User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
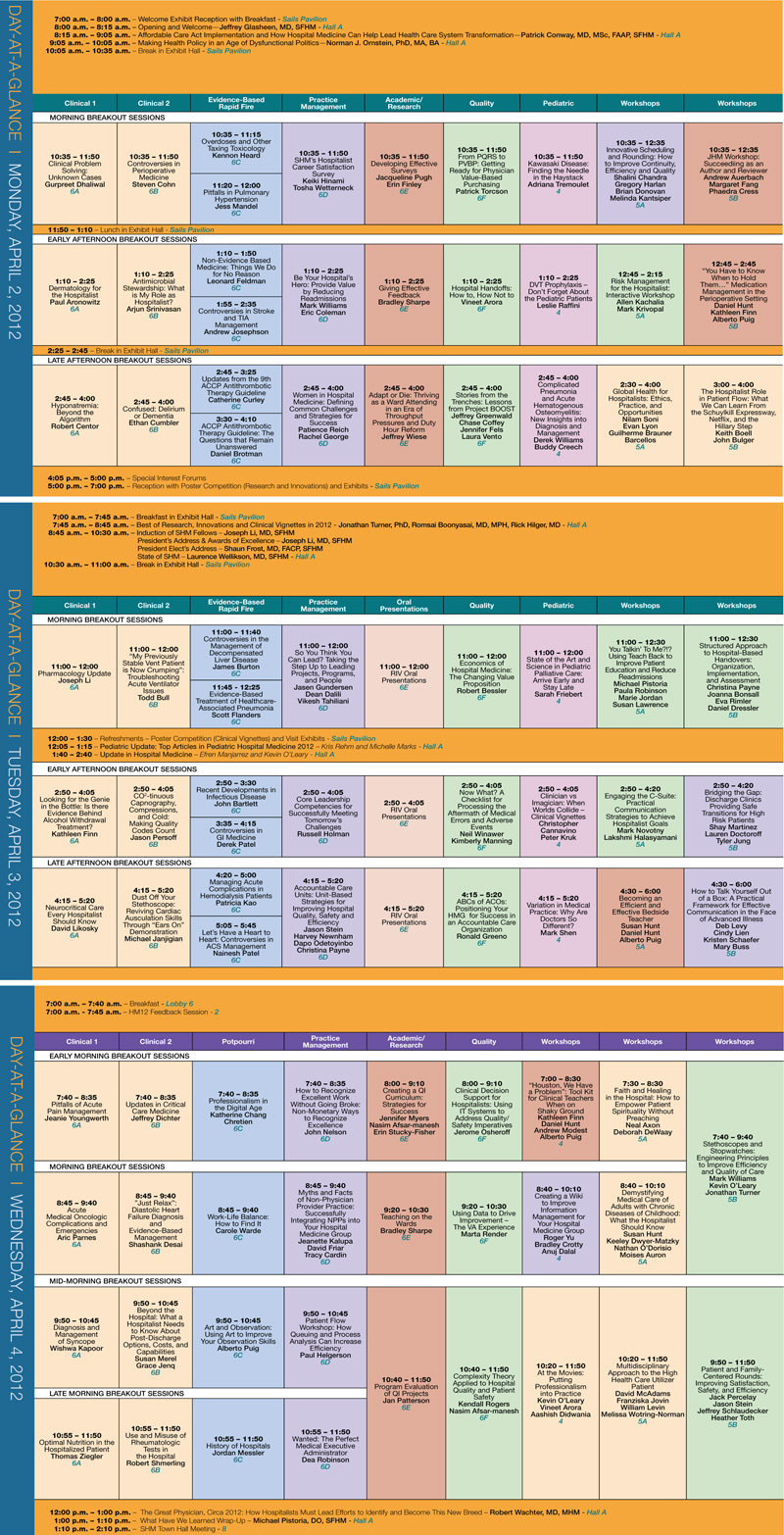
HM12 Features High-Profile Speakers, RIV Sessions, Expanded Breakouts

The world was a different place in 2008, the last time SHM’s annual meeting was in San Diego. Attendance at the yearly confab of hospitalists was almost half of what it is expected to be this year, healthcare reform was still just a bullet point for a presidential candidate’s talking points, and society leaders were drumming up interest in a new fellowship program they’d created.
Now, more than 2,000 hospitalists are expected to fill the San Diego Convention Center April 1-4. Reform isn’t just a political buzzword; it’s the subject of landmark legislation and three plenary addresses—including the requisite convention-ender from HM pioneer Robert Wachter, MD, MHM. And the now-three-tiered fellowship track is more than 1,000 physicians strong.
“Hospitalists really are on the radar of policymakers both inside and outside of our field,” says Jeff Glasheen, MD, SFHM, HM12 course director. “We really have evolved from an insular hospitalist group to the bigger picture that really touches healthcare in many different ways.”
And nowhere is that breadth on display more than the annual meting.
Among the most popular components are the April 1 pre-courses. The schedule features popular sessions on practice management, billing and coding, and ABIM Maintenance of Certification, along with a couple new offerings. The debut class generating the most interest is “How to Improve Performance in CMS’s Value-Based Purchasing Program,” led by SHM senior vice president Joseph Miller and Patrick Torcson, MD, MMM, FAACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee.
Then there is the Research, Innovations, and Clinical Vignettes (RIV) poster competition. So many entries came in for HM12 that the poster sessions have been split up to give attendees more time to interact with their authors. The Research and Innovations poster reception will be from 5 to 7 p.m. April 2. The 90-minute Vignettes session will start at noon April 3.
And, of course, the featured speakers always draw a crowd. This year offers three keynote addresses. First up will be Patrick Conway, MD, MSc, FAAP, SFHM, a pediatric hospitalist and chief medical officer of the Centers for Medicare & Medicaid Services (CMS). His talk is titled “Affordable Care Act Implementation and How Hospital Medicine Can Help Lead Health Care System Transformation.” Political commentator and analyst Norman Ornstein, PhD, MA, BA, will follow with a presentation dubbed “Making Health Policy in an Age of Dysfunctional Politics.” HM12 also continues the tradition of having Dr. Wachter give the last talk, “The Great Physician, Circa 2012: How Hospitalists Must Lead Efforts to Identify and Become This New Breed.”
Throw in a new offering of educational sessions, a new way for attendees to design a thematic schedule of classes that cross different categorical tracks, and a sunny seaside locale, and this year’s meeting would seem destined for success.
“Hopefully the weather will hold up,” says local hospitalist Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego. “My fear is it’s going to be rainy that one week.”
Richard Quinn is a freelance writer in New Jersey.
The world was a different place in 2008, the last time SHM’s annual meeting was in San Diego. Attendance at the yearly confab of hospitalists was almost half of what it is expected to be this year, healthcare reform was still just a bullet point for a presidential candidate’s talking points, and society leaders were drumming up interest in a new fellowship program they’d created.
Now, more than 2,000 hospitalists are expected to fill the San Diego Convention Center April 1-4. Reform isn’t just a political buzzword; it’s the subject of landmark legislation and three plenary addresses—including the requisite convention-ender from HM pioneer Robert Wachter, MD, MHM. And the now-three-tiered fellowship track is more than 1,000 physicians strong.
“Hospitalists really are on the radar of policymakers both inside and outside of our field,” says Jeff Glasheen, MD, SFHM, HM12 course director. “We really have evolved from an insular hospitalist group to the bigger picture that really touches healthcare in many different ways.”
And nowhere is that breadth on display more than the annual meting.
Among the most popular components are the April 1 pre-courses. The schedule features popular sessions on practice management, billing and coding, and ABIM Maintenance of Certification, along with a couple new offerings. The debut class generating the most interest is “How to Improve Performance in CMS’s Value-Based Purchasing Program,” led by SHM senior vice president Joseph Miller and Patrick Torcson, MD, MMM, FAACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee.
Then there is the Research, Innovations, and Clinical Vignettes (RIV) poster competition. So many entries came in for HM12 that the poster sessions have been split up to give attendees more time to interact with their authors. The Research and Innovations poster reception will be from 5 to 7 p.m. April 2. The 90-minute Vignettes session will start at noon April 3.
And, of course, the featured speakers always draw a crowd. This year offers three keynote addresses. First up will be Patrick Conway, MD, MSc, FAAP, SFHM, a pediatric hospitalist and chief medical officer of the Centers for Medicare & Medicaid Services (CMS). His talk is titled “Affordable Care Act Implementation and How Hospital Medicine Can Help Lead Health Care System Transformation.” Political commentator and analyst Norman Ornstein, PhD, MA, BA, will follow with a presentation dubbed “Making Health Policy in an Age of Dysfunctional Politics.” HM12 also continues the tradition of having Dr. Wachter give the last talk, “The Great Physician, Circa 2012: How Hospitalists Must Lead Efforts to Identify and Become This New Breed.”
Throw in a new offering of educational sessions, a new way for attendees to design a thematic schedule of classes that cross different categorical tracks, and a sunny seaside locale, and this year’s meeting would seem destined for success.
“Hopefully the weather will hold up,” says local hospitalist Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego. “My fear is it’s going to be rainy that one week.”
Richard Quinn is a freelance writer in New Jersey.
The world was a different place in 2008, the last time SHM’s annual meeting was in San Diego. Attendance at the yearly confab of hospitalists was almost half of what it is expected to be this year, healthcare reform was still just a bullet point for a presidential candidate’s talking points, and society leaders were drumming up interest in a new fellowship program they’d created.
Now, more than 2,000 hospitalists are expected to fill the San Diego Convention Center April 1-4. Reform isn’t just a political buzzword; it’s the subject of landmark legislation and three plenary addresses—including the requisite convention-ender from HM pioneer Robert Wachter, MD, MHM. And the now-three-tiered fellowship track is more than 1,000 physicians strong.
“Hospitalists really are on the radar of policymakers both inside and outside of our field,” says Jeff Glasheen, MD, SFHM, HM12 course director. “We really have evolved from an insular hospitalist group to the bigger picture that really touches healthcare in many different ways.”
And nowhere is that breadth on display more than the annual meting.
Among the most popular components are the April 1 pre-courses. The schedule features popular sessions on practice management, billing and coding, and ABIM Maintenance of Certification, along with a couple new offerings. The debut class generating the most interest is “How to Improve Performance in CMS’s Value-Based Purchasing Program,” led by SHM senior vice president Joseph Miller and Patrick Torcson, MD, MMM, FAACP, SFHM, chair of SHM’s Performance Measurement and Reporting Committee.
Then there is the Research, Innovations, and Clinical Vignettes (RIV) poster competition. So many entries came in for HM12 that the poster sessions have been split up to give attendees more time to interact with their authors. The Research and Innovations poster reception will be from 5 to 7 p.m. April 2. The 90-minute Vignettes session will start at noon April 3.
