secretly recorded patients also have been settled:
- A Connecticut endocrinologist who took photos of patients nude settled for $50 million in 2012.1
- A pediatrician pedophile in Delaware was associated with a $123-million settlement with long-term follow-up of victims.2
WHAT ARE THE ETHICAL OBLIGATIONS?
Ethics in medicine can be discussed at great length (see “Issues of ethics in medicine”). An important question related to this case concerns the investigators’ obligations to make their findings public with the scenario that the patient/victims are not aware that a crime occurred.3 This is among the issues that will be considered in part 2 of this article that will be published next month. One concern is that publicly identifying the victims may lead to the development of PTSD and its intrinsic consequences. How can one prosecute the perpetrator and yet prevent psychological consequences of the victims?
What do ACOG and the AMA say about sexual misconduct in medicine?
ACOG. The American College of Obstetricians and Gynecologists (ACOG) is explicit about sexual misconduct. Specifically, the physician-patient relationship can be damaged when there is “confusion regarding professional roles and behavior or clear lack of integrity”1 that results in sexual exploitation and harm. ACOG further states that1:
- Mere mutual consent is rejected as a justification for sexual relations with patients because the disparity in power, status, vulnerability, and need make it difficult for a patient to give meaningful consent to sexual contact or sexual relations.
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances. The relevant standard is the potential for misuse of physician power and exploitation of patient emotions derived from the former relationship.
- Education on ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- Physicians have a responsibility to report offending colleagues to disciplinary boards.
The request by either a patient or a physician to have a chaperone present during a physical examination should be accommodated regardless of the physician’s sex. If a chaperone is present during the physical examination, the physician should provide a separate opportunity for private conversation.
The AMA. The American Medical Association’s Council on Ethical and Judicial Affairs developed a report titled “Sexual Misconduct in the Practice of Medicine.” The Council concluded that2:
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances.
- Education on the ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- In the case of sexual misconduct, reporting offending colleagues is especially important.
References
- Committee on Ethics. ACOG Committee Opinion No. 373. Sexual misconduct. http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Ethics/Sexual-Misconduct. Published August 2007. Accessed November 11, 2014.
- McMurray RJ, Clarke OW, Barrasso JA, et al; Council on Ethical and Judicial Affairs. Sexual misconduct in the practice of medicine. JAMA. 1991;266(19):2741–2745. http://jama.jamanetwork.com/article.aspx?articleid=393342&resultClick=3. Accessed November 11, 2014.
UNUSUAL ELEMENTS OF THIS CASE
The case of “The gynecologist who wore an unusual pen” is extraordinary in terms of the financial consequences for the medical center. Indeed, the $190 million class-action settlement is probably a record in cases of this kind. The facts (insofar as we know them, and we certainly do not know them all) are sufficiently unusual to seem more like fiction than reality.
An unusual element of the case is that the images were apparently not shared with others, but retained by the gynecologist. Thus, the $190 million settlement was not for disclosing confidential information, but for the unauthorized and inappropriate act of taking the videos and storing them at home. This case was a violation of professional obligations and clearly unethical and likely illegal. It was not associated with the distribution of images that is so often the hallmark of breach of privacy cases.
Another very unusual condition of this case was that there was no way to identify the victims. The faces of the women were not in the videos, so the subjects of the 1,200 videos and 140 images found on the physician’s home computer could have been any of more than 7,000 patients.1 The distribution of funds, therefore, may encompass all of these former patients, and the size of an individual’s recovery may depend largely on the degree of emotional upset she experiences. The victims will be asked how much time they spent with the physician, whether a nurse was present, whether there was any verbal or sexual abuse, and details about emotional harm they experienced.
VICARIOUS LIABILITY
Why was the medical center responsible?