And, of course, the featured speakers always draw a crowd. This year offers three keynote addresses. First up will be Patrick Conway, MD, MSc, FAAP, SFHM, a pediatric hospitalist and chief medical officer of the Centers for Medicare & Medicaid Services (CMS). His talk is titled “Affordable Care Act Implementation and How Hospital Medicine Can Help Lead Health Care System Transformation.” Political commentator and analyst Norman Ornstein, PhD, MA, BA, will follow with a presentation dubbed “Making Health Policy in an Age of Dysfunctional Politics.” HM12 also continues the tradition of having Dr. Wachter give the last talk, “The Great Physician, Circa 2012: How Hospitalists Must Lead Efforts to Identify and Become This New Breed.”
Throw in a new offering of educational sessions, a new way for attendees to design a thematic schedule of classes that cross different categorical tracks, and a sunny seaside locale, and this year’s meeting would seem destined for success.
“Hopefully the weather will hold up,” says local hospitalist Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego. “My fear is it’s going to be rainy that one week.”
Richard Quinn is a freelance writer in New Jersey.
Six Keys to a Successful Annual Meeting

Michael Pistoria, DO, FACP, SFHM, is as guilty as you are of not always getting the most out of the annual meeting—and he’s one of the people planning it.
Dr. Pistoria, HM12 assistant course director and hospitalist at Lehigh Valley Health Network in Allentown, Pa., always suggests that if an HM group sends more than one person to the annual meeting, those people should split up and go to as many different sessions as possible. But then, at HM11 in Dallas, an interesting course about an accountable-care unit caught the attention of three people from his office.
“I went, our senior vice president of care continuum went, and the director of our program—we were all there,” Dr. Pistoria says. “I’m thinking, ‘Well this is good, we’re all going to get a slightly different take on it and we’re all going to be listening for different things, and, when we do sit down to compare notes, this is going to be helpful.’ But there were other sessions we could be in.”
To be clear, there is no wrong way to attend an annual meeting. But like knowing which nurse shepherds a smoother discharge, there’s always a way to do it better. Tips from Dr. Pistoria and HM12 course director Jeff Glasheen, MD, SFHM, include:

—Jeff Glasheen, MD, SFHM, HM12 course director
- Prepare. Set up at least a basic schedule or pick out a few sessions to sit in on before arriving at HM12, or you risk trying to build a successful meeting on the fly. “I would treat this much like you would your first semester of college,” Dr. Glasheen says. “You wouldn’t just show up and see what course you wanted to go to. You’d spend some time prior to showing up....If you don’t have a game plan, you’re going to end up missing out on something you want to learn.”
- Go where you friends don’t. As Dr. Pistoria attests, it’s a natural tendency to want to attend sessions with colleagues and critique together. However, this is a once-a-year opportunity. Attend different sessions and compare notes.
- Attend the keynote addresses. This year’s lineup features a national election analyst for “CBS News,” the chief medical officer of the Centers for Medicare & Medicaid Services (CMS), and the incoming chair of the American Board of Internal Medicine (ABIM). Between them, there probably are a few good nuggets to glean.
- Attend the special-interest forums. SHM holds a series of small-group sessions focused on such hyperlocal topics as rural HM and health information technology (HIT), among others. Society staff and leadership take notes and let attendees drive the conversation.
- Network, network, network. Everyone had that first meeting where they didn’t know who was who, so feel free to introduce yourself to anybody. Get business cards from everybody. And hit the hotel hotspots armed with questions and a willingness to buy a potential new relationship a drink.
- “There’s a tremendous willingness to help new people, to answer questions, to have the hallway questions, the conversations that occur at 11 o’clock at night at the bar,” Dr. Pistoria says. “If you see somebody and you say, ‘Hey, you know, I was in your session earlier, can I ask you a couple of follow-up questions?’ People are going to say, ‘Hell yes, sit down. Let’s talk.’ If people remember that and aren’t shy, I think people really can maximize the potential benefit.”
- Share what you learn. Start a quality initiative or talk with your C-suite about starting a project. Email some of your new contacts to start a dialogue. Don’t go home, give one brown-bag session to your colleagues, and wait until next year’s annual meeting to think about the “big picture” again.
“It’s easy to get back home and fall right back into the patterns you were doing before,” Dr. Glasheen says. “If you get excited by something at the annual meeting, go back home and really work at putting that into place.”
Richard Quinn is a freelance writer in New Jersey.
To get involved, visit www.hospitalmedicine2012.org/schedule
Michael Pistoria, DO, FACP, SFHM, is as guilty as you are of not always getting the most out of the annual meeting—and he’s one of the people planning it.
Dr. Pistoria, HM12 assistant course director and hospitalist at Lehigh Valley Health Network in Allentown, Pa., always suggests that if an HM group sends more than one person to the annual meeting, those people should split up and go to as many different sessions as possible. But then, at HM11 in Dallas, an interesting course about an accountable-care unit caught the attention of three people from his office.
“I went, our senior vice president of care continuum went, and the director of our program—we were all there,” Dr. Pistoria says. “I’m thinking, ‘Well this is good, we’re all going to get a slightly different take on it and we’re all going to be listening for different things, and, when we do sit down to compare notes, this is going to be helpful.’ But there were other sessions we could be in.”
To be clear, there is no wrong way to attend an annual meeting. But like knowing which nurse shepherds a smoother discharge, there’s always a way to do it better. Tips from Dr. Pistoria and HM12 course director Jeff Glasheen, MD, SFHM, include:
—Jeff Glasheen, MD, SFHM, HM12 course director
- Prepare. Set up at least a basic schedule or pick out a few sessions to sit in on before arriving at HM12, or you risk trying to build a successful meeting on the fly. “I would treat this much like you would your first semester of college,” Dr. Glasheen says. “You wouldn’t just show up and see what course you wanted to go to. You’d spend some time prior to showing up....If you don’t have a game plan, you’re going to end up missing out on something you want to learn.”
- Go where you friends don’t. As Dr. Pistoria attests, it’s a natural tendency to want to attend sessions with colleagues and critique together. However, this is a once-a-year opportunity. Attend different sessions and compare notes.
- Attend the keynote addresses. This year’s lineup features a national election analyst for “CBS News,” the chief medical officer of the Centers for Medicare & Medicaid Services (CMS), and the incoming chair of the American Board of Internal Medicine (ABIM). Between them, there probably are a few good nuggets to glean.
- Attend the special-interest forums. SHM holds a series of small-group sessions focused on such hyperlocal topics as rural HM and health information technology (HIT), among others. Society staff and leadership take notes and let attendees drive the conversation.
- Network, network, network. Everyone had that first meeting where they didn’t know who was who, so feel free to introduce yourself to anybody. Get business cards from everybody. And hit the hotel hotspots armed with questions and a willingness to buy a potential new relationship a drink.
- “There’s a tremendous willingness to help new people, to answer questions, to have the hallway questions, the conversations that occur at 11 o’clock at night at the bar,” Dr. Pistoria says. “If you see somebody and you say, ‘Hey, you know, I was in your session earlier, can I ask you a couple of follow-up questions?’ People are going to say, ‘Hell yes, sit down. Let’s talk.’ If people remember that and aren’t shy, I think people really can maximize the potential benefit.”
- Share what you learn. Start a quality initiative or talk with your C-suite about starting a project. Email some of your new contacts to start a dialogue. Don’t go home, give one brown-bag session to your colleagues, and wait until next year’s annual meeting to think about the “big picture” again.
“It’s easy to get back home and fall right back into the patterns you were doing before,” Dr. Glasheen says. “If you get excited by something at the annual meeting, go back home and really work at putting that into place.”
Richard Quinn is a freelance writer in New Jersey.
To get involved, visit www.hospitalmedicine2012.org/schedule
Michael Pistoria, DO, FACP, SFHM, is as guilty as you are of not always getting the most out of the annual meeting—and he’s one of the people planning it.
Dr. Pistoria, HM12 assistant course director and hospitalist at Lehigh Valley Health Network in Allentown, Pa., always suggests that if an HM group sends more than one person to the annual meeting, those people should split up and go to as many different sessions as possible. But then, at HM11 in Dallas, an interesting course about an accountable-care unit caught the attention of three people from his office.
“I went, our senior vice president of care continuum went, and the director of our program—we were all there,” Dr. Pistoria says. “I’m thinking, ‘Well this is good, we’re all going to get a slightly different take on it and we’re all going to be listening for different things, and, when we do sit down to compare notes, this is going to be helpful.’ But there were other sessions we could be in.”
To be clear, there is no wrong way to attend an annual meeting. But like knowing which nurse shepherds a smoother discharge, there’s always a way to do it better. Tips from Dr. Pistoria and HM12 course director Jeff Glasheen, MD, SFHM, include:
—Jeff Glasheen, MD, SFHM, HM12 course director
- Prepare. Set up at least a basic schedule or pick out a few sessions to sit in on before arriving at HM12, or you risk trying to build a successful meeting on the fly. “I would treat this much like you would your first semester of college,” Dr. Glasheen says. “You wouldn’t just show up and see what course you wanted to go to. You’d spend some time prior to showing up....If you don’t have a game plan, you’re going to end up missing out on something you want to learn.”
- Go where you friends don’t. As Dr. Pistoria attests, it’s a natural tendency to want to attend sessions with colleagues and critique together. However, this is a once-a-year opportunity. Attend different sessions and compare notes.
- Attend the keynote addresses. This year’s lineup features a national election analyst for “CBS News,” the chief medical officer of the Centers for Medicare & Medicaid Services (CMS), and the incoming chair of the American Board of Internal Medicine (ABIM). Between them, there probably are a few good nuggets to glean.
- Attend the special-interest forums. SHM holds a series of small-group sessions focused on such hyperlocal topics as rural HM and health information technology (HIT), among others. Society staff and leadership take notes and let attendees drive the conversation.
- Network, network, network. Everyone had that first meeting where they didn’t know who was who, so feel free to introduce yourself to anybody. Get business cards from everybody. And hit the hotel hotspots armed with questions and a willingness to buy a potential new relationship a drink.
- “There’s a tremendous willingness to help new people, to answer questions, to have the hallway questions, the conversations that occur at 11 o’clock at night at the bar,” Dr. Pistoria says. “If you see somebody and you say, ‘Hey, you know, I was in your session earlier, can I ask you a couple of follow-up questions?’ People are going to say, ‘Hell yes, sit down. Let’s talk.’ If people remember that and aren’t shy, I think people really can maximize the potential benefit.”
- Share what you learn. Start a quality initiative or talk with your C-suite about starting a project. Email some of your new contacts to start a dialogue. Don’t go home, give one brown-bag session to your colleagues, and wait until next year’s annual meeting to think about the “big picture” again.
“It’s easy to get back home and fall right back into the patterns you were doing before,” Dr. Glasheen says. “If you get excited by something at the annual meeting, go back home and really work at putting that into place.”
Richard Quinn is a freelance writer in New Jersey.
To get involved, visit www.hospitalmedicine2012.org/schedule
Policy Experts Say Hospital Medicine Should be Ready to Tackle Reform Challenges

In a restaurant, it’s called being in the weeds: when the duties of one’s job become so overwhelming that you can’t keep up with the pace. Think five new admissions at the end of a 12-hour workday.
That’s where Norm Ornstein, one of the keynote speakers at HM12 in San Diego, can help. A resident scholar at the American Enterprise Institute in Washington, D.C., and a longtime observer of all things political, Ornstein is in the weeds of healthcare reform on a partisan and policy level. He pens a weekly column for the Congressional newspaper Roll Call and also provides election analysis for “CBS News.” He has authored or edited multiple books, including “Intensive Care: How Congress Shapes Health Policy” and “The Permanent Campaign and Its Future.”
So hospitalists who too often feel that, between patient care and clinical research, they don’t have time to study the political landscape should probably plan to attend Ornstein’s address, tentatively dubbed “Making Health Policy in an Age of Dysfunctional Politics.” The Hospitalist spent a few moments with Ornstein as he prepared for his HM12 address.
What do you plan to speak about and what do you want hospitalists to take away from your talk?
We’re really going to be looking toward the fall matchup in the presidential campaign. And we know that health policy is going to be not the No. 1 issue—it’s pretty clear now that the economy and jobs will be the No. 1 issue—but it will be following pretty closely behind at No. 2. And we know we’re going to get a very hot debate on whether we can or should repeal the Affordable Care Act (ACA). … But we also know that, repeal or not … health policy is up in the air. We’re going to go through some tumultuous changes. Everybody is on the line; who’s actually delivering services, or trying to, is going to have enormous challenges. It’s a perfect time to talk about these issues.
Healthcare professionals aren’t used to being part of the political maelstrom. What is their role in this process?
If anything, the last year or two should make it very clear to them they better be involved. … Whatever happens with the Affordable Care Act, we’re going to be making adjustments in public policy, and we’re going to be seeing massive adjustments in the private sector for years to come. Lots of people are going to be looking for the best ideas and looking for ways to make sure we can bend the cost curve, to use the cliché, but not sacrifice significantly services to people—and maybe even improve those services. It’s time, I think, for people in this world to understand it’s in their own self-interest to be engaged.
How nervous should hospitalists be that there really is a chance the ACA can be repealed?
I don’t think they should be worried that the whole kit and caboodle will be replaced. I think they should be concerned that we will see a combination of some elements of it perhaps repealed, but even more that the corrosive nature of our politics is such that Republicans, if they can’t repeal it, will do everything they can to bollocks up its implementation so that they can both score political points but also say, “See, we told you so.” This would be a challenge under the best of circumstances to make this work. But I think everybody has to be braced for what I think will be a series of some substantial bumps and jolts in the road along the way.
That is a lot of uncertainty for a hospitalist. How can they prepare?
I don’t think one can prepare adequately for the changes that are going to take place. What hospitalists have to do first is to make sure that they fulfill their own roles in caring for patients, but they should also be thinking about innovative approaches and ways of delivering services that are good for patents but also good for the system.
Is that enough—being at the vanguard of care delivery?
No, and I can’t give people assurances that there is any specific thing they can do that will make things work, or work better, because we’re moving into an uncertain environment—an uncertain environment in the real world where we’re going to see health as a share of GDP probably continue to go up for a while, but there will be some pushback against that; uncertainty as we try to integrate the public and private halves of our healthcare system a little bit better than we have; uncertainty as we find that the fiscal realities of America mean that you’ve got to put even more of a squeeze on Medicare, Medicaid, and even veterans’ health. Those things don’t happen in isolation.
Should doctors see this as an exciting time?
I think there is a bright side to this, which is there really is an opportunity here for innovation in ways to fulfill their oaths. There is an opportunity to find ways to provide better healthcare for people, better services to make their lives better.
Richard Quinn is a freelance writer in New Jersey.
To get involved, visit www.hospitalmedicine.org/advocacy
In a restaurant, it’s called being in the weeds: when the duties of one’s job become so overwhelming that you can’t keep up with the pace. Think five new admissions at the end of a 12-hour workday.
That’s where Norm Ornstein, one of the keynote speakers at HM12 in San Diego, can help. A resident scholar at the American Enterprise Institute in Washington, D.C., and a longtime observer of all things political, Ornstein is in the weeds of healthcare reform on a partisan and policy level. He pens a weekly column for the Congressional newspaper Roll Call and also provides election analysis for “CBS News.” He has authored or edited multiple books, including “Intensive Care: How Congress Shapes Health Policy” and “The Permanent Campaign and Its Future.”
So hospitalists who too often feel that, between patient care and clinical research, they don’t have time to study the political landscape should probably plan to attend Ornstein’s address, tentatively dubbed “Making Health Policy in an Age of Dysfunctional Politics.” The Hospitalist spent a few moments with Ornstein as he prepared for his HM12 address.
What do you plan to speak about and what do you want hospitalists to take away from your talk?
We’re really going to be looking toward the fall matchup in the presidential campaign. And we know that health policy is going to be not the No. 1 issue—it’s pretty clear now that the economy and jobs will be the No. 1 issue—but it will be following pretty closely behind at No. 2. And we know we’re going to get a very hot debate on whether we can or should repeal the Affordable Care Act (ACA). … But we also know that, repeal or not … health policy is up in the air. We’re going to go through some tumultuous changes. Everybody is on the line; who’s actually delivering services, or trying to, is going to have enormous challenges. It’s a perfect time to talk about these issues.
Healthcare professionals aren’t used to being part of the political maelstrom. What is their role in this process?
If anything, the last year or two should make it very clear to them they better be involved. … Whatever happens with the Affordable Care Act, we’re going to be making adjustments in public policy, and we’re going to be seeing massive adjustments in the private sector for years to come. Lots of people are going to be looking for the best ideas and looking for ways to make sure we can bend the cost curve, to use the cliché, but not sacrifice significantly services to people—and maybe even improve those services. It’s time, I think, for people in this world to understand it’s in their own self-interest to be engaged.
How nervous should hospitalists be that there really is a chance the ACA can be repealed?
I don’t think they should be worried that the whole kit and caboodle will be replaced. I think they should be concerned that we will see a combination of some elements of it perhaps repealed, but even more that the corrosive nature of our politics is such that Republicans, if they can’t repeal it, will do everything they can to bollocks up its implementation so that they can both score political points but also say, “See, we told you so.” This would be a challenge under the best of circumstances to make this work. But I think everybody has to be braced for what I think will be a series of some substantial bumps and jolts in the road along the way.
That is a lot of uncertainty for a hospitalist. How can they prepare?
I don’t think one can prepare adequately for the changes that are going to take place. What hospitalists have to do first is to make sure that they fulfill their own roles in caring for patients, but they should also be thinking about innovative approaches and ways of delivering services that are good for patents but also good for the system.
Is that enough—being at the vanguard of care delivery?
No, and I can’t give people assurances that there is any specific thing they can do that will make things work, or work better, because we’re moving into an uncertain environment—an uncertain environment in the real world where we’re going to see health as a share of GDP probably continue to go up for a while, but there will be some pushback against that; uncertainty as we try to integrate the public and private halves of our healthcare system a little bit better than we have; uncertainty as we find that the fiscal realities of America mean that you’ve got to put even more of a squeeze on Medicare, Medicaid, and even veterans’ health. Those things don’t happen in isolation.
Should doctors see this as an exciting time?
I think there is a bright side to this, which is there really is an opportunity here for innovation in ways to fulfill their oaths. There is an opportunity to find ways to provide better healthcare for people, better services to make their lives better.
Richard Quinn is a freelance writer in New Jersey.
To get involved, visit www.hospitalmedicine.org/advocacy
In a restaurant, it’s called being in the weeds: when the duties of one’s job become so overwhelming that you can’t keep up with the pace. Think five new admissions at the end of a 12-hour workday.
That’s where Norm Ornstein, one of the keynote speakers at HM12 in San Diego, can help. A resident scholar at the American Enterprise Institute in Washington, D.C., and a longtime observer of all things political, Ornstein is in the weeds of healthcare reform on a partisan and policy level. He pens a weekly column for the Congressional newspaper Roll Call and also provides election analysis for “CBS News.” He has authored or edited multiple books, including “Intensive Care: How Congress Shapes Health Policy” and “The Permanent Campaign and Its Future.”
So hospitalists who too often feel that, between patient care and clinical research, they don’t have time to study the political landscape should probably plan to attend Ornstein’s address, tentatively dubbed “Making Health Policy in an Age of Dysfunctional Politics.” The Hospitalist spent a few moments with Ornstein as he prepared for his HM12 address.
What do you plan to speak about and what do you want hospitalists to take away from your talk?
We’re really going to be looking toward the fall matchup in the presidential campaign. And we know that health policy is going to be not the No. 1 issue—it’s pretty clear now that the economy and jobs will be the No. 1 issue—but it will be following pretty closely behind at No. 2. And we know we’re going to get a very hot debate on whether we can or should repeal the Affordable Care Act (ACA). … But we also know that, repeal or not … health policy is up in the air. We’re going to go through some tumultuous changes. Everybody is on the line; who’s actually delivering services, or trying to, is going to have enormous challenges. It’s a perfect time to talk about these issues.
Healthcare professionals aren’t used to being part of the political maelstrom. What is their role in this process?
If anything, the last year or two should make it very clear to them they better be involved. … Whatever happens with the Affordable Care Act, we’re going to be making adjustments in public policy, and we’re going to be seeing massive adjustments in the private sector for years to come. Lots of people are going to be looking for the best ideas and looking for ways to make sure we can bend the cost curve, to use the cliché, but not sacrifice significantly services to people—and maybe even improve those services. It’s time, I think, for people in this world to understand it’s in their own self-interest to be engaged.
How nervous should hospitalists be that there really is a chance the ACA can be repealed?
I don’t think they should be worried that the whole kit and caboodle will be replaced. I think they should be concerned that we will see a combination of some elements of it perhaps repealed, but even more that the corrosive nature of our politics is such that Republicans, if they can’t repeal it, will do everything they can to bollocks up its implementation so that they can both score political points but also say, “See, we told you so.” This would be a challenge under the best of circumstances to make this work. But I think everybody has to be braced for what I think will be a series of some substantial bumps and jolts in the road along the way.
That is a lot of uncertainty for a hospitalist. How can they prepare?
I don’t think one can prepare adequately for the changes that are going to take place. What hospitalists have to do first is to make sure that they fulfill their own roles in caring for patients, but they should also be thinking about innovative approaches and ways of delivering services that are good for patents but also good for the system.
Is that enough—being at the vanguard of care delivery?
No, and I can’t give people assurances that there is any specific thing they can do that will make things work, or work better, because we’re moving into an uncertain environment—an uncertain environment in the real world where we’re going to see health as a share of GDP probably continue to go up for a while, but there will be some pushback against that; uncertainty as we try to integrate the public and private halves of our healthcare system a little bit better than we have; uncertainty as we find that the fiscal realities of America mean that you’ve got to put even more of a squeeze on Medicare, Medicaid, and even veterans’ health. Those things don’t happen in isolation.