At first blush it may seem puzzling that the medical center, rather than the gynecologist, was responsible for the damages. In fact, the gynecologist might well have been both criminally and civilly responsible, but sadly, he committed suicide after his wrongdoing was discovered.3
The hospital was civilly responsible. In this instance it appears (again, from our limited facts) that the gynecologist was an employee of the medical center. Employees are generally considered agents of their employers (“principals”). By definition, a principal has the right and obligation to oversee and control the actions of its agents. As such, the principal is generally legally liable for the actions of an employee within the course of employment. Vicarious liability essentially allows someone harmed by an agent to seek compensation from the principal because the principal selected and appointed the agent.
The vicarious responsibility of an agency relationship applies even when the employee is not following the direct instructions of the employer. For example, even if a trucking company tells its employee, “Do not drink at all and do not drive over the speed limit for any reason,” the company can still be liable when an employee becomes drunk or speeds and causes an accident. At some point, however, the employee may so deviate from tasks related to employment that the employee is off on a “lark of his own.” For example, if the driver is supposed to travel from New York City to Buffalo, but instead takes a personal side trip to Baltimore, where the truck hits a pedestrian, that side trip is probably not the responsibility of the employer.
Applying these principles to this case (assuming the physician was an employee of the medical center), the center would generally be legally responsible for the torts (wrongful acts) of the gynecologist. Now you ask, “what about the ‘lark of his own’? Wasn’t taking all those pictures and videos for his own purposes not really part of the job?” (Now you are thinking like a lawyer—that was meant as a compliment.) It is a good question. First, this involved serious misconduct, which was a violation of basic professional ethics. Second, this videotaping was not part of the job the physician was supposed to be doing. Although it may have been for his own benefit, this deviation of good practice was closely related to and entangled with the purpose of his employment. It is perhaps analogous to the truck driver who drank at lunch and then caused the accident. It made sense, therefore, for the medical center to conclude that it would likely be responsible for the actions of this employee, and settle the case.
As a side note, this vicarious liability does not just apply to medical centers. Physicians have agents in their offices (employees: nurses, interns, and even volunteers). Your medical practice is likely responsible for the actions of your staff members via the concept of vicarious liability.
In hospitals, it is common for physicians to have staff privileges without being employees. Would this case have a different result if the physician had staff privileges but was not an employee? Another good question. We are going to look at that in the next installment—and the answer has significant implications for physicians and nurses as well as for medical facilities.
We want to hear from you! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
What obligations do physicians and medical facilities have when it comes to dealing with troubled or troublesome clinicians? In this 2-part column, we look at a recently reported case of a gynecologist who engaged in serious misconduct without being noticed. In part 2, we will discuss the obligation of the medical profession to notice and deal with colleagues who are creating a risk to patients or the institution.
CASE: Medical center blamed for negligence when rogue physician records pelvic exams
Dr. A, a gynecologist, had been a physician at a leading academic medical center for many years. His employment was terminated in February 2013 when he admitted taking more than 1,000 videos and images using a tiny camera embedded in a pen or key fob that he wore around his neck. He stored the images on his home computer. It seems that he had been secretly recording pelvic examinations since 2005.
A class-action lawsuit initiated against the academic medical center and the physician suggested invasion of privacy, emotional distress, and negligence in oversight on the part of the academic institution. (This case was settled before trial and most of the records are not publicly available. The facts used here are based on press releases and published articles and, therefore, are incomplete and may be subject to interpretation.)
Breach of trust
Talk about a violation of the doctor-patient relationship! The suit claims, among other things, “harmful and offensive sexual contact with patients.” The hospital identified 12,700 patients that the gynecologist might have seen during his 25-year-span as an employee.
Some victims report posttraumatic stress disorder (PTSD). In addition to feeling betrayed by their physician, the victims feel the action was a breach of faith, of trust. They report being fearful of being examined by another physician, and some have refused to seek medical care. The sense of mistrust of the medical profession has resulted in some victims’ reluctance to allow their children to be seen by pediatricians.1
CASE: SETTLED
This lawsuit, possibly the largest medical malpractice case of its kind, resulted in a $190 million settlement. The academic medical center will disperse the funds to more than 7,000 possible victims.1 A special hotline Web site and a toll-free number have been established to facilitate victim reporting. A board-certified psychologist will work with victims.