Should doctors see this as an exciting time?
I think there is a bright side to this, which is there really is an opportunity here for innovation in ways to fulfill their oaths. There is an opportunity to find ways to provide better healthcare for people, better services to make their lives better.
Richard Quinn is a freelance writer in New Jersey.
To get involved, visit www.hospitalmedicine.org/advocacy
CME Credit at HM12
HM12 is planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Blackwell Futura Media Services (BFMS) and SHM. BFMS is accredited by ACCME to provide CME for physicians.
HM12 registration is available at www.hospitalmedicine2012.org until March 5. SHM also permits walk-up registration at the San Diego Convention Center.
BFMS designates the educational activity for SHM’s annual meeting at a maximum of 19.75 Category 1 credits toward the AMA Physician’s Recognition Award. Each physician should claim only those hours of credit they actually spend in each educational activity. BFMS has designated a credit schedule for HM12’s pre-courses on April 1 as follows:
- ABIM MOC learning session, 6.5 credits;
- Advanced Interactive Critical Care, 7.75 credits;
- CMS’s Value-Based Purchasing Program, 3.75 credits;
- Medical Procedures, 7.5 credits;
- Portable Ultrasounds, 3.75 credits;
- Perioperative Medicine, 7.75 credits; and
- Practice Management, 7.5 credits.
Source: www.hospitalmedicine.org
HM12 is planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Blackwell Futura Media Services (BFMS) and SHM. BFMS is accredited by ACCME to provide CME for physicians.
HM12 registration is available at www.hospitalmedicine2012.org until March 5. SHM also permits walk-up registration at the San Diego Convention Center.
BFMS designates the educational activity for SHM’s annual meeting at a maximum of 19.75 Category 1 credits toward the AMA Physician’s Recognition Award. Each physician should claim only those hours of credit they actually spend in each educational activity. BFMS has designated a credit schedule for HM12’s pre-courses on April 1 as follows:
- ABIM MOC learning session, 6.5 credits;
- Advanced Interactive Critical Care, 7.75 credits;
- CMS’s Value-Based Purchasing Program, 3.75 credits;
- Medical Procedures, 7.5 credits;
- Portable Ultrasounds, 3.75 credits;
- Perioperative Medicine, 7.75 credits; and
- Practice Management, 7.5 credits.
Source: www.hospitalmedicine.org
HM12 is planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of Blackwell Futura Media Services (BFMS) and SHM. BFMS is accredited by ACCME to provide CME for physicians.
HM12 registration is available at www.hospitalmedicine2012.org until March 5. SHM also permits walk-up registration at the San Diego Convention Center.
BFMS designates the educational activity for SHM’s annual meeting at a maximum of 19.75 Category 1 credits toward the AMA Physician’s Recognition Award. Each physician should claim only those hours of credit they actually spend in each educational activity. BFMS has designated a credit schedule for HM12’s pre-courses on April 1 as follows:
- ABIM MOC learning session, 6.5 credits;
- Advanced Interactive Critical Care, 7.75 credits;
- CMS’s Value-Based Purchasing Program, 3.75 credits;
- Medical Procedures, 7.5 credits;
- Portable Ultrasounds, 3.75 credits;
- Perioperative Medicine, 7.75 credits; and
- Practice Management, 7.5 credits.
Source: www.hospitalmedicine.org
HM12 Organizers Strive for ‘Meaningful’ Educational Offerings for Hospitalists

Jeff Glasheen, MD, SFHM, has been going to SHM’s annual meetings for a decade. He’s played the part of poster presenter, session leader, physician editor of The Hospitalist, and even just a healthcare consumer eager to hear what a keynote speaker has to say.
This year, he’s added a new title: HM12 course director. The sobriquet has given him a new appreciation for the work that goes into the four-day summit, April 1-4 at the San Diego Convention Center.
“It’s been a great experience to see how much work really goes into these meetings behind the scenes and how thoughtful people are to try to program content that all different types of hospitalists would be interested in,” says Dr. Glasheen, associate professor of medicine and director of the hospital medicine group at the University of Colorado Denver. “Trying to target enough stuff so that it’s meaningful for everybody ends up being incredibly challenging.”
The challenge is important because continuing medical education (CME) arguably is the biggest draw for the annual meeting. From pre-courses offering Category 1 credits toward the AMA Physician’s Recognition Award to rapid-fire sessions offering “Jeopardy!”-like chances to test current knowledge, a majority of past attendees say CME and pedagogy keep them coming back.
“It’s one of the top reasons people come, and it should be,” Dr. Glasheen adds. “This is the opportunity for people to come and hear new ideas. And I don’t mean that just in terms of clinical medicine, but also nonclinical medicine. This is our opportunity to pull ourselves out of the weeds … and really get a sense of what’s coming down the pike.”
Dr. Glasheen and assistant course director Michael Pistoria, DO, FACP, SFHM, say the goals of each year’s offerings are to keep things current and user-friendly.
—Jeff Glasheen, MD, SFHM, HM12 course director
Take “How to Improve Performance in CMS’s Value-Based Purchasing Program,” a debut pre-course designed as a primer for the new VBP rules going into effect Oct. 1. The session is led by SHM’s senior vice president and chief solutions officer Joseph Miller and Patrick Torcson, MD, MMM, FACP, SFHM, director of hospital medicine at St. Tammany Parish Hospital in Covington, La. The new pre-course joins the now well-established American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) course as one of the sessions that, although they didn’t exist a few years ago, are viewed as crucial to the specialty’s future development.
“It’s the natural evolution of what hospitalists do,” Dr. Glasheen says. “If we went back to the first year of this meeting, it was primarily a clinical meeting. But I think over time, just as my role as a hospitalist has evolved over 10 years, so has the society’s annual meeting. Yes, we have the clinical core that everybody needs. But there’s a lot of other stuff that’s happening in the world around us—including healthcare policy, payment reform—and we need to know about those things.”
Constant change to the HM12 course menu keeps things fresh, says Dr. Pistoria, HM13’s course director, who works at Lehigh Valley Health Network in Allentown, Pa. “Quite frankly, it allows us to some degree to keep the faculty fresh as well,” he says. “If you give them a year off, they come back fully charged with new ideas. Even if it’s the same information, maybe they’ve got some new ideas of how to present it.”
Another area where the importance of the meeting’s educational offerings becomes self-evident is the Research, Innovations, and Clinical Vignettes (RIV) poster competition. The popularity of the competition continues to grow; the review committee was deluged with 200 more submissions for HM12 than for HM11. Organizers felt that was too many posters to give attendees enough quality time with their presenters, so the session has been expanded and broken up into two sessions—one for Research and Innovations (Monday, April 2, 5-7 p.m.), and one for Vignettes (Tuesday, April 3, noon-1:30 p.m.).
“It speaks to the fact that academic hospital medicine is really growing up,” Dr. Glasheen says. “Ten years ago, we were all just trying to get enough docs to take care of patients. Now we’re getting to the point where academic hospitalists really can develop a career as a scholar and a researcher.”
An educational twist to this year’s meeting is an approach called “Pathways.” The tack is an online map of interrelated courses that may appear in different categorical tracks. For example, the “pathway” highlights for attendees how they can find sessions devoted to early-career hospitalist issues, palliative care, or transitions of care. So if two people from one institution wanted to break up the sessions by a topic, they now have an easier way.
“It affords people the opportunity to plan,” Dr. Pistoria says. “And again, it keeps us fresh. As the annual meeting committee, we’re constantly looking: What can we do what can we do differently? What can we do better?”
Richard Quinn is a freelance writer in New Jersey.
Jeff Glasheen, MD, SFHM, has been going to SHM’s annual meetings for a decade. He’s played the part of poster presenter, session leader, physician editor of The Hospitalist, and even just a healthcare consumer eager to hear what a keynote speaker has to say.
This year, he’s added a new title: HM12 course director. The sobriquet has given him a new appreciation for the work that goes into the four-day summit, April 1-4 at the San Diego Convention Center.
“It’s been a great experience to see how much work really goes into these meetings behind the scenes and how thoughtful people are to try to program content that all different types of hospitalists would be interested in,” says Dr. Glasheen, associate professor of medicine and director of the hospital medicine group at the University of Colorado Denver. “Trying to target enough stuff so that it’s meaningful for everybody ends up being incredibly challenging.”
The challenge is important because continuing medical education (CME) arguably is the biggest draw for the annual meeting. From pre-courses offering Category 1 credits toward the AMA Physician’s Recognition Award to rapid-fire sessions offering “Jeopardy!”-like chances to test current knowledge, a majority of past attendees say CME and pedagogy keep them coming back.
“It’s one of the top reasons people come, and it should be,” Dr. Glasheen adds. “This is the opportunity for people to come and hear new ideas. And I don’t mean that just in terms of clinical medicine, but also nonclinical medicine. This is our opportunity to pull ourselves out of the weeds … and really get a sense of what’s coming down the pike.”
Dr. Glasheen and assistant course director Michael Pistoria, DO, FACP, SFHM, say the goals of each year’s offerings are to keep things current and user-friendly.
—Jeff Glasheen, MD, SFHM, HM12 course director
Take “How to Improve Performance in CMS’s Value-Based Purchasing Program,” a debut pre-course designed as a primer for the new VBP rules going into effect Oct. 1. The session is led by SHM’s senior vice president and chief solutions officer Joseph Miller and Patrick Torcson, MD, MMM, FACP, SFHM, director of hospital medicine at St. Tammany Parish Hospital in Covington, La. The new pre-course joins the now well-established American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) course as one of the sessions that, although they didn’t exist a few years ago, are viewed as crucial to the specialty’s future development.
“It’s the natural evolution of what hospitalists do,” Dr. Glasheen says. “If we went back to the first year of this meeting, it was primarily a clinical meeting. But I think over time, just as my role as a hospitalist has evolved over 10 years, so has the society’s annual meeting. Yes, we have the clinical core that everybody needs. But there’s a lot of other stuff that’s happening in the world around us—including healthcare policy, payment reform—and we need to know about those things.”
Constant change to the HM12 course menu keeps things fresh, says Dr. Pistoria, HM13’s course director, who works at Lehigh Valley Health Network in Allentown, Pa. “Quite frankly, it allows us to some degree to keep the faculty fresh as well,” he says. “If you give them a year off, they come back fully charged with new ideas. Even if it’s the same information, maybe they’ve got some new ideas of how to present it.”
Another area where the importance of the meeting’s educational offerings becomes self-evident is the Research, Innovations, and Clinical Vignettes (RIV) poster competition. The popularity of the competition continues to grow; the review committee was deluged with 200 more submissions for HM12 than for HM11. Organizers felt that was too many posters to give attendees enough quality time with their presenters, so the session has been expanded and broken up into two sessions—one for Research and Innovations (Monday, April 2, 5-7 p.m.), and one for Vignettes (Tuesday, April 3, noon-1:30 p.m.).
“It speaks to the fact that academic hospital medicine is really growing up,” Dr. Glasheen says. “Ten years ago, we were all just trying to get enough docs to take care of patients. Now we’re getting to the point where academic hospitalists really can develop a career as a scholar and a researcher.”
An educational twist to this year’s meeting is an approach called “Pathways.” The tack is an online map of interrelated courses that may appear in different categorical tracks. For example, the “pathway” highlights for attendees how they can find sessions devoted to early-career hospitalist issues, palliative care, or transitions of care. So if two people from one institution wanted to break up the sessions by a topic, they now have an easier way.
“It affords people the opportunity to plan,” Dr. Pistoria says. “And again, it keeps us fresh. As the annual meeting committee, we’re constantly looking: What can we do what can we do differently? What can we do better?”
Richard Quinn is a freelance writer in New Jersey.
Jeff Glasheen, MD, SFHM, has been going to SHM’s annual meetings for a decade. He’s played the part of poster presenter, session leader, physician editor of The Hospitalist, and even just a healthcare consumer eager to hear what a keynote speaker has to say.
This year, he’s added a new title: HM12 course director. The sobriquet has given him a new appreciation for the work that goes into the four-day summit, April 1-4 at the San Diego Convention Center.
“It’s been a great experience to see how much work really goes into these meetings behind the scenes and how thoughtful people are to try to program content that all different types of hospitalists would be interested in,” says Dr. Glasheen, associate professor of medicine and director of the hospital medicine group at the University of Colorado Denver. “Trying to target enough stuff so that it’s meaningful for everybody ends up being incredibly challenging.”
The challenge is important because continuing medical education (CME) arguably is the biggest draw for the annual meeting. From pre-courses offering Category 1 credits toward the AMA Physician’s Recognition Award to rapid-fire sessions offering “Jeopardy!”-like chances to test current knowledge, a majority of past attendees say CME and pedagogy keep them coming back.
“It’s one of the top reasons people come, and it should be,” Dr. Glasheen adds. “This is the opportunity for people to come and hear new ideas. And I don’t mean that just in terms of clinical medicine, but also nonclinical medicine. This is our opportunity to pull ourselves out of the weeds … and really get a sense of what’s coming down the pike.”
Dr. Glasheen and assistant course director Michael Pistoria, DO, FACP, SFHM, say the goals of each year’s offerings are to keep things current and user-friendly.
—Jeff Glasheen, MD, SFHM, HM12 course director
Take “How to Improve Performance in CMS’s Value-Based Purchasing Program,” a debut pre-course designed as a primer for the new VBP rules going into effect Oct. 1. The session is led by SHM’s senior vice president and chief solutions officer Joseph Miller and Patrick Torcson, MD, MMM, FACP, SFHM, director of hospital medicine at St. Tammany Parish Hospital in Covington, La. The new pre-course joins the now well-established American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) course as one of the sessions that, although they didn’t exist a few years ago, are viewed as crucial to the specialty’s future development.
“It’s the natural evolution of what hospitalists do,” Dr. Glasheen says. “If we went back to the first year of this meeting, it was primarily a clinical meeting. But I think over time, just as my role as a hospitalist has evolved over 10 years, so has the society’s annual meeting. Yes, we have the clinical core that everybody needs. But there’s a lot of other stuff that’s happening in the world around us—including healthcare policy, payment reform—and we need to know about those things.”
Constant change to the HM12 course menu keeps things fresh, says Dr. Pistoria, HM13’s course director, who works at Lehigh Valley Health Network in Allentown, Pa. “Quite frankly, it allows us to some degree to keep the faculty fresh as well,” he says. “If you give them a year off, they come back fully charged with new ideas. Even if it’s the same information, maybe they’ve got some new ideas of how to present it.”
Another area where the importance of the meeting’s educational offerings becomes self-evident is the Research, Innovations, and Clinical Vignettes (RIV) poster competition. The popularity of the competition continues to grow; the review committee was deluged with 200 more submissions for HM12 than for HM11. Organizers felt that was too many posters to give attendees enough quality time with their presenters, so the session has been expanded and broken up into two sessions—one for Research and Innovations (Monday, April 2, 5-7 p.m.), and one for Vignettes (Tuesday, April 3, noon-1:30 p.m.).
“It speaks to the fact that academic hospital medicine is really growing up,” Dr. Glasheen says. “Ten years ago, we were all just trying to get enough docs to take care of patients. Now we’re getting to the point where academic hospitalists really can develop a career as a scholar and a researcher.”
An educational twist to this year’s meeting is an approach called “Pathways.” The tack is an online map of interrelated courses that may appear in different categorical tracks. For example, the “pathway” highlights for attendees how they can find sessions devoted to early-career hospitalist issues, palliative care, or transitions of care. So if two people from one institution wanted to break up the sessions by a topic, they now have an easier way.
“It affords people the opportunity to plan,” Dr. Pistoria says. “And again, it keeps us fresh. As the annual meeting committee, we’re constantly looking: What can we do what can we do differently? What can we do better?”
Richard Quinn is a freelance writer in New Jersey.
HM12’s Host City of San Diego Offers Plenty of Fun Things to Do
Clinical updates, plenary addresses from D.C. heavyweights, and special-interest forums—sure, those are necessary parts of SHM’s annual meeting in San Diego.
But a local hospitalist’s favorite restaurant? That’s downright important.
“You know, I’d have to say my son and I’s is Casa Guadalajara in Old Town,” says Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego. “He loves the bean burritos. It’s sort of a slower pace, so when you go, it’s going to take some time, but the food’s really good.”
HM12 is a perfect chance to learn about San Diego. (Did you know it is the eighth-largest city in the U.S., with 1.3 million residents?) San Diego offers a plethora of attractions for those with time to explore, and the San Diego Convention Center’s location—along San Diego Bay—is a big reason why (as is the average high temperature: 68 degrees in April). Hospitalists and their families will be within walking distance of:
- The Gaslamp Quarter, a national historic district and entertainment destination. The trendy neighborhood offers scores of dining options, from elbows-on-the-table relaxation to white-linen prix fixe.
- Petco Park, the baseball stadium for the San Diego Padres. The team plays its home opener on April 4, the start of a four-game series with the rival Los Angeles Dodgers.
- Just north of the village are two museums of note for sailors: the USS Midway Museum and the Maritime Museum of San Diego. The USS Midway offers tours of an aircraft carrier; MMSD visitors experience the world’s oldest active ship, the Star of India.
- Coronado: A ferry brings visitors and locals alike to a luxury resort area whose name in Spanish means “the crowned one.” Sometimes called Coronado Island—though the land mass is technically a peninsula—visitors can rent bikes to tour its streets. A particular highlight is Hotel Del Coronado, built in 1888 and now a historic landmark. The property has been featured in major motion pictures, including the Marilyn Monroe classic “Some Like it Hot.”
—Pedro Ramos, MD, assistant clinical professor of medicine, University of California at San Diego
And that’s just the pedestrian-friendly parts of the city. Board a trolley, a pedi-cab, or a light-rail train, and Dr. Ramos says a few other jewels are a few minutes away.
First up is Old Town San Diego, where Dr. Ramos and his son go for those burritos. The neighborhood is a mix of historic buildings, eateries, and two of the city’s best-known recreation areas: Old Town San Diego State Historic Park and Presidio Park.
Second, and perhaps more prized to Dr. Ramos, is the city’s namesake zoo and its environs. “It’s a short cab ride away,” he says, “and it’s connected to Balboa Park, which has these great museums, a huge park, lots of beautiful things to see there.”
To get involved, visit www.hospitalmedicine2012.org/family_activities
Clinical updates, plenary addresses from D.C. heavyweights, and special-interest forums—sure, those are necessary parts of SHM’s annual meeting in San Diego.
But a local hospitalist’s favorite restaurant? That’s downright important.
“You know, I’d have to say my son and I’s is Casa Guadalajara in Old Town,” says Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego. “He loves the bean burritos. It’s sort of a slower pace, so when you go, it’s going to take some time, but the food’s really good.”
HM12 is a perfect chance to learn about San Diego. (Did you know it is the eighth-largest city in the U.S., with 1.3 million residents?) San Diego offers a plethora of attractions for those with time to explore, and the San Diego Convention Center’s location—along San Diego Bay—is a big reason why (as is the average high temperature: 68 degrees in April). Hospitalists and their families will be within walking distance of:
- The Gaslamp Quarter, a national historic district and entertainment destination. The trendy neighborhood offers scores of dining options, from elbows-on-the-table relaxation to white-linen prix fixe.
- Petco Park, the baseball stadium for the San Diego Padres. The team plays its home opener on April 4, the start of a four-game series with the rival Los Angeles Dodgers.
- Just north of the village are two museums of note for sailors: the USS Midway Museum and the Maritime Museum of San Diego. The USS Midway offers tours of an aircraft carrier; MMSD visitors experience the world’s oldest active ship, the Star of India.
- Coronado: A ferry brings visitors and locals alike to a luxury resort area whose name in Spanish means “the crowned one.” Sometimes called Coronado Island—though the land mass is technically a peninsula—visitors can rent bikes to tour its streets. A particular highlight is Hotel Del Coronado, built in 1888 and now a historic landmark. The property has been featured in major motion pictures, including the Marilyn Monroe classic “Some Like it Hot.”
—Pedro Ramos, MD, assistant clinical professor of medicine, University of California at San Diego
And that’s just the pedestrian-friendly parts of the city. Board a trolley, a pedi-cab, or a light-rail train, and Dr. Ramos says a few other jewels are a few minutes away.
First up is Old Town San Diego, where Dr. Ramos and his son go for those burritos. The neighborhood is a mix of historic buildings, eateries, and two of the city’s best-known recreation areas: Old Town San Diego State Historic Park and Presidio Park.
Second, and perhaps more prized to Dr. Ramos, is the city’s namesake zoo and its environs. “It’s a short cab ride away,” he says, “and it’s connected to Balboa Park, which has these great museums, a huge park, lots of beautiful things to see there.”
To get involved, visit www.hospitalmedicine2012.org/family_activities
Clinical updates, plenary addresses from D.C. heavyweights, and special-interest forums—sure, those are necessary parts of SHM’s annual meeting in San Diego.
But a local hospitalist’s favorite restaurant? That’s downright important.
“You know, I’d have to say my son and I’s is Casa Guadalajara in Old Town,” says Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego. “He loves the bean burritos. It’s sort of a slower pace, so when you go, it’s going to take some time, but the food’s really good.”
HM12 is a perfect chance to learn about San Diego. (Did you know it is the eighth-largest city in the U.S., with 1.3 million residents?) San Diego offers a plethora of attractions for those with time to explore, and the San Diego Convention Center’s location—along San Diego Bay—is a big reason why (as is the average high temperature: 68 degrees in April). Hospitalists and their families will be within walking distance of:
- The Gaslamp Quarter, a national historic district and entertainment destination. The trendy neighborhood offers scores of dining options, from elbows-on-the-table relaxation to white-linen prix fixe.