Similar suits have settled
Other lawsuits involving physicians who have secretly recorded patients also have been settled:
- A Connecticut endocrinologist who took photos of patients nude settled for $50 million in 2012.1
- A pediatrician pedophile in Delaware was associated with a $123-million settlement with long-term follow-up of victims.2
WHAT ARE THE ETHICAL OBLIGATIONS?
Ethics in medicine can be discussed at great length (see “Issues of ethics in medicine”). An important question related to this case concerns the investigators’ obligations to make their findings public with the scenario that the patient/victims are not aware that a crime occurred.3 This is among the issues that will be considered in part 2 of this article that will be published next month. One concern is that publicly identifying the victims may lead to the development of PTSD and its intrinsic consequences. How can one prosecute the perpetrator and yet prevent psychological consequences of the victims?
What do ACOG and the AMA say about sexual misconduct in medicine?
ACOG. The American College of Obstetricians and Gynecologists (ACOG) is explicit about sexual misconduct. Specifically, the physician-patient relationship can be damaged when there is “confusion regarding professional roles and behavior or clear lack of integrity”1 that results in sexual exploitation and harm. ACOG further states that1:
- Mere mutual consent is rejected as a justification for sexual relations with patients because the disparity in power, status, vulnerability, and need make it difficult for a patient to give meaningful consent to sexual contact or sexual relations.
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances. The relevant standard is the potential for misuse of physician power and exploitation of patient emotions derived from the former relationship.
- Education on ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- Physicians have a responsibility to report offending colleagues to disciplinary boards.
The request by either a patient or a physician to have a chaperone present during a physical examination should be accommodated regardless of the physician’s sex. If a chaperone is present during the physical examination, the physician should provide a separate opportunity for private conversation.
The AMA. The American Medical Association’s Council on Ethical and Judicial Affairs developed a report titled “Sexual Misconduct in the Practice of Medicine.” The Council concluded that2:
- Sexual contact or a romantic relationship concurrent with the physician-patient relationship is unethical.
- Sexual contact or a romantic relationship with a former patient may be unethical under certain circumstances.
- Education on the ethical issues involved in sexual misconduct should be included throughout all levels of medical training.
- In the case of sexual misconduct, reporting offending colleagues is especially important.
References
- Committee on Ethics. ACOG Committee Opinion No. 373. Sexual misconduct. http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Ethics/Sexual-Misconduct. Published August 2007. Accessed November 11, 2014.
- McMurray RJ, Clarke OW, Barrasso JA, et al; Council on Ethical and Judicial Affairs. Sexual misconduct in the practice of medicine. JAMA. 1991;266(19):2741–2745. http://jama.jamanetwork.com/article.aspx?articleid=393342&resultClick=3. Accessed November 11, 2014.
UNUSUAL ELEMENTS OF THIS CASE
The case of “The gynecologist who wore an unusual pen” is extraordinary in terms of the financial consequences for the medical center. Indeed, the $190 million class-action settlement is probably a record in cases of this kind. The facts (insofar as we know them, and we certainly do not know them all) are sufficiently unusual to seem more like fiction than reality.
An unusual element of the case is that the images were apparently not shared with others, but retained by the gynecologist. Thus, the $190 million settlement was not for disclosing confidential information, but for the unauthorized and inappropriate act of taking the videos and storing them at home. This case was a violation of professional obligations and clearly unethical and likely illegal. It was not associated with the distribution of images that is so often the hallmark of breach of privacy cases.
Another very unusual condition of this case was that there was no way to identify the victims. The faces of the women were not in the videos, so the subjects of the 1,200 videos and 140 images found on the physician’s home computer could have been any of more than 7,000 patients.1 The distribution of funds, therefore, may encompass all of these former patients, and the size of an individual’s recovery may depend largely on the degree of emotional upset she experiences. The victims will be asked how much time they spent with the physician, whether a nurse was present, whether there was any verbal or sexual abuse, and details about emotional harm they experienced.
VICARIOUS LIABILITY
Why was the medical center responsible?