- Petco Park, the baseball stadium for the San Diego Padres. The team plays its home opener on April 4, the start of a four-game series with the rival Los Angeles Dodgers.
- Just north of the village are two museums of note for sailors: the USS Midway Museum and the Maritime Museum of San Diego. The USS Midway offers tours of an aircraft carrier; MMSD visitors experience the world’s oldest active ship, the Star of India.
- Coronado: A ferry brings visitors and locals alike to a luxury resort area whose name in Spanish means “the crowned one.” Sometimes called Coronado Island—though the land mass is technically a peninsula—visitors can rent bikes to tour its streets. A particular highlight is Hotel Del Coronado, built in 1888 and now a historic landmark. The property has been featured in major motion pictures, including the Marilyn Monroe classic “Some Like it Hot.”
—Pedro Ramos, MD, assistant clinical professor of medicine, University of California at San Diego
And that’s just the pedestrian-friendly parts of the city. Board a trolley, a pedi-cab, or a light-rail train, and Dr. Ramos says a few other jewels are a few minutes away.
First up is Old Town San Diego, where Dr. Ramos and his son go for those burritos. The neighborhood is a mix of historic buildings, eateries, and two of the city’s best-known recreation areas: Old Town San Diego State Historic Park and Presidio Park.
Second, and perhaps more prized to Dr. Ramos, is the city’s namesake zoo and its environs. “It’s a short cab ride away,” he says, “and it’s connected to Balboa Park, which has these great museums, a huge park, lots of beautiful things to see there.”
To get involved, visit www.hospitalmedicine2012.org/family_activities
Wachter to Examine ‘Great Physicians’ at HM12
Let’s face it: Robert Wachter, MD, MHM, has a way with words.
The man who co-dubbed the term “hospitalist” has used his vocabulary wisely in his career, from his day jobs as professor and chief of the Division of Hospital Medicine and chief of the medical service at the University of California at San Francisco Medical Center to his appointment as a 2012 Fulbright Scholar, which took him to London, to his nascent title of chair-elect for the American Board of Internal Medicine (ABIM).
And yet the author of the HM blog Wachter’s World (www.wachtersworld.com) might best be known for the penultimate address he delivers at SHM’s annual meeting. This year he takes center stage at the San Diego Convention Center at noon April 4, capping HM12.
So, without further adieu, Dr. Wachter, in his own words:

—Robert Wachter, MD, MHM
- On how to keep his talks fresh after nearly 15 years: “It’s increasingly a struggle. One of the things that’s fun about the hospitalist field is that we are so linked to the changes in the world of healthcare, both having to pay a lot of attention to them and, to some extent, leading them. As long as the world of healthcare changes, there’s new content.”
- On his HM12 address, “The Great Physician, Circa 2012”: How Hospitalists Must Lead Efforts to Identify and Become This New Breed”: “I’ve been thinking more and more about the role of individual physicians. Part of that is opportunistic, in that I’m becoming the chair of the ABIM in July. If you’re in charge of the largest accreditation group for doctors, certainly in the county, you have to think pretty deeply about what is good and competent, and what does a great physician look like? … That line of thinking got me to then settle on a theme for this year: What does the great physician in 2012 look like? How do we train such a person? What is the mental model for that person? And how do we ensure in our field that we are both producing those people and creating a field and a professional society that encourages them and nurtures them and ensures that we are at the cutting edge?”
- On what a great hospitalist looks like in 2012: “A great hospitalist will welcome accountability and measurement and transparency. He or she will be absolutely comfortable being a member of, and a leader of, or a nonleader of, high-functioning teams. He or she will be comfortable with working through some challenging questions about what things do I need to do versus what things can others do more effectively, or as effectively, but at a lower cost. The great hospitalist now and the great doctor in the future will recognize that delivering high-quality, safe, and patient-centric care that is agnostic about how much that case costs is no longer ethical.”
- On where HM stands in its evolution as a specialty: “I’ve talked before about our field being in its adolescence. We’re rapidly reaching the adult phase where the kind of slack you gave your kid or even your teenager for transgressions, well, no one’s going to give us anymore.
- On what leadership looks like in the face of generational healthcare reform: “We should be the canaries in the coal mine, the first ones to notice that there are important changes afoot. We’ll also be the first ones that feel pressures to change ourselves in response to these forces. And the first ones to really lead the charge. I think we saw that a decade ago, with respect to safety and quality. I think we also saw it when we embraced the importance of coordination of care and communication and teamwork.”
Let’s face it: Robert Wachter, MD, MHM, has a way with words.
The man who co-dubbed the term “hospitalist” has used his vocabulary wisely in his career, from his day jobs as professor and chief of the Division of Hospital Medicine and chief of the medical service at the University of California at San Francisco Medical Center to his appointment as a 2012 Fulbright Scholar, which took him to London, to his nascent title of chair-elect for the American Board of Internal Medicine (ABIM).
And yet the author of the HM blog Wachter’s World (www.wachtersworld.com) might best be known for the penultimate address he delivers at SHM’s annual meeting. This year he takes center stage at the San Diego Convention Center at noon April 4, capping HM12.
So, without further adieu, Dr. Wachter, in his own words:
—Robert Wachter, MD, MHM
- On how to keep his talks fresh after nearly 15 years: “It’s increasingly a struggle. One of the things that’s fun about the hospitalist field is that we are so linked to the changes in the world of healthcare, both having to pay a lot of attention to them and, to some extent, leading them. As long as the world of healthcare changes, there’s new content.”
- On his HM12 address, “The Great Physician, Circa 2012”: How Hospitalists Must Lead Efforts to Identify and Become This New Breed”: “I’ve been thinking more and more about the role of individual physicians. Part of that is opportunistic, in that I’m becoming the chair of the ABIM in July. If you’re in charge of the largest accreditation group for doctors, certainly in the county, you have to think pretty deeply about what is good and competent, and what does a great physician look like? … That line of thinking got me to then settle on a theme for this year: What does the great physician in 2012 look like? How do we train such a person? What is the mental model for that person? And how do we ensure in our field that we are both producing those people and creating a field and a professional society that encourages them and nurtures them and ensures that we are at the cutting edge?”
- On what a great hospitalist looks like in 2012: “A great hospitalist will welcome accountability and measurement and transparency. He or she will be absolutely comfortable being a member of, and a leader of, or a nonleader of, high-functioning teams. He or she will be comfortable with working through some challenging questions about what things do I need to do versus what things can others do more effectively, or as effectively, but at a lower cost. The great hospitalist now and the great doctor in the future will recognize that delivering high-quality, safe, and patient-centric care that is agnostic about how much that case costs is no longer ethical.”
- On where HM stands in its evolution as a specialty: “I’ve talked before about our field being in its adolescence. We’re rapidly reaching the adult phase where the kind of slack you gave your kid or even your teenager for transgressions, well, no one’s going to give us anymore.
- On what leadership looks like in the face of generational healthcare reform: “We should be the canaries in the coal mine, the first ones to notice that there are important changes afoot. We’ll also be the first ones that feel pressures to change ourselves in response to these forces. And the first ones to really lead the charge. I think we saw that a decade ago, with respect to safety and quality. I think we also saw it when we embraced the importance of coordination of care and communication and teamwork.”
Let’s face it: Robert Wachter, MD, MHM, has a way with words.
The man who co-dubbed the term “hospitalist” has used his vocabulary wisely in his career, from his day jobs as professor and chief of the Division of Hospital Medicine and chief of the medical service at the University of California at San Francisco Medical Center to his appointment as a 2012 Fulbright Scholar, which took him to London, to his nascent title of chair-elect for the American Board of Internal Medicine (ABIM).
And yet the author of the HM blog Wachter’s World (www.wachtersworld.com) might best be known for the penultimate address he delivers at SHM’s annual meeting. This year he takes center stage at the San Diego Convention Center at noon April 4, capping HM12.
So, without further adieu, Dr. Wachter, in his own words:
—Robert Wachter, MD, MHM
- On how to keep his talks fresh after nearly 15 years: “It’s increasingly a struggle. One of the things that’s fun about the hospitalist field is that we are so linked to the changes in the world of healthcare, both having to pay a lot of attention to them and, to some extent, leading them. As long as the world of healthcare changes, there’s new content.”
- On his HM12 address, “The Great Physician, Circa 2012”: How Hospitalists Must Lead Efforts to Identify and Become This New Breed”: “I’ve been thinking more and more about the role of individual physicians. Part of that is opportunistic, in that I’m becoming the chair of the ABIM in July. If you’re in charge of the largest accreditation group for doctors, certainly in the county, you have to think pretty deeply about what is good and competent, and what does a great physician look like? … That line of thinking got me to then settle on a theme for this year: What does the great physician in 2012 look like? How do we train such a person? What is the mental model for that person? And how do we ensure in our field that we are both producing those people and creating a field and a professional society that encourages them and nurtures them and ensures that we are at the cutting edge?”
- On what a great hospitalist looks like in 2012: “A great hospitalist will welcome accountability and measurement and transparency. He or she will be absolutely comfortable being a member of, and a leader of, or a nonleader of, high-functioning teams. He or she will be comfortable with working through some challenging questions about what things do I need to do versus what things can others do more effectively, or as effectively, but at a lower cost. The great hospitalist now and the great doctor in the future will recognize that delivering high-quality, safe, and patient-centric care that is agnostic about how much that case costs is no longer ethical.”
- On where HM stands in its evolution as a specialty: “I’ve talked before about our field being in its adolescence. We’re rapidly reaching the adult phase where the kind of slack you gave your kid or even your teenager for transgressions, well, no one’s going to give us anymore.
- On what leadership looks like in the face of generational healthcare reform: “We should be the canaries in the coal mine, the first ones to notice that there are important changes afoot. We’ll also be the first ones that feel pressures to change ourselves in response to these forces. And the first ones to really lead the charge. I think we saw that a decade ago, with respect to safety and quality. I think we also saw it when we embraced the importance of coordination of care and communication and teamwork.”
Smartphones Present Both Risks and Opportunities for Hospitalists
The near-viral adoption of smartphone technology in hospital settings has made headlines recently, raising concerns about distracted physicians, data security breaches, infection hazards from bacteria on devices, and even misplaced devices. Critics also note the problems will be multiplied as electronic health records gain traction and become even more linked with handheld devices.
Russ Cucina, MD, MS, a hospitalist and medical director of information technology at the University of California at San Francisco (UCSF) Medical Center, says these issues aren’t new, and they’ve been successfully addressed in other industries for years.
Peter J. Papadakos, MD, professor of anesthesiology, surgery, and neurosurgery at the University of Rochester in New York, wrote in Anesthesiology News in November about the dangers of “electronic distraction” from mobile devices.1 He told The New York Times: “You walk around the hospital and what you see is not funny,” in terms of professional staff texting, surfing the Web, and playing games.2 “My gut feeling is lives are in danger.”