At first blush it may seem puzzling that the medical center, rather than the gynecologist, was responsible for the damages. In fact, the gynecologist might well have been both criminally and civilly responsible, but sadly, he committed suicide after his wrongdoing was discovered.3
The hospital was civilly responsible. In this instance it appears (again, from our limited facts) that the gynecologist was an employee of the medical center. Employees are generally considered agents of their employers (“principals”). By definition, a principal has the right and obligation to oversee and control the actions of its agents. As such, the principal is generally legally liable for the actions of an employee within the course of employment. Vicarious liability essentially allows someone harmed by an agent to seek compensation from the principal because the principal selected and appointed the agent.
The vicarious responsibility of an agency relationship applies even when the employee is not following the direct instructions of the employer. For example, even if a trucking company tells its employee, “Do not drink at all and do not drive over the speed limit for any reason,” the company can still be liable when an employee becomes drunk or speeds and causes an accident. At some point, however, the employee may so deviate from tasks related to employment that the employee is off on a “lark of his own.” For example, if the driver is supposed to travel from New York City to Buffalo, but instead takes a personal side trip to Baltimore, where the truck hits a pedestrian, that side trip is probably not the responsibility of the employer.
Applying these principles to this case (assuming the physician was an employee of the medical center), the center would generally be legally responsible for the torts (wrongful acts) of the gynecologist. Now you ask, “what about the ‘lark of his own’? Wasn’t taking all those pictures and videos for his own purposes not really part of the job?” (Now you are thinking like a lawyer—that was meant as a compliment.) It is a good question. First, this involved serious misconduct, which was a violation of basic professional ethics. Second, this videotaping was not part of the job the physician was supposed to be doing. Although it may have been for his own benefit, this deviation of good practice was closely related to and entangled with the purpose of his employment. It is perhaps analogous to the truck driver who drank at lunch and then caused the accident. It made sense, therefore, for the medical center to conclude that it would likely be responsible for the actions of this employee, and settle the case.
As a side note, this vicarious liability does not just apply to medical centers. Physicians have agents in their offices (employees: nurses, interns, and even volunteers). Your medical practice is likely responsible for the actions of your staff members via the concept of vicarious liability.
In hospitals, it is common for physicians to have staff privileges without being employees. Would this case have a different result if the physician had staff privileges but was not an employee? Another good question. We are going to look at that in the next installment—and the answer has significant implications for physicians and nurses as well as for medical facilities.
We want to hear from you! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
- Gabriel T. Hospital agrees to pay $190 million over recording of pelvic exams. http://www.nytimes.com/2014/07/22/us/johns-hopkins-settlement-190-million.html?_r=0. Published July 21, 2014. Accessed November 11, 2014.
- Doe v. Bradley, 64 A.3d 379 (Del. Super. Ct. 2012). http://capegazette.villagesoup.com/media/Common/11/3A/735985/bradley-settlement-opinion.pdf. Accessed November 24, 2014.
- Klosterman C. Should unwitting victims be informed of the crime? NY Times Magazine. http://www.nytimes.com/2014/08/17/magazine/should-unwitting-victims-be-informed-of-the-crime.html. Published August 17, 2014. Accessed November 11, 2014.
- Gabriel T. Hospital agrees to pay $190 million over recording of pelvic exams. http://www.nytimes.com/2014/07/22/us/johns-hopkins-settlement-190-million.html?_r=0. Published July 21, 2014. Accessed November 11, 2014.
- Doe v. Bradley, 64 A.3d 379 (Del. Super. Ct. 2012). http://capegazette.villagesoup.com/media/Common/11/3A/735985/bradley-settlement-opinion.pdf. Accessed November 24, 2014.
- Klosterman C. Should unwitting victims be informed of the crime? NY Times Magazine. http://www.nytimes.com/2014/08/17/magazine/should-unwitting-victims-be-informed-of-the-crime.html. Published August 17, 2014. Accessed November 11, 2014.
Could thorough documentation have changed the outcome of this trial?
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.