In December, John Halamka, MD, chief information officer at Beth Israel Deaconess Medical Center in Boston and chair of the U.S. Healthcare Information Technology Standards Panel, commented on a multitasking medical mishap involving a resident who answered a text message about an upcoming party during rounds.3 He noted that BIDMC doctors and nurses at have purchased more than 1,000 iPads and 1,600 iPhones with their own funds. Because of increased risks for interruptions and inadvertent disclosure of protected health information, Dr. Halamka recommends that hospitals carefully consider best practices and implement policies and technologies to mitigate those risks.
In November, CIO.com called mobile devices “the dominant technology tool in American enterprise,” but also labeled them a “security minefield.”4 Amcom Software of Eden Prairie, Minn., recently produced a white paper, “Six Things Hospitals Need to Know about Supporting the Adoption of Smartphones,” with recommendations for integration, redundancy, and escalation in their use.5 And the Schumacher physician management group of Lafayette, La., has incorporated smartphone applications for its emergency physicians, with similar technology expected soon for its hospitalists.6
“To me, a lot of this discussion in medicine is 18 to 28 months behind the times,” Dr. Cucina says. “Perhaps it’s novel to Dr. Papadakos, but we’ve had the problem for some time. Everyone is using smartphones in the clinical environment. Everybody has one. The computers we have at work get a lot of use for personal business. It’s happening; we have arrived. Now, how are we going to deal with it?”
Other industries have placed technological or administrative limits on using company devices for personal use. At UCSF, bandwidth limits were placed on access to the online video service YouTube—with unintended consequences. “There is a lot of good clinical content on YouTube that could be used for patient education at the bedside,” Dr. Cucina admits.
Given the technological imperatives, Dr. Cucina says, it makes less sense for clinicians to carry two smartphones—“one to call your spouse, one to call up Epocrates. But if we’re all going to carry converged devices, how do we use them appropriately?” It also is important to be clear on what they do well, such as retrieving clinical information, but not inputting complex charting or expecting security, privacy, and guaranteed message delivery.
Ultimately, Dr. Cucina says, new technology brings into focus issues that have long been part of medicine. “The obligation to honor patients’ privacy goes back to Hippocrates. And we’ve had infection control issues with stethoscopes since they were invented,” he says, adding the issues—and solutions—are less technological than administrative and behavioral.
References
- Papadakos P. Electronic distraction: an unmeasured variable in modern medicine. Anesthesiology News website. Available at: http://www.anesthesiologynews.com/ViewArticle.aspx?d=Commentary&d_id=449&i=November+2011&i_id=785&a_id=19643. Accessed Jan. 14, 2012.
- Richtel M. As doctors use more devices, potential for distraction grows. The New York Times website. Available at: http://www.nytimes.com/2011/12/15/health/as-doctors-use-more-devices-potential-for-distraction-grows.html?_r=4&pagewanted=all%3Fsrc%3Dtp&smid=fb-share. Accessed Jan. 14, 2012.
- Halamka J. Order interrupted by text: multitasking mishap. AHRQ website. Available at: http://webmm.ahrq.gov/case.aspx?caseID=257. Accessed Jan. 12, 2012.
- Armerding T. In 2012, a mobile security minefield. CIO-IN website. Available at: http://www.cio.in/news/2012-mobile-security-minefield-199762011. Accessed Jan. 12, 2012.
- Six things hospitals need to know about supporting the adoption of smartphones. Amcom website. Available at: http://www.amcomsoftware.com/gwf/?id=NDMy&name=Amcom+Website_Smartphone+Adoption+WP. Accessed Jan. 11, 2012.
- Quinn R. HM embraces smartphones. The Hospitalist website. Available at: http://www.the-hospitalist.org/details/article/1418005/HM_Embraces_Smartphones.html. Accessed Jan. 14, 2012.
The near-viral adoption of smartphone technology in hospital settings has made headlines recently, raising concerns about distracted physicians, data security breaches, infection hazards from bacteria on devices, and even misplaced devices. Critics also note the problems will be multiplied as electronic health records gain traction and become even more linked with handheld devices.
Russ Cucina, MD, MS, a hospitalist and medical director of information technology at the University of California at San Francisco (UCSF) Medical Center, says these issues aren’t new, and they’ve been successfully addressed in other industries for years.
Peter J. Papadakos, MD, professor of anesthesiology, surgery, and neurosurgery at the University of Rochester in New York, wrote in Anesthesiology News in November about the dangers of “electronic distraction” from mobile devices.1 He told The New York Times: “You walk around the hospital and what you see is not funny,” in terms of professional staff texting, surfing the Web, and playing games.2 “My gut feeling is lives are in danger.”
In December, John Halamka, MD, chief information officer at Beth Israel Deaconess Medical Center in Boston and chair of the U.S. Healthcare Information Technology Standards Panel, commented on a multitasking medical mishap involving a resident who answered a text message about an upcoming party during rounds.3 He noted that BIDMC doctors and nurses at have purchased more than 1,000 iPads and 1,600 iPhones with their own funds. Because of increased risks for interruptions and inadvertent disclosure of protected health information, Dr. Halamka recommends that hospitals carefully consider best practices and implement policies and technologies to mitigate those risks.
In November, CIO.com called mobile devices “the dominant technology tool in American enterprise,” but also labeled them a “security minefield.”4 Amcom Software of Eden Prairie, Minn., recently produced a white paper, “Six Things Hospitals Need to Know about Supporting the Adoption of Smartphones,” with recommendations for integration, redundancy, and escalation in their use.5 And the Schumacher physician management group of Lafayette, La., has incorporated smartphone applications for its emergency physicians, with similar technology expected soon for its hospitalists.6
“To me, a lot of this discussion in medicine is 18 to 28 months behind the times,” Dr. Cucina says. “Perhaps it’s novel to Dr. Papadakos, but we’ve had the problem for some time. Everyone is using smartphones in the clinical environment. Everybody has one. The computers we have at work get a lot of use for personal business. It’s happening; we have arrived. Now, how are we going to deal with it?”
Other industries have placed technological or administrative limits on using company devices for personal use. At UCSF, bandwidth limits were placed on access to the online video service YouTube—with unintended consequences. “There is a lot of good clinical content on YouTube that could be used for patient education at the bedside,” Dr. Cucina admits.
Given the technological imperatives, Dr. Cucina says, it makes less sense for clinicians to carry two smartphones—“one to call your spouse, one to call up Epocrates. But if we’re all going to carry converged devices, how do we use them appropriately?” It also is important to be clear on what they do well, such as retrieving clinical information, but not inputting complex charting or expecting security, privacy, and guaranteed message delivery.
Ultimately, Dr. Cucina says, new technology brings into focus issues that have long been part of medicine. “The obligation to honor patients’ privacy goes back to Hippocrates. And we’ve had infection control issues with stethoscopes since they were invented,” he says, adding the issues—and solutions—are less technological than administrative and behavioral.
References
- Papadakos P. Electronic distraction: an unmeasured variable in modern medicine. Anesthesiology News website. Available at: http://www.anesthesiologynews.com/ViewArticle.aspx?d=Commentary&d_id=449&i=November+2011&i_id=785&a_id=19643. Accessed Jan. 14, 2012.
- Richtel M. As doctors use more devices, potential for distraction grows. The New York Times website. Available at: http://www.nytimes.com/2011/12/15/health/as-doctors-use-more-devices-potential-for-distraction-grows.html?_r=4&pagewanted=all%3Fsrc%3Dtp&smid=fb-share. Accessed Jan. 14, 2012.
- Halamka J. Order interrupted by text: multitasking mishap. AHRQ website. Available at: http://webmm.ahrq.gov/case.aspx?caseID=257. Accessed Jan. 12, 2012.
- Armerding T. In 2012, a mobile security minefield. CIO-IN website. Available at: http://www.cio.in/news/2012-mobile-security-minefield-199762011. Accessed Jan. 12, 2012.
- Six things hospitals need to know about supporting the adoption of smartphones. Amcom website. Available at: http://www.amcomsoftware.com/gwf/?id=NDMy&name=Amcom+Website_Smartphone+Adoption+WP. Accessed Jan. 11, 2012.
- Quinn R. HM embraces smartphones. The Hospitalist website. Available at: http://www.the-hospitalist.org/details/article/1418005/HM_Embraces_Smartphones.html. Accessed Jan. 14, 2012.
The near-viral adoption of smartphone technology in hospital settings has made headlines recently, raising concerns about distracted physicians, data security breaches, infection hazards from bacteria on devices, and even misplaced devices. Critics also note the problems will be multiplied as electronic health records gain traction and become even more linked with handheld devices.
Russ Cucina, MD, MS, a hospitalist and medical director of information technology at the University of California at San Francisco (UCSF) Medical Center, says these issues aren’t new, and they’ve been successfully addressed in other industries for years.
Peter J. Papadakos, MD, professor of anesthesiology, surgery, and neurosurgery at the University of Rochester in New York, wrote in Anesthesiology News in November about the dangers of “electronic distraction” from mobile devices.1 He told The New York Times: “You walk around the hospital and what you see is not funny,” in terms of professional staff texting, surfing the Web, and playing games.2 “My gut feeling is lives are in danger.”
In December, John Halamka, MD, chief information officer at Beth Israel Deaconess Medical Center in Boston and chair of the U.S. Healthcare Information Technology Standards Panel, commented on a multitasking medical mishap involving a resident who answered a text message about an upcoming party during rounds.3 He noted that BIDMC doctors and nurses at have purchased more than 1,000 iPads and 1,600 iPhones with their own funds. Because of increased risks for interruptions and inadvertent disclosure of protected health information, Dr. Halamka recommends that hospitals carefully consider best practices and implement policies and technologies to mitigate those risks.
In November, CIO.com called mobile devices “the dominant technology tool in American enterprise,” but also labeled them a “security minefield.”4 Amcom Software of Eden Prairie, Minn., recently produced a white paper, “Six Things Hospitals Need to Know about Supporting the Adoption of Smartphones,” with recommendations for integration, redundancy, and escalation in their use.5 And the Schumacher physician management group of Lafayette, La., has incorporated smartphone applications for its emergency physicians, with similar technology expected soon for its hospitalists.6
“To me, a lot of this discussion in medicine is 18 to 28 months behind the times,” Dr. Cucina says. “Perhaps it’s novel to Dr. Papadakos, but we’ve had the problem for some time. Everyone is using smartphones in the clinical environment. Everybody has one. The computers we have at work get a lot of use for personal business. It’s happening; we have arrived. Now, how are we going to deal with it?”
Other industries have placed technological or administrative limits on using company devices for personal use. At UCSF, bandwidth limits were placed on access to the online video service YouTube—with unintended consequences. “There is a lot of good clinical content on YouTube that could be used for patient education at the bedside,” Dr. Cucina admits.
Given the technological imperatives, Dr. Cucina says, it makes less sense for clinicians to carry two smartphones—“one to call your spouse, one to call up Epocrates. But if we’re all going to carry converged devices, how do we use them appropriately?” It also is important to be clear on what they do well, such as retrieving clinical information, but not inputting complex charting or expecting security, privacy, and guaranteed message delivery.
Ultimately, Dr. Cucina says, new technology brings into focus issues that have long been part of medicine. “The obligation to honor patients’ privacy goes back to Hippocrates. And we’ve had infection control issues with stethoscopes since they were invented,” he says, adding the issues—and solutions—are less technological than administrative and behavioral.
References
- Papadakos P. Electronic distraction: an unmeasured variable in modern medicine. Anesthesiology News website. Available at: http://www.anesthesiologynews.com/ViewArticle.aspx?d=Commentary&d_id=449&i=November+2011&i_id=785&a_id=19643. Accessed Jan. 14, 2012.
- Richtel M. As doctors use more devices, potential for distraction grows. The New York Times website. Available at: http://www.nytimes.com/2011/12/15/health/as-doctors-use-more-devices-potential-for-distraction-grows.html?_r=4&pagewanted=all%3Fsrc%3Dtp&smid=fb-share. Accessed Jan. 14, 2012.
- Halamka J. Order interrupted by text: multitasking mishap. AHRQ website. Available at: http://webmm.ahrq.gov/case.aspx?caseID=257. Accessed Jan. 12, 2012.
- Armerding T. In 2012, a mobile security minefield. CIO-IN website. Available at: http://www.cio.in/news/2012-mobile-security-minefield-199762011. Accessed Jan. 12, 2012.
- Six things hospitals need to know about supporting the adoption of smartphones. Amcom website. Available at: http://www.amcomsoftware.com/gwf/?id=NDMy&name=Amcom+Website_Smartphone+Adoption+WP. Accessed Jan. 11, 2012.
- Quinn R. HM embraces smartphones. The Hospitalist website. Available at: http://www.the-hospitalist.org/details/article/1418005/HM_Embraces_Smartphones.html. Accessed Jan. 14, 2012.
HHS Pushes Back ICD-10 Deadline
Hospitalists keeping an eye on the planned implementation of the 10th revision of the International Statistical Classification of Diseases coding system (ICD-10) can breathe a temporary sigh of relief: The U.S. Department of Health and Human Services (HHS) announced last week that it would delay the October 2013 start date for using the new codes. No new date was given.
The decision came after the American Medical Association (AMA) launched a public campaign to persuade Congress and HHS to delay the transition to ICD-10. SHM's AMA delegate and public policy committee member Bradley Flansbaum, DO, MPH, SFHM, says SHM took no formal position on the start date but was watching the national discussion closely.
"This is a big jump," says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. "As always with administrative procedures and the legacy systems of yesteryear, a lot of institutions are pushing back."
At issue, according to AMA leaders, is that physicians already are dealing with a litany of regulatory, technological, and coding changes tied to the national healthcare reform movement. The immediate implementation quintuples the number of billing codes to 68,000, an expansion that would be an "onslaught of overlapping regulatory mandates and reporting requirements," wrote James Madara, MD, AMA executive vice president and chief executive officer, in a letter this month to HHS Secretary Kathleen Sebilius (PDF).
"ICD-10 codes are important to many positive improvements in our healthcare system," Sebilius said in announcing the delay. "We have heard from many in the provider community who have concerns about the administrative burdens they face in the years ahead. We are committing to work with the provider community to re-examine the pace at which HHS and the nation implement these important improvements to our healthcare system."
Hospitalists keeping an eye on the planned implementation of the 10th revision of the International Statistical Classification of Diseases coding system (ICD-10) can breathe a temporary sigh of relief: The U.S. Department of Health and Human Services (HHS) announced last week that it would delay the October 2013 start date for using the new codes. No new date was given.
The decision came after the American Medical Association (AMA) launched a public campaign to persuade Congress and HHS to delay the transition to ICD-10. SHM's AMA delegate and public policy committee member Bradley Flansbaum, DO, MPH, SFHM, says SHM took no formal position on the start date but was watching the national discussion closely.
"This is a big jump," says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. "As always with administrative procedures and the legacy systems of yesteryear, a lot of institutions are pushing back."
At issue, according to AMA leaders, is that physicians already are dealing with a litany of regulatory, technological, and coding changes tied to the national healthcare reform movement. The immediate implementation quintuples the number of billing codes to 68,000, an expansion that would be an "onslaught of overlapping regulatory mandates and reporting requirements," wrote James Madara, MD, AMA executive vice president and chief executive officer, in a letter this month to HHS Secretary Kathleen Sebilius (PDF).
"ICD-10 codes are important to many positive improvements in our healthcare system," Sebilius said in announcing the delay. "We have heard from many in the provider community who have concerns about the administrative burdens they face in the years ahead. We are committing to work with the provider community to re-examine the pace at which HHS and the nation implement these important improvements to our healthcare system."
Hospitalists keeping an eye on the planned implementation of the 10th revision of the International Statistical Classification of Diseases coding system (ICD-10) can breathe a temporary sigh of relief: The U.S. Department of Health and Human Services (HHS) announced last week that it would delay the October 2013 start date for using the new codes. No new date was given.
The decision came after the American Medical Association (AMA) launched a public campaign to persuade Congress and HHS to delay the transition to ICD-10. SHM's AMA delegate and public policy committee member Bradley Flansbaum, DO, MPH, SFHM, says SHM took no formal position on the start date but was watching the national discussion closely.
"This is a big jump," says Dr. Flansbaum, director of hospitalist services at Lenox Hill Hospital in New York City. "As always with administrative procedures and the legacy systems of yesteryear, a lot of institutions are pushing back."
At issue, according to AMA leaders, is that physicians already are dealing with a litany of regulatory, technological, and coding changes tied to the national healthcare reform movement. The immediate implementation quintuples the number of billing codes to 68,000, an expansion that would be an "onslaught of overlapping regulatory mandates and reporting requirements," wrote James Madara, MD, AMA executive vice president and chief executive officer, in a letter this month to HHS Secretary Kathleen Sebilius (PDF).
"ICD-10 codes are important to many positive improvements in our healthcare system," Sebilius said in announcing the delay. "We have heard from many in the provider community who have concerns about the administrative burdens they face in the years ahead. We are committing to work with the provider community to re-examine the pace at which HHS and the nation implement these important improvements to our healthcare system."
New Studies Show Increased MI, ACS Risks in Dabigatran Patients
A pair of new studies suggest that dabigatran etexilate (Pradaxa), the first new oral anticoagulant approved in 56 years, increases the risk of myocardial infarction (MI) and acute coronary syndrome (ACS) in patients. But the author of one of the reports says the drug's benefits may be worth the risks.
"Yes, there's an increase, but that tends to be the headline," says Ken Uchino, MD, FAHA, program director of the Vascular Neurology Fellowship at the Cleveland Clinic's Cerebrovascular Center. "We have to think about the benefits and the risk balance. So far, it is favorable."
Dr. Uchino and a colleague's meta-analysis, "Dabigatran Association with Higher Risk of Acute Coronary Events," was published last month on the Archives of Internal Medicine's website. The report found dabigatran, which was approved last year, was significantly associated with a higher risk of MI or ACS when measured against multiple control groups.
A separate study, "Myocardial Ischemic Events in Patients with Atrial Fibrillation Treated with Dabigatran or Warfarin in the RE-LY Trial," published on Circulation's website, reported a nonsignificant increase in MI with dabigatran compared with warfarin, but other myocardial ischemic events were not increased.
Both reports come as the FDA evaluates post-marketing reports of serious bleeds in patients taking the drug.
Dr. Uchino believes that, taken together, the two studies are important, but more research would need to be completed to sway public opinion on whether dabigatran and other new anticoagulation therapies can unseat warfarin as the go-to treatment.
"Warfarin is such a cumbersome medication, we have all been waiting for a new medication," he adds. "So there are clear advantages to dabigatran and other newer anticoagulants. ... Our study puts us at a caution, but we should continue to gather data and continue to assess risk and benefits."
A pair of new studies suggest that dabigatran etexilate (Pradaxa), the first new oral anticoagulant approved in 56 years, increases the risk of myocardial infarction (MI) and acute coronary syndrome (ACS) in patients. But the author of one of the reports says the drug's benefits may be worth the risks.
"Yes, there's an increase, but that tends to be the headline," says Ken Uchino, MD, FAHA, program director of the Vascular Neurology Fellowship at the Cleveland Clinic's Cerebrovascular Center. "We have to think about the benefits and the risk balance. So far, it is favorable."
Dr. Uchino and a colleague's meta-analysis, "Dabigatran Association with Higher Risk of Acute Coronary Events," was published last month on the Archives of Internal Medicine's website. The report found dabigatran, which was approved last year, was significantly associated with a higher risk of MI or ACS when measured against multiple control groups.
A separate study, "Myocardial Ischemic Events in Patients with Atrial Fibrillation Treated with Dabigatran or Warfarin in the RE-LY Trial," published on Circulation's website, reported a nonsignificant increase in MI with dabigatran compared with warfarin, but other myocardial ischemic events were not increased.
Both reports come as the FDA evaluates post-marketing reports of serious bleeds in patients taking the drug.
Dr. Uchino believes that, taken together, the two studies are important, but more research would need to be completed to sway public opinion on whether dabigatran and other new anticoagulation therapies can unseat warfarin as the go-to treatment.
"Warfarin is such a cumbersome medication, we have all been waiting for a new medication," he adds. "So there are clear advantages to dabigatran and other newer anticoagulants. ... Our study puts us at a caution, but we should continue to gather data and continue to assess risk and benefits."
A pair of new studies suggest that dabigatran etexilate (Pradaxa), the first new oral anticoagulant approved in 56 years, increases the risk of myocardial infarction (MI) and acute coronary syndrome (ACS) in patients. But the author of one of the reports says the drug's benefits may be worth the risks.
"Yes, there's an increase, but that tends to be the headline," says Ken Uchino, MD, FAHA, program director of the Vascular Neurology Fellowship at the Cleveland Clinic's Cerebrovascular Center. "We have to think about the benefits and the risk balance. So far, it is favorable."
Dr. Uchino and a colleague's meta-analysis, "Dabigatran Association with Higher Risk of Acute Coronary Events," was published last month on the Archives of Internal Medicine's website. The report found dabigatran, which was approved last year, was significantly associated with a higher risk of MI or ACS when measured against multiple control groups.
A separate study, "Myocardial Ischemic Events in Patients with Atrial Fibrillation Treated with Dabigatran or Warfarin in the RE-LY Trial," published on Circulation's website, reported a nonsignificant increase in MI with dabigatran compared with warfarin, but other myocardial ischemic events were not increased.
Both reports come as the FDA evaluates post-marketing reports of serious bleeds in patients taking the drug.
Dr. Uchino believes that, taken together, the two studies are important, but more research would need to be completed to sway public opinion on whether dabigatran and other new anticoagulation therapies can unseat warfarin as the go-to treatment.
"Warfarin is such a cumbersome medication, we have all been waiting for a new medication," he adds. "So there are clear advantages to dabigatran and other newer anticoagulants. ... Our study puts us at a caution, but we should continue to gather data and continue to assess risk and benefits."